Shock Definition
Shock is a life-threatening clinical syndrome of cardiovascular collapse characterised by:
- An acute reduction of effective circulating blood volume (hypotension); and
- An inadequate perfusion of cells and tissues (hypoperfusion).
If uncompensated, these mechanisms may lead to impaired cellular metabolism, production and release of damage-associated molecular patterns (DAMPs or ‘danger signals’) and death.
Read And Learn More Homeostasis
Thus, by definition “true (or secondary) shock” is a circulatory imbalance between oxygen supply and oxygen requirements at the cellular level, and is also called as circulatory shock and is the type which is commonly referred to as ‘shock’ if not specified.
The term “Initial (or primary) shock” is used for transient and usually a benign vasovagal attack resulting from sudden reduction of venous return to the heart caused by neurogenic vasodilatation and consequent peripheral pooling of blood for example, Immediately following trauma, severe pain or emotional overreaction such as due to fear, sorrow or surprise.
Clinically, patients of primary shock suffer from the attack lasting for a few seconds or minutes and develop brief unconsciousness, weakness, sinking sensation, pale and clammy limbs, weak and rapid pulse, and low blood pressure.
Another type of shock which is not due to circulatory derangement is anaphylactic shock from a type 1 immunologic (anaphylactic) reaction.
Classification and Etiology:
Although in a given clinical case, two or more factors may be involved in causation of true shock, a simple etiologic classification of shock syndrome divides it into following 3 major types and a few other variants:
- Hypovolaemic shock: This form of shock results from inadequate circulatory blood volume by various etiologic factors that may be either from the loss of whole blood (i.e. red cell mass and plasma) from haemorrhage, or from the loss of plasma volume alone.
Classification and etiology of shock:
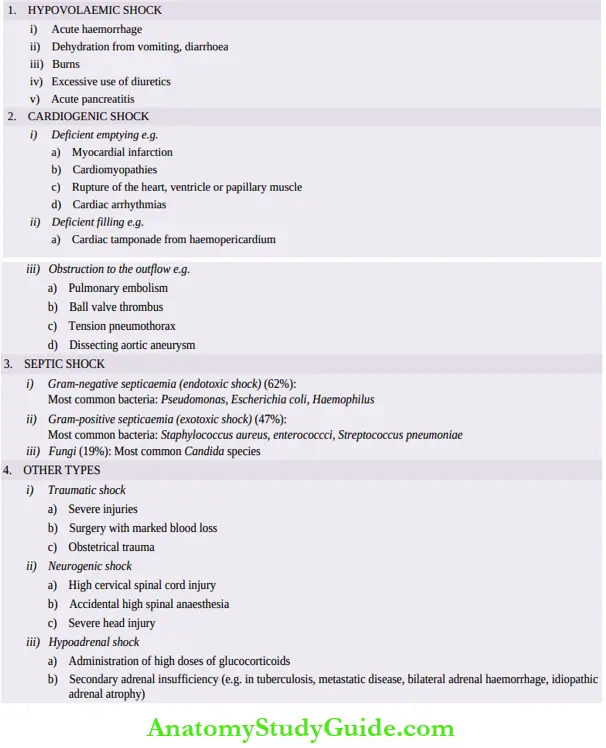
- Cardiogenic shock: Acute circulatory failure with sudden fall in cardiac output from acute diseases of the heart without actual reduction of blood volume (normovolaemia) results in cardiogenic shock.
- Septic (Toxaemic) shock: Severe bacterial infections or septicaemia induce septic shock. It may be the result of Gram-negative septicaemia (endotoxic shock), or from Gram-positive septicaemia (exotoxic shock).
- Other types: These include the following:
- Traumatic shock Shock resulting from trauma is initially due to hypovolaemia, but even after haemorrhage has been controlled, these patients continue to suffer loss of plasma volume into the interstitium of injured.
- Tissue and hence is considered separately in some descriptions.
- Neurogenic shock Neurogenic shock results from causes of interruption of sympathetic vasomotor supply.
- Hypoadrenal shock Hypoadrenal shock occurs from unknown adrenal insufficiency in which the patient fails to respond normally to the stress of trauma, surgery or illness.
Pathogenesis:
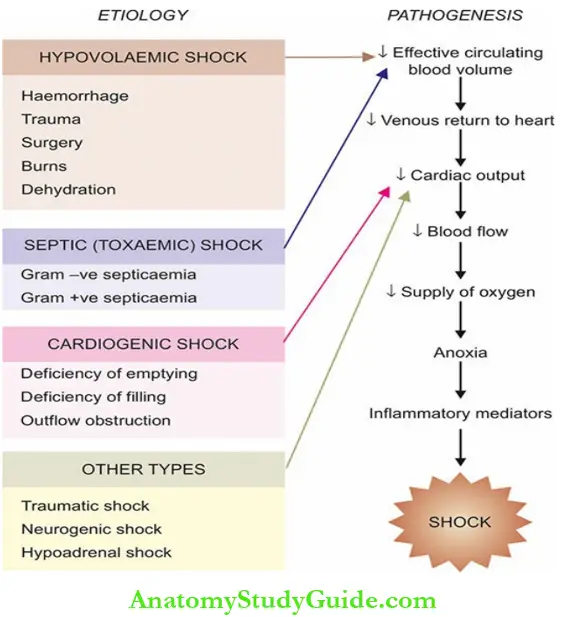
In general, all forms of shock involve the following 3 derangements:
- Reduced effective circulating blood volume.
- Reduced supply of oxygen to the cells and tissues with resultant anoxia.
- Inflammatory mediators and toxins released from shock-induced cellular injury.
These derangements initially set in compensatory mechanisms (discussed below) but eventually a vicious cycle of cell injury and severe cellular dysfunction lead to breakdown of organ function.
- Reduced effective circulating blood volume: This may result by either of the following mechanisms:
- By actual loss of blood volume as occurs in hypovolaemic shock; or
- By decreased cardiac output without actual loss of blood (normovolaemia) as occurs in cardiogenic shock and septic shock.
- Impaired tissue oxygenation: Following reduction in the effective circulating blood volume from either of the above two mechanisms and from any of the etiologic factors, there is decreased venous return to the heart resulting in decreased cardiac output.
This consequently causes reduced supply of oxygen to the organs and tissues and hence tissue anoxia occurs, which sets in cellular injury
- Release of inflammatory mediators: In response to cellular injury, innate immunity of the body gets activated as a body defense mechanism and causes release of inflammatory mediators but eventually these agents themselves become the cause of cell injury.
Endotoxins in bacterial wall in septic shock stimulate massive release of pro-inflammatory mediators (cytokines) but a similar process of release of these agents takes place in late stages of shock from other causes.
Several pro-inflammatory mediators are released from monocytes-macrophages, other leucocytes and other body cells, the most important being the tumour necrosis factor-(TNF)-α and interleukin-1 (IL-1) cytokines.
After these general comments on mechanisms in shock, features specific to pathogenesis of three major forms of shock are given below:
Pathogenesis Of Hypovolaemic Shock:
Hypovolaemic shock occurs from inadequate circulating blood volume due to various causes, most often from loss of red cell mass due to haemorrhage and, therefore, also called as haemorrhagic shock.
The major effects in this are due to decreased cardiac output and low intracardiac pressure. The severity of clinical features depends upon degree of blood volume lost.
Accordingly haemorrhagic shock is divided into four types:
- <1000 ml: Compensated
- 1000-1500 ml: Mild
- 1500-2000 ml: Moderate
- >2000 ml: Severe
Major clinical features are increased heart rate (tachycardia), low blood pressure (hypotension), low urinary output (oliguria to anuria) and alteration in mental state (agitated to confused to lethargic).
Pathogenesis Of Cardiogenic Shock:
Cardiogenic shock results from severe left ventricular dysfunction from various causes such as acute myocardial infarction.
The resultant decreased cardiac output has its effects in the form of decreased tissue perfusion and movement of fluid from pulmonary vascular bed into pulmonary interstitial space initially (interstitial pulmonary oedema) and later into alveolar spaces (alveolar pulmonary oedema).
Pathogenesis Of Septic Shock:
Septic shock results from bacterial or fungal infection. Microbes gain entry into the body from various routes, most often via respiratory tract infection; other routes are genitourinary tract, alimentary tract, or the skin.
As per studies, organisms are culture-positive in only about 70% cases of septic shock only; more frequently
Gram-negative bacteria (62%) (predominantly Pseudomonas, Escherichia coli, Haemophilus) than Gram-positive bacteria (47%) (most common organisms Staphylococcus aureus, enterococcci, Streptococcus pneumonia) and fungi (19%) (most commonly Candida species).
Many cases may have polymicrobial infection. Microbes escape immune attack by the host due to acquired deficiencies in the host defences from various factors.
Instead, microbial products set in a chain of events as under:
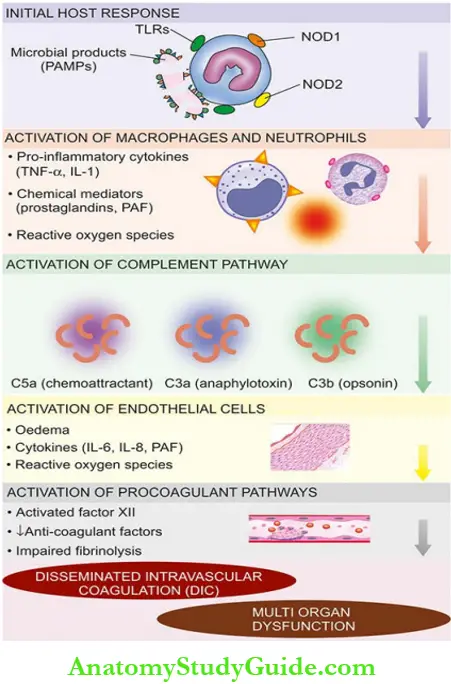
- Initial host response to microbes: Lysis of microbial cell wall releases microbe-derived molecular products, lipopolysaccharide (LPS) and bacterial peptides, into circulation; these products are called PAMPs (pathogen-associated molecular patterns).
- PAMPs are recognised by pattern-recognition receptors on the surface of the monocytes, macrophages and neutrophils as under.
-
- Toll-like receptors which bind bacterial LPS, and
- G-protein coupled receptors, and NOD1 and NOD2 (nucleotide oligmerisation domains) proteins which recognise bacterial peptides.
The complex of PAMPs-receptors transduces recognition signal to the interior of the cells that triggers the production of pro-inflammatory mechanisms and subsequent events.
- Activation of macrophages and neutrophils:
- Activation of participating cells stimulates the following:
- Pro-inflammatory cytokines, notably TNF-α and IL-1.
- Other inflammatory mediators such as HMGB-1 (high mobility group box-1) protein
- Chemical mediators of lipids such as prostaglandins and platelet-activating factor (PAF).
- Generation of reactive oxygen species
- Activation of participating cells stimulates the following:
- Activation of complement pathway:
- The cascade of complement is activated by PAMPs and forms C5a (chemoattractant), C3a (anaphylotoxin) and C3b (opsonin).
- These end-products of complement activation activate endothelial cells and further induce proinflammatory process.
- Activation of endothelial cells: Endothelial cells injured by the proinflammatory process are activated and lead to following consequences:
- Oedema due to widespread leakiness
- Release of cytokines such as IL-6, IL-8, PAF
- Production of reactive oxygen species
- Activation of procoagulant pathways:
- Coagulation pathway is activated by the following:
- Activation of factor XII by microbial products and inflammatory cytokines
- Decreased production of anti-coagulant factors by endothelial cells such as thrombomodulin and protein C
- Impaired fibrinolysis due to increased plasminogen activator inhibitor
The net result of above mechanisms is increased vascular permeability, profound peripheral vasodilatation, and pooling of blood causing hyperdynamic circulation in septic shock, in contrast to hypovolaemic and cardiogenic shock.
Reduced blood flow produces hypotension, and inadequate perfusion of cells and tissues, finally leading to organ dysfunction. Development of disseminated intravascular coagulation (DIC) with consumptive coagulopathy is an important end-result of septic shock.
Leave a Reply