Intestinal Obstruction—Special Causes
1. Adhesive Obstruction
- Firstly, strangulation should be ruled out by clinical and radiological tests. extended nonoperative therapy may be advised, for example, if one can wait for 48 hours in a case of intestinal obstruction.
- In these cases, 4–6 days of waiting is sometimes worth it, especially in a patient who has been operated many times earlier.
- During this extended period, careful monitoring is important to look for any new symptoms/signs of strangulation.
- Early postoperative adhesions (bread and butter adhesions) can also be given extended nonoperative therapy because mostly it is partial obstruction.
2. Intestinal Obstruction In Crohn’S Disease
- As far as possible, resection should be avoided in Crohn’s disease because the aim is to save as much as possible.
- 30% of patients eventually develop obstruction which requires resection.
- Again, if possible do strictureplasty
- Strictureplasty should not be done in patients with intra-abdominal abscesses or intestinal fistulae.
- Some cases of Crohn’s obstruction also respond well to medications—one more reason for nonoperative treatment.
3. Intestinal Obstruction In Pregnancy
- The commonest cause of intestinal obstruction in pregnancy and puerperium is adhesive bands.
- Volvulus is the second most common cause of intestinal obstruction—the intestine volvulates around an adhesive band and that is why the primary cause is adhesive bands
- Inguinal hernia and intussusception are the other causes.
- The consequences of intestinal obstruction in pregnancy do not differ from those found in nonpregnant women except that in the pregnant patient, a second entity, the foetus, is also threatened.
- Most of the intestinal obstructions tend to occur in the third trimester.
- Maternal mortality for intestinal obstruction in pregnancy (10–33%) is higher than in nonpregnant patients.

- In the first half of the pregnancy, nausea, vomiting and episodes of constipation are quite common. Hence, they are confused for hyperemesis gravidarum, acute duodenal ulcer and gastritis.
- In the second half of the pregnancy, symptoms can be confused for toxaemia, constipation, Braxton Hicks contractions, etc.
- Ultrasound can help in the diagnosis by detecting dilated intestinal loops, fluid in the peritoneal cavity and intussusception. It also helps to rule out ovarian torsion, gallstone disease, etc.
- Premature labour can be prevented with tocolysis (abolition of uterine contraction).
- Abdominal surgery in the third trimester does not induce labour.
- Negative laparotomy carries a small risk of disturbing the pregnancy.
- Volvulus and intussusception are the two major causes of small intestinal obstruction in pregnancy.
- Both can give rise to gangrene. Hence an intervention is required before gangrene sets in.
- The diagnosis and treatment of a pregnant patient suspected of having a bowel obstruction should be no different from those given to a nonpregnant one.
4. Ileosigmoid Knotting
It is rare type of knotting between sigmoid and ileum carrying significant mortality if not treated timely.
Ileosigmoid Knotting:
- It is also called compound volvulus.
- The predisposing factor is long pelvic mesocolon.
- The ileum twists around the sigmoid colon resulting in gangrene of the ileum or sigmoid colon or both.
- Even though the sigmoid is also twisted, features are similar to small intestinal obstruction—not massive distension as seen in sigmoid volvulus.
- Resection anastomosis of gangrenous segment followed by anastomosis of the bowel (ileoileal/colic and colocolic).
5. Iliac Crest Graft Hernia With Obstruction
- This is also a rare hernia following bone graft removal from the iliac crest for treatment of fractures.
- Iliac crest is the common donor site of bone grafts. If the bone graft removed is large, the intestines can herniate resulting in intestinal obstruction.
- Tenderness in the surgical site scar can cause diagnostic difficulty.
- It is confused for haematoma.
- CT scan gives the diagnosis.

Following is the case report of a patient who had undergone an iliac crest bone graft and developed a hernia
Intestinal Obstruction Clinical Notes:
- A 50-year-old man presented to the casualty with abdominal pain, vomiting and distension. Features were suggestive of intestinal obstruction. On examination, there was a bulge in the region of right iliac fossa—more lateral.
- There was a scar of a bone graft incision. On questioning the patient, he says that he had fractured the humerus. Two months back, nailing and bone grafting had been done.
- Ultrasound revealed bowel loops. CT scan showed a large bone graft defect with herniation of the intestines resulting in intestinal obstruction.
- Emergency surgery, reduction of hernia contents and mesh repair were done. Recovery was uneventful.
6. Food Bolus Obstruction
This complication can occur, particularly when a GJ or partial gastrectomy is done.
Factors Precipitating this Condition:
- Unmasticated, undigested particles
- Coconut pieces, jackfruit seeds gulped coins, etc.
- They get impacted in the terminal ileum which is the narrowest portion of the gut.
Treatment: Squeeze the bolus into the caecum. Otherwise, enterotomy and removal may be necessary.
7. Obstruction Due To Internal Hernia
Syn: Stammer’s Hernia:
1. These are rare causes of intestinal obstruction. Due to some congenital defect in the mesentery, the floating, mobile intestines can herniate
The defect may be in:
- Mesentery
- Transverse mesocolon or
- Broad ligament
- Foramen of Winslow
Hence, whenever a surgical procedure is done for resection of the bowel or GJ, etc. Once the anastomosis is completed, the rent in the mesocolon as in GJ or rent in the small bowel mesentery should be closed.
2. Herniation can also occur through one of the potential spaces (fossae) in and around a viscus.
Internal Hernia:
Wherever a defect is present which is an anatomically present recesses or congenital or following surgery, loop of the small intestine can herniate resulting in hernias.
- They are difficult to diagnose. The diagnosis is by exclusion.
- Triggering factors: Inflammation in the vicinity with or without an adhesion and band triggers herniation and complications.
- Most of these cases present as acute abdomen with features of intestinal obstruction.
- CT scan is the best investigation in such cases.
- It should be remembered that an important vessel runs in the close vicinity of these sites in most of cases.
- Treatment is reduction, suturing the defect or resection anastomosis if the intestine is gangrenous taking care not to damage the vessel. Decompression without dividing the constricting ring may be required
Duodenal Fossa:
- Left paraduodenal fossa: The inferior mesenteric vein lies very close to the free border here.
- Right duodenojejunal fossa: The superior mesenteric artery runs in its free border.
Colonic Fossa:
- Superior ileocaecal fossa
- Inferior ileocaecal fossa
- Sigmoid fossa
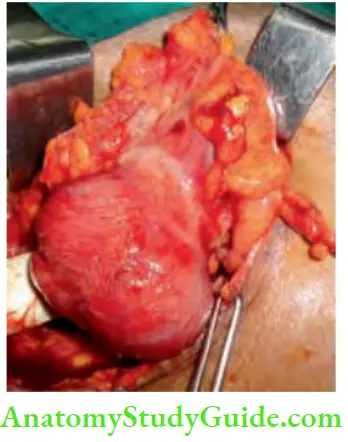
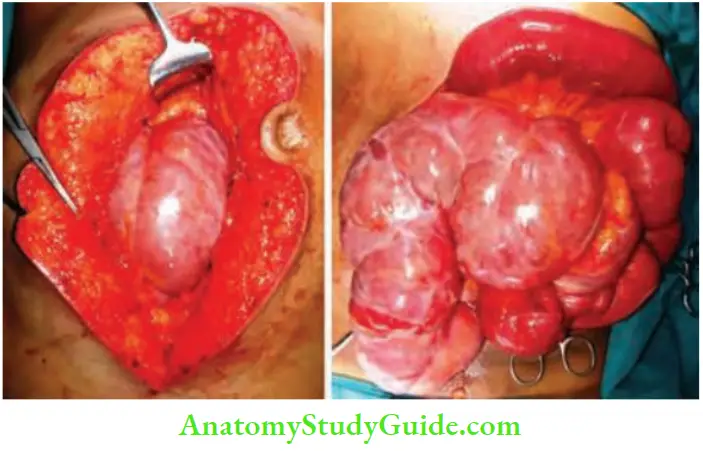
8. Abdominal Cocoon Syndrome
It is characterized by small bowel encapsulation by a fibro-collagenous membrane or “cocoon”. It is a rare cause of intestinal obstruction secondary to kinking and/or compression of the intestines within the constricting cocoon.
Three types have been recognized:
- Primary form: Primary form is probably caused by subclinical peritonitis leading to the formation of a chemical peritonitis was caused by retrograde menstruation, leading to the formation of a cocoon. This was first reported by Foo1 KT, et al. and he coined the term “abdominal cocoon” in 1978.
- Secondary: Secondary causes include the placement of Le Veen shunts for refractory ascites, continuous ambulatory peritoneal dialysis, systemic lupus erythematosus, use of povidone iodine for abdominal wash-out, an adrenergic blocker practolol, etc.
- Tuberculosis: Tuberculosis also is a factor in a few cases.
Diagnosis is established by CECT scan and treatment is separation of bowel loops and removal of the membrane in toto or in pieces.
Intestinal Obstruction Clinical Notes:
- We had a 30-year-old man with nil previous history of abdominal pain or any illness, who presented to the hospital with colicky abdominal pain, 2 times bilious vomiting and distension.
- On examination tympanitic vague mass was palpable in the right iliac fossa. X-ray was suggestive of intestinal obstruction. Abdominal ultrasonography revealed clustering of the small bowel loops in the right iliac fossa.
- CECT was reported as intestinal obstruction secondary to internal herniation. An emergency exploratory laparotomy was done. A cocoon with matted loops were found in the right iliac fossa.
- An attempt to separate the cocoon resulted in multiple tears, it was not possible, hence resection and anastomosis of about 20 cm of the ileum followed by ileocolic anastomosis was done. The patient recovered completely from obstruction and was discharged.
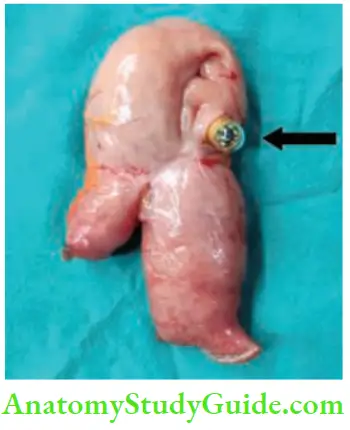
9. Capsule Obstruction
- Capsule endoscopy is done for evaluation of small intestines, major indication being occult bleeding or diarrhoea—causes can be tumours or tuberculosis or Crohn’s disease, etc.
- Capsule can get stuck at the site of ulcer or stricture or a bent intestinal loop due to adhesions. In such patients, it needs to be removed along with the intestine.
10. Acute Large Bowel Obstruction
Details about the causes of large bowel obstruction, however, a few important points have been given in Ten Commandments.
Ten Commandments While Treating Intestinal Obstruction:
- Should rule out pseudo-obstruction before exploring the abdomen.
- Should do limited contrast study or CT scan
- Should resuscitate the patient before surgery
- Should take into account, the general condition of the patient before resection anastomosis.
- Should consider right hemicolectomy or extended hemicolectomy for right-sided growth which is operable.
- Should consider single-stage resection anastomosis also for left-sided growth provided the general condition of the patient is good and on table lavage is given before the anastomosis.
- Should consider exteriorisation of gangrenous bowel in a very sick patient.
- Should consider a simple diversion colostomy in moribund patients in rectosigmoid obstructions (it is a common problem).
- Should not do anastomosis in cases with faecal contamination, peritonitis, haemodynamic instability or possible ischaemia of the remaining colonic segments.
- Should mark the probable stoma site.
Leave a Reply