Lasers in the Complete Denture
Laser is an acronym, which stands for Light Amplification by Stimulated Emission of Radiation. Lasers are an alternative to conventional surgical systems.
Table of Contents
Lasers in the complete denture Advantages
- Easy access to the anatomic site
- Possess inherent hemostatic properties.
- Capable of ablation of lesions in proximity to normal structures, with minimal damage to normal structures.
- Reduced pain during surgical procedures and less postoperative pain.
- Enhanced healing.
- Bactericidal and virucidal effects of laser result in decreased rates of wound infection.
Read And Learn More: Complete Dentures Question and Answers
Lasers in the complete denture Uses Of Lasers
- Frenectomy
Maxillary midline
Lingual (Tongue-tie). - Incisional and excisional biopsies.
- Removal of benign fibrous lesions as
- Papillous
- Pyogenic granuloma
- Lichen planus
- Erosive lichen planus
- Nicotinic stomatitis
- Verruca Vulgaris
- Inflammatory papillary hyperplasia
- Epulis.
- Soft tissue tuberosity reduction.
- Soft tissue distal wedge procedure.
- Aphthous ulcer.
- Removal of hyperkeratotic lesions.
- Removal of malignant lesions.
- Coagulation
- Graft donor sites
- Vestibuloplasty.
- Removal of vascular lesions
- Hemangioma
- Pyogenic granuloma.
- Removal of lesions in patients with hemorrhagic disorders.
- Implants pilot drill and stage II at the time of recovery.
Implant Biomaterials
Implant biomaterials The common biomaterials used are:
- Pure Titanium (In compromised bone beds CP titanium is the safest alternative)
- Titanium – 6Aluminum – 4Vanadium (Ti-6Al-4V) alloy
- Niobium
- Hydroxyapatite(calcium phosphate ceramic material)
- Hydroxyapatite-coated titanium implants
- Plasma-sprayed Ti implants
- Cobalt- chromium-Molybdenum alloy
- Iron- Chromium-Nickel based alloy
- Ceramics and carbon
- Aluminum, Titanium, and Zirconium oxides
- Calcium phosphate ceramic biomaterials
- Bioglass or Ceravital (Sodium lithium invert glasses with calcium phosphate)
- Glass-ceramics.
Implant Biomaterials Advantages of Ceramic Biomaterials Over the Other Materials
- Pure chemical composition and constituents similar to biological tissue.
- Biocompatible
- Minimal thermal and electrical conductivity
- Moduli of elasticity similar to bone
- Color similar to bone, dentin, and enamel.
Implant biomaterials Disadvantages
- Relatively low tensile and shear strength
- Limited information regarding the stability of coatings
- Low fatigue strength
- Variable solubility for different materials.
Ideally, any biomaterial that does not corrode, or abrade, is biocompatible with good strength and osseointegration properties, and with minimum thermal conductivity are good implant materials.
Geriatric Age Changes
Geriatric age changes Gerodontology
Gerodontology is dentistry for patients above 75 years of age.
Geriatric age changes Epidemiology
- Increase in the proportion of the elderly.
- Improved dental health.
Geriatric age changes Problems
- Age changes, physiological and pathological
- Disease and drug therapy
- Delivery of care.
Geriatric age changes General Aspects Of Aging
- Decreased microcirculation
- Decreased cellular production
- Decreased tissue repair
- Increased fibrosis.
Overall there is reduced function of body systems.
Geriatric age changes Oral Aspects Of Aging
- Loss of teeth: Mainly due to degeneration of periodontal structures.
- Attrition: Increases due to diet and masticatory habits.
- Oral mucosa: Loss of elasticity, dryness, atrophy, and hyperkeratosis.
- Gingiva: Edematous, thin keratinized layer, friable tissue, and loss of stippling.
- Saliva: Xerostomia due to atrophy of cells lining the intermediate ducts. Abnormal taste sensations.
- Tongue: Atrophic glossitis due to vitamin deficiency.
- Lips: Angular cheilitis due to decreased vertical dimension or vitamin B deficiency.
- Bone: Osteoporosis, excessive alveolar ridge resorption (Knife edge ridge) due to senile atrophy.
Geriatric age changes Prosthetic Problems
- Reduced adaptive capacity
- Age changes in denture-bearing areas as resorption and atrophy.
Geriatric age changes Complete Denture Construction
Geriatric age changes Impression
- If the patient was wearing an ill-fitting denture and the tissues are abused, then tissue conditioning should be done.
- An impression with maximum tissue coverage with no peripheral displacement during functional movement is to be made.
- Preliminary impressions are to be made in stock trays with final impressions in custom trays.
Geriatric age changes Vertical Dimension
- In geriatric patients, more time is needed for accurate recording of all jaw relations. An adequate interocclusal distance is required for proper mastication, phonetics, and patient comfort.
- Geriatric patients need more than 3 mm of interocclusal space. In some situations, 5 to 10 mm of space is needed.
- In cases of difficulty in recording vertical dimensions, other methods as old dentures or pre-extraction records have to be used.
- Vertical dimensions should not be opened more than 5 mm at one time.
Geriatric age changes Centric Relation
- Centric relation must be recorded at the established vertical dimension. In the case of a patient with the habitual forward position of the mandible, sufficient time should be given for the accurate jaw relation record to be registered.
- For patients with muscular incoordination muscle relaxants can be used. In geriatric patients, interocclusal wax records are favored as patients might find gothic arch tracing difficult due to many reasons.
Geriatric age changes Posterior Tooth Selection
Geriatric age changes The zero-degree tooth is highly recommended as:
- Can adapt to unusual jaw positions.
- Eliminates horizontal forces
- They adapt to negative changes in ridge height better.
Geriatric age changes Adjustments
Geriatric patients should be seen the day after insertion. No border or tooth should be reduced until sure of the problem. Home care, cleaning procedure, and oral hygiene instructions should be reinforced.
Bennett Movement and Bennett Angle
Bennett movement
It is defined as the bodily lateral movement or lateral shift of the mandible resulting from the movements of the condyles along the lateral inclines along the mandibular fossae in lateral jaw movements.
- Recorded in the region of the translating condyle of the non-working side.
- The mandible shifts 1 to 4 mm towards the working side in a lateral movement called the Bennett movement.
- If a major part of Bennett’s movement occurs in the first 4 mm, it is called distributed side shift.
Bennett Movement Factors Affecting Bennett Movement
- Shape of fossa
- Looseness of capsular ligament
- Contraction of medial pterygoids.
Bennett movement Types of Bennett movement in relation to the forward movement of the nonworking condyle
- Immediate side shift: Occurs in lateral movement before the nonworking condyles move forward (Average 0.75 mm).
- Precurrent side shift: This is the initial 2 to 3 mm of forward movement of non-working condyles.
- Progressive side shift: Lateral translation occurring beyond 2 to 3 mm of forward movement.
Bennett Movement Effects Of Bennett Movement On Cusp Paths
- Depending on the value of side shifts cusp path varies in mandibular and maxillary teeth.
- The balancing and working cusp paths in maxillary and mandibular vary with the different types of side shifts.
- Greater the side shifts, the shorter the cusps and the shallower the fossa.
- Lesser the side shift, the longer the cusp and deeper the fossa.
Bennett movement Methods of Recording Bennett Movement
- Electronic pantograph
- Polyether interocclusal records
- Mechanical pantography (Denar, Panadent)
- Simplified mandibular motion analyser.
Bennett movement Bennett angle
It is defined as the angle formed by the sagittal plane and the path of the advancing condyle during lateral mandibular movements as viewed in the horizontal plane.
- This angle is formed between the path of the non-working condyle and the sagittal plane.
- Average Bennett Angle is 7.5 to 12.8 degrees.
- In Hanau articulator, it is calculated as L = H/8 + 12.
Overjet and Overbite
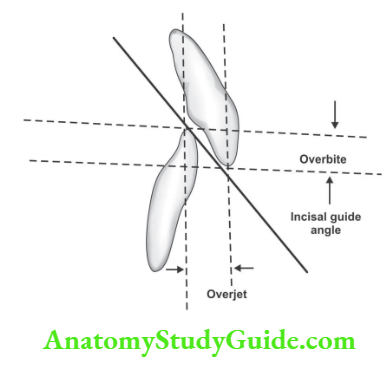
Overjet and overbite Overjet is the distance between upper and lower incisors and Overbite denotes horizontal overlap of upper and lower incisors.
Overjet and overbite Incisal guidance: is defined as, “The influence of the contacting surfaces of the mandibular and maxillary anterior teeth during mandibular movement.” –GPT
- It is usually expressed in degrees of angulation from the horizontal by a line drawn in the sagittal plane between the incisal edges of the upper and lower incisor teeth when closed in centric occlusion.
- An increase in overjet and overbite will alter the incisal guidance of occlusion.
- With a given vertical overlap incisal guide angle can be made flatter by increasing the horizontal overlap. It can be made less steep by reducing vertical overlap.
- If the incisal guidance is steep, it needs steep cusps, a steep occlusal plane, and a steep compensating curve to produce occlusal balance. Ideally, the incisal guidance should be as flat as esthetic and phonetics will permit.
- If the anterior teeth necessitate a vertical overlap, a compensating horizontal overlap should be set to prevent anterior interference from upsetting the occlusal balance on the posterior teeth.
- The increased horizontal overlap will provide freedom for the anterior teeth during normal functional and parafunctional activities. Repeated anterior interference of the teeth during mastication unstabilizes the denture bases and causes damaging effects to the anterior region of the supporting structures.
Overjet and Overbite Values
- Normal overjet and overbite values should not exceed 2 mm in the class 1 situation.
- In class 2 the overjet is more than 2 mm.
- In class 3 the overjet is less than 2 mm
Biofunctional prosthetic system (Bps)
BPS is an idea of denture prosthetics developed by Ivoclar Vivadent. This treatment concept is used for treating edentulous and partially edentulous patients.
Biofunctional prosthetic System Steps Involved In The Bps Denture Fabrication
- Anatomic impression
- Provisional jaw relation (recording vertical jaw relation and tentative centric relation using centric trays)
- Facebow transfer with centric trays in position
- Articulation
- Functional impression
- Determining definite jaw relation
- Definite face bow transfer
- Selection and arrangement of teeth
- Try-in
- Denture insertion.
Biofunctional prosthetic system Anatomic Impression
Biofunctional prosthetic system Materials Used: Impression trays Accu- trays ( 5 differently sized maxillary and mandibular trays).
Impression material System 1 Accu-gel material is available as syringe gel and tray gel to be mixed with water.
Biofunctional prosthetic system Procedure
- Appropriate size tray is selected for maxilla and mandible based on ridge size and shape
- Accu-gel tray material is mixed and loaded on the tray
- Accu- gel syringe material is mixed, loaded in a syringe, and dispensed in the patient’s mouth
- Tray material is inserted over the syringe material
- Accu- dent cast with markings of anatomic landmarks is prepared from the impression for the fabrication of a special tray and occlusal rim.
Biofunctional prosthetic system Provisional Jaw Relation: Materials Used
- Centric tray
- Accu gel tray material
Biofunctional prosthetic system Procedure For Jaw Relation
- The centric tray helps to determine the occlusal position, and centric relation and also helps in mounting the models in the proper relation
- Vertical dimension is measured at rest
- Load the centric tray with Accu-gel and ask the patient to close the mouth until desired VD is obtained.
- A face bow transfer is done with the centric tray in position
- The cast is seated in the impression on the centric tray and it is mounted.
Biofunctional prosthetic system Definitive Jaw relation and functional Impression
- A serrated light cure resin rim is placed on a maxillary custom tray and a normal wax rim is on the mandibular custom tray
- Correct vertical dimension is obtained by adjusting the lower wax rim
- Border molding is done with this tray and a maxillary and mandibular functional impression is made
- For centric relation, gothic arch tracing is done.
- For this, a Gnathometer M (metal trays) is attached to the occlusal surface of the rims with a white spacer in between to maintain the vertical dimension
- After recording the functional impression, the white spacer is removed and intraoral needle point tracing is done
- Interocclusal centric and protrusive bite registration is done for programming the articulator
- The entire assembly is transferred to the Stratos articulator after making the master cast
- Articulation and model orientation is done according to average values with the help of a ‘horizontal guide’ based on the Bonwill triangle of the articulator.
Biofunctional prosthetic system Teeth Selection And Arrangement
Teeth selection and arrangement are done based on anatomical landmarks like:
- Mid-palatine raphe
- Incisive papilla
- First large pair of rugae
- Maxillary tuberosity
- Ridgeline in the posterior region of the mandible
- The retromolar pad
- Teeth arrangement is also based on standard parameters like the Curve of Spee and the Curve of Wilson. Arrangement of teeth is done using the special teeth set for BPS dentures with the help of a setting-up template that follows these landmarks.
Biofunctional prosthetic system Denture Processing
Done using injection molding technique.
Biofunctional prosthetic system Advantages Of Bps Dentures
- Improved stability and retention
- Posterior teeth will be correctly positioned allowing sufficient tongue space
- Reduced food trapping adjacent to the molar teeth
- Good esthetics.
Leave a Reply