Luxation Injuries Treatment Notes
Luxation Injuries
Luxation injuries cause trauma to supporting structures of teeth ranging from minor crushing of periodontal ligament and neurovascular supply of pulp to total displacement of teeth. These are caused by sudden impacts such as a blow, fall, or striking a hard object.
Table of Contents
Incidence
Luxation injuries account for 30–40% of all dental injuries.
Types of luxation injuries:
- Concussion
- Subluxation
- Lateral luxation
- Extrusive luxation
- Intrusive luxation
Read And Learn More: Endodontics Notes
Luxation Injuries Concussion
In concussion
- The tooth is not displaced
- Mobility is not present
- The tooth is tender to percussion because of edema and hemorrhage in the periodontal ligament
- The pulp may respond normally to testing.
Subluxation
In subluxation
- Teeth are sensitive to percussion and have some mobility
- Sulcular bleeding is seen showing damage and rupture of the periodontal ligament fiers
- Pulp responds normally to testing
- The tooth is not displaced.
Treatment of Concussion and Subluxation
- Rule out the root fracture by taking radiographs
- Relieve the occlusion by selective grinding of opposing teeth
- Immobilize the injured teeth.
- Endodontic therapy should not be carried out at the first visit because both negative testing results and crown discoloration can be reversible Follow-up is done at 3 weeks, 3, 6, and 12 months Prognosis there is only a minimal risk of pulp necrosis, and root resorption
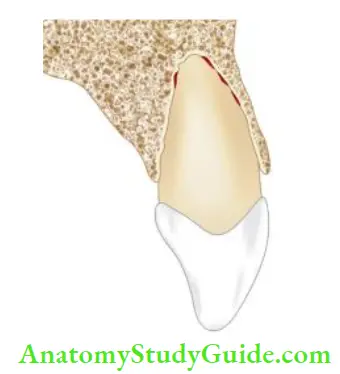
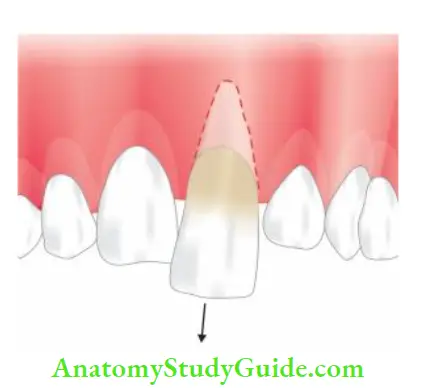
Lateral Luxation
In lateral luxation:
- Trauma displaces the tooth lingually, buccally, mesially, or distally, in other words out of its normal position away from its long axis
- Sulcular bleeding is present indicating rupture of the periodontal ligament (PDL) fiers
- The tooth is sensitive to percussion
- Clinically, the crown of the laterally luxated tooth is usually displaced horizontally with the tooth locked firmly in the new position. Here percussion may elicit a metallic tone indicating that the root has been forced into the alveolar bone.
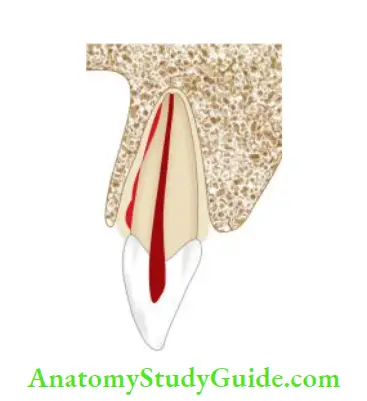
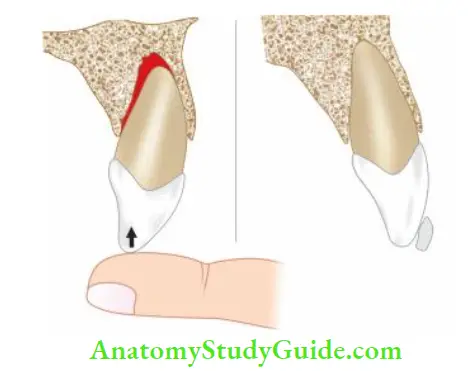
Extrusive Luxation
In extrusive luxation:
- The tooth is displaced from the socket along its long axis
- The tooth is very mobile
- The radiograph shows the displacement of the tooth.
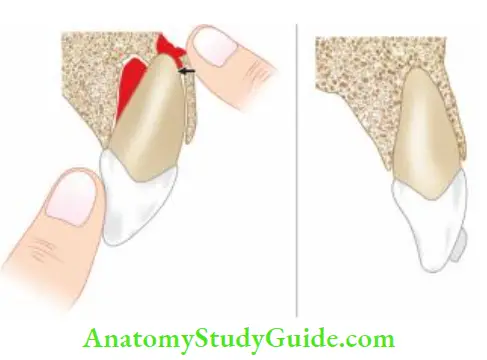
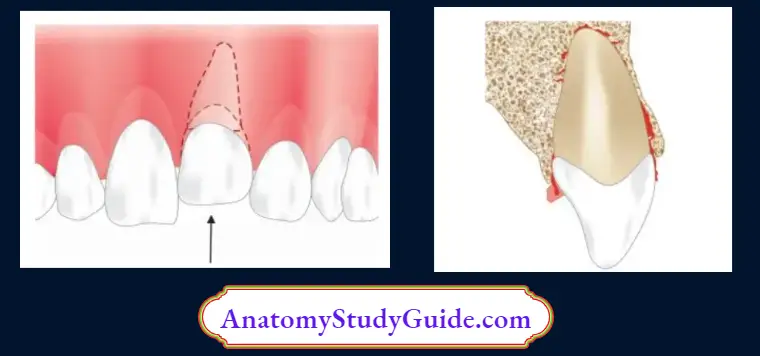
Treatment of Lateral and Extrusive Luxation
Treatments of these injuries consist of atraumatic repositioning and fixation of teeth which prevents excessive movement during healing.
- Repositioning of laterally luxated teeth requires minimal force for positioning. Before repositioning laterally luxated teeth, anesthesia should be administrated. A tooth must be dislodged from the labial cortical plate by moving it coronally and then apically. This tooth is first moved coronally out of the buccal plate of the bone and then fitted into its original position.
- For repositioning of the extruded tooth, a slow and steady pressure is required to displace the coagulum formed between the root apex and flor of the socket. After, this tooth is immobilized, stabilized, and splinted for approximately 2 weeks. Local anesthesia is not needed while doing this.
- Follow-up: Splint is removed 2 weeks after extrusion. If a tooth has become nonvital, inflammatory root resorption can occur, requiring immediate endodontic therapy. Pulp testing should be performed on regular intervals.
Prognosis
It depends on the stage of root development at the time of injury. Commonly seen sequelae of luxation injuries are pulp necrosis, root canal obliteration, and root resorption.
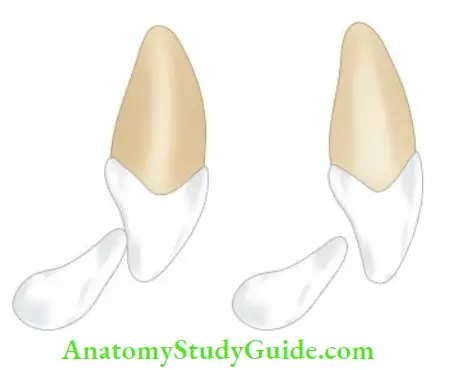
Intrusive Luxation
In intrusive luxation:
- The tooth is forced into its socket in an apical direction
- It is the most damaging injury to a tooth. In other words, it results in maximum damage to the pulp and the supporting structures
- When examined clinically, the tooth is in infra occlusion
- The tooth presents with clinical presentation of ankylosis because of being fit in the socket
- On percussion metallic sound is heard
- In mixed dentition, diagnosis is more difficult as intrusion can mimic a tooth undergoing eruption
- Radiographic evaluation is needed to know the position of the tooth
Intrusive Luxation Treatment
Healing following the intrusive luxation is complicated because intensive injury to the PDL can lead to replacement resorption and further dentoalveolar ankylosis.
Pulp is also affected by this type of injury. So the main objective of treatment is to reduce the extent of these complications. Treatment mainly depends upon the stage of root development.
In immature teeth, spontaneous re-eruption is usually seen. If re-eruption stops before normal occlusion is attained, orthodontic movement is initiated before the tooth gets ankylosed.
If a tooth is severely intruded, surgical access is made to the tooth to attach orthodontic appliances and extrude the tooth. A tooth can also be repositioned by loosening the tooth surgically and aligning it with the adjacent teeth.

Intrusive Luxation Follow-up:
Regular clinical and radiographic evaluation is needed in this case because of the frequent occurrence of pulpal and periodontal healing complications.
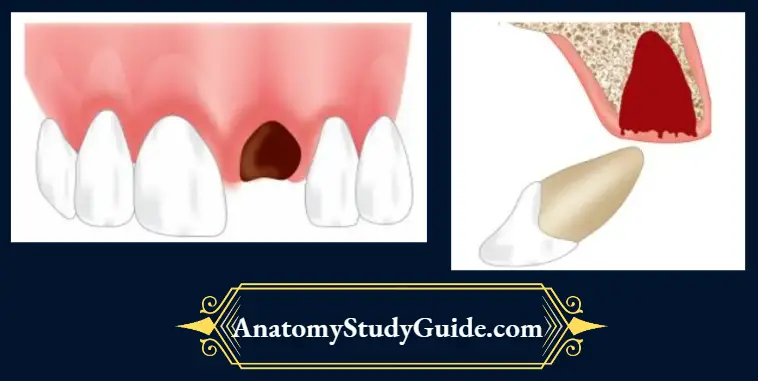
Avulsion/Exarticulation/Total Luxation
It is defined as complete and total displacement of the tooth out of the socket. A common cause is a directed force sufficient to overcome the bond between the affected tooth and the periodontal ligament within the alveolar socket
Incidence
- It usually occurs in the age group of 7–10 years
- 1–16% of all traumatic injuries occurring to permanent dentition
- Sports, fall from height and automobile accidents are the most frequent causes
Biologic Consequences of Avulsion Injury to Teeth
The following are the predominant consequences of avulsion injury to teeth:
- Pulpal necrosis: It occurs due to disruption of blood supply to the tooth. Pulp testing and frequent monitoring of pulp vitality should be done at regular intervals
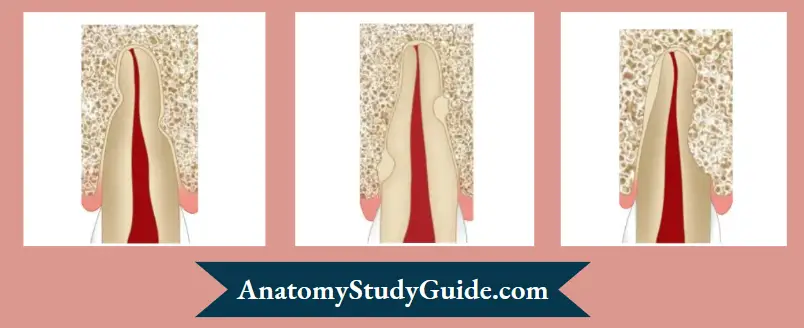
- Surface resorption: In this, small superficial resorption cavities occur within the cementum and the outer dentin. It is the repair process of physical damage to calcified tissue by the recruitment of cells following the removal of damaged tissues by macrophages
- Inflammatory resorption: It occurs as a result of necrotic pulp becoming infected in the presence of severely damaged cementum. This infected pulp allows bacterial toxins to migrate out through the dentinal tubules into the periodontal ligament causing resorption of both root and adjacent bone
- Replacement resorption: It occurs when there is extensive damage to the periodontal ligament and cementum. Healing occurs from the alveolar side creating a union between tooth and bone. It is the incorporation of the root into the normal remodeling process of the alveolus with gradual replacement by bone. As a result, the root is ultimately replaced by bone.
- Radiographically, there is the absence of lamina dura and the root assumes a moth-eaten appearance as dentin is replaced by bone. Clinically the tooth will not show any sign of mobility and on percussion, a metallic sound is heard. Replacement resorption in younger patients may interfere with the growth and development of the alveolar process which subsequently results in infra occlusion of that tooth
The prognosis of treatment depends on
- Extra-alveolar time
- Preservation of root structure
- Storage media
Management of Avulsed Tooth
The main aim of reimplantation is to preserve a maximum number of periodontal ligament cells which have the capability to regenerate and repair the injured root surface. Periodontal ligament cells should be prevented from drying since drying can result in the loss of their normal
physiology and morphology.
If it is not possible to maintain the viable cells of PDL, the aim of the treatment should be directed to slow down the resorption process. The lesser is the time lapse between avulsion and replantation, the better is the prognosis.
If it is not possible to reimplant the tooth immediately, it should be placed in an adequate storage media.
Ideal storage media should
- Be capable of preserving the vitality of periodontal ligament cells
- Be nontoxic
- Have osmolality of 290–330 mOsm/L
- Have a pH of 6.7–7.8
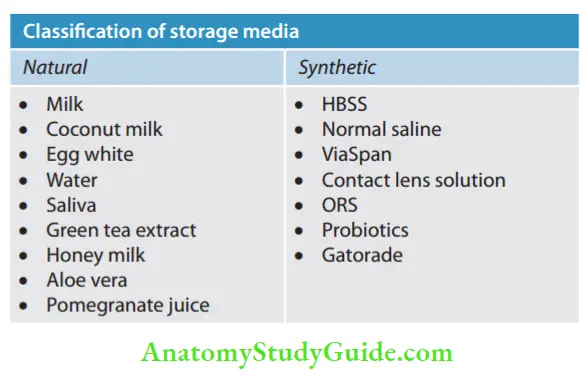
- Milk: It has been shown to maintain the vitality of periodontal ligament cells for 3–4 hours. It is relatively bacteria-free with pH and osmolality compatible with vital cells.
- Coconut water: The electrolyte composition of coconut water is similar to intracellular fluid. It consists of vitamins, minerals, amino acids, and antioxidants. It preserves vitality for up to 8 hours. It has advantage of easy availability, economical and sterile nature.
- Egg white: It consists of proteins, minerals, and ovalbumin. Its advantage is being free from contamination and can store the tooth up to 8 hours.
- Water: This is the least desirable transport medium because it results in hypotonic rapid cell lysis.
- Saliva: It has the advantage that it is a biological fluid. The tooth is kept in a buccal vestibule or in a container with saliva. It provides 2 hours of storage time for an avulsed tooth. However, it is not ideal because of incompatible osmolality, pH, and the presence of bacteria.
- Green tea extract: It is antioxidant and anti-inflammatory which provides storage for up to 24 hours.
- Honey milk: It consists of essential amino acids, vitamins, and minerals. It can preserve cells for up to 8 hours. It maintains the vitality of cells and is bacteriostatic in nature.
- Aloe vera: It consists of vitamins, enzymes, minerals, and amino acids. It increases fibroblasts which increases collagen proliferation. A tooth can be stored for up to 2 h.
- Pomegranate juice: It consists of polyphenolic flavonoids and ellagic acids which have antioxidant properties and promote healing. It can store the tooth from 6–24 h.
- Hank’s balanced solution (Save-A-Tooth): HBSS is biocompatible to periodontal ligament cells and can keep them viable for up to 72 h because of its ideal pH and osmolality. It contains sodium chloride, potassium chloride, glucose, calcium chloride, magnesium chloride, sodium bicarbonate, and sodium phosphate.
- Saline: It is isotonic and sterile and thus can be used as a tooth carrier solution. It provides storage up to 30 min.
- ViaSpan: It has a pH of 7.4 and an osmolarity of 320 Osm/L. These properties are advantageous for cell growth. It can preserve the viability of fibroblasts for 24 h.
- Probiotics: It contains the microorganism Lactobacillus Reuter. It provides viability of periodontal ligament cells similar to HBSS.
- Order of efficacy of different storage media:
- ViaSpan=HBSS>Coconut water>Milk>green tea>egg white
Management Options for an Avulsed Tooth
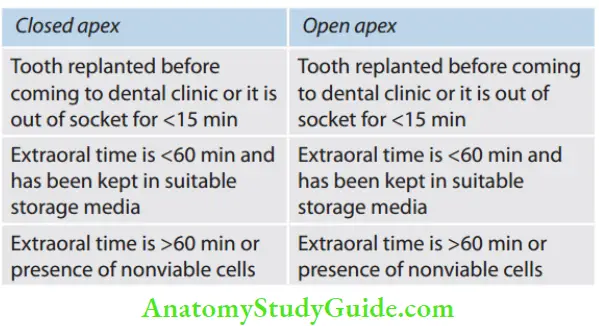
Tooth replanted before coming to a dental clinic or it is out of the socket for <15 min
Closed apex
- Hold the tooth by the crown
- Tell the patient to rinse their mouth with water, saline, or chlorhexidine
- Reimplant the tooth gently with firm finger pressure. Ask the patient to bite firmly on the gauze piece to help stabilize the tooth. If possible, splint the tooth with adjacent teeth using wire for 7–10 days, arch bars, or a temporary periodontal pack
- Put the patient on a soft diet and instruct to do chlorhexidine mouth rinses twice a day for 1–2 weeks
- Prescribe systemic antibiotics preferably tetracycline and plan the next dental appointment. In patients <12 years of age, the preferred antibiotic is phenoxymethyl penicillin. RCT is started after 1 week. Place calcium hydroxide medicament for 1 month followed by obturation of the tooth. Remove the splint and take radiographs after 1, 3, 6, and 12 months for follow-up.
A tooth with open apex
- The goal of the replanting immature tooth is to allow revascularization of the pulp, if it does not occur, RCT is indicated
- Clean the root surface with saline
- Examine the alveolar socket after cleaning it with saline
- Cover the root surface with minocycline hydrochloride microspheres before reimplantation to kill the bacteria which could enter the immature apex and form an abscess
- Reimplant the tooth gently with firm finger pressure. Ask the patient to bite firmly on the gauze piece to stabilize the tooth
- After evaluating the occlusion, give flexible splint for not >7–10 days
- RCT should be avoided unless there is clinical or radiographic evidence of pulp necrosis
- Take radiographs after 1, 3, 6, and 12 months for follow-up
Extraoral time is <60 min and has been kept in suitable storage media
A tooth with closed apex
- Clean the root surface with saline
- Do not touch a viable root with hands, forceps, gauze, or anything, or try to scrub or clean it to avoid injury to the periodontal ligament which makes it difficult to revascularize the reimplanted tooth
- Examine the alveolar socket after cleaning it with saline. Do not overlook fracture of the tooth and alveolar ridge
- Reimplant the tooth gently with firm finger pressure. Ask the patient to bite firmly on the gauze piece to stabilize the tooth
- After evaluating the occlusion, give a flexible splint for not >7–10 days
- RCT is started after 1 week. Place calcium hydroxide medicament for 1 month followed by obturation of the tooth. Remove the splint and take radiographs after 1, 3, 6, and 12 months for follow-up
A tooth with open apex
- The goal of the replanting immature tooth is to allow revascularization of the pulp, if it does not occur, RCT is indicated
- Clean the root surface with saline
- Examine the alveolar socket after cleaning it with saline
- Cover the root surface with minocycline hydrochloride microspheres before reimplantation to increase the chances of revascularization of the pulp. Soaking the tooth in 2% sodium fluoride for 20 min slows down the process of replacement resorption
- Reimplant the tooth gently with firm finger pressure. Ask the patient to bite firmly on gauze piece to stabilize the tooth
- After evaluating the occlusion, give flexible splint for not >7–10 days
- RCT should be avoided unless there is clinical or radiographic evidence of pulp necrosis
- Take radiographs after 1, 3, 6, and 12 months for follow-up

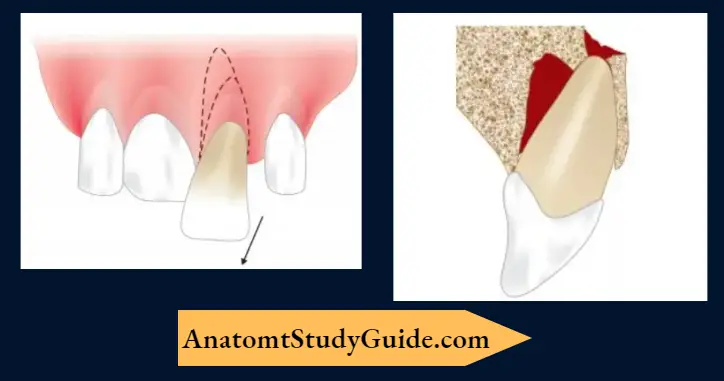
- (A) Photograph showing avulsed central incisor;
- (B) Tooth repositioned and splinting done;
- (C) Radiograph showing positioning and stabilization of teeth.
Extraoral time is >60 min or the presence of nonviable cells. A tooth with a closed apex:
- If the tooth was out over 2 h, the periodontal ligament becomes dead and should be removed along with the pulp. The goal of delayed replantation is to promote alveolar bone growth to encapsulate the tooth
- Local anesthesia will probably be needed before reimplanting as above
- The tooth should be soaked for 20 min in 2.4% stannous fluoride, or sodium hypochlorite for 5 min to remove all remaining dead periodontal ligament cells that may initiate the resorption process on replantation
- Endodontic treatment is done either before replantation or 7–10 days after replantation
- Replant the tooth gently with firm finger pressure. Ask the patient to bite down firmly on a piece of gauze to help stabilize the tooth
- Verify the position of the replanted tooth on the radiograph
- Stabilize it for 4 weeks
- Administer systemic antibiotics
After completion of endodontic treatment, take follow-up radiographs after 1, 3, 6, 9, and 12 months.
A tooth with open apex:
- The periodontal ligament is dead and is not expected to heal. The goal of delayed replantation is to preserve the alveolar ridge contour
- The tooth should be soaked for 20 min in 2.4% stannous fluoride and 5 min in doxycycline to slow down the replacement resorption of the tooth
- RCT can be started prior to or after replantation
- Replant the tooth gently with firm finger pressure. Ask the patient to bite down firmly on a piece of gauze to help stabilize the tooth
- Verify the position of the replanted tooth on the radiograph
- Stabilize it for 4 weeks
- Administer systemic antibiotics
- After completion of endodontic treatment, take follow-up radiographs after 1, 3, 6, 9, and 12 months
- Replanted primary tooth heals by ankylosis which can cause
- Cosmetic deformity because an ankylosed tooth will not grow at the same rate as the rest of the dentofacial complex
- Interference with the eruption of permanent tooth
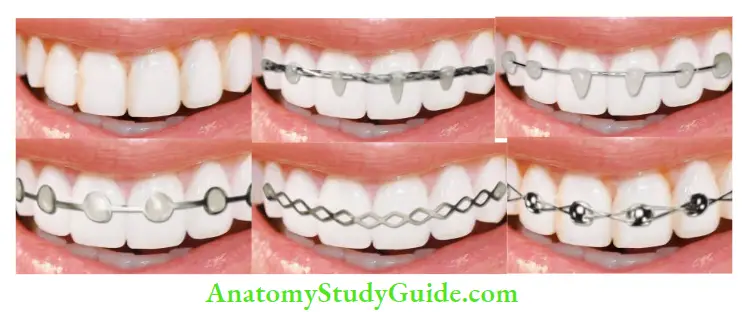
Types of Splints
Composite Splint
It is a rigid splint, here composite is applied to the surfaces
of teeth. Composite resin is applied on the labial or interproximal surfaces of the teeth for splinting mobile teeth to the adjacent teeth.
Composite and Wire Splint
It is the most commonly used flexible splint. Here, the wire having a diameter of 0.3–0.4 mm is used with composite resin.
Orthodontic Wire and Bracket Splint
This splint uses orthodontic brackets bonded to the teeth and connected with a light 0.014 NiTi flexible wire. It can be irritating to the lips when compared to composite and wire splints and titanium trauma splints; this can be solved by applying wax.
Fiber Splint
It uses a polyethylene fier mesh and is attached with an unfiled resin and/or with composite resin. Commercially available materials are Fiber-Splint, Ribbond, or EverStick.
Titanium Trauma Splints
The titanium trauma splint is a flexible splint made of titanium approximately 0.2 mm thick and 2.8 mm wide. It has a rhomboid mesh structure which is fixed to the flowable composite resin.
Arch Bar Splint
Here a metal bar is bent into the shape of the arch and fied with ligature wires. It is a rigid splint and may cause gingival irritation.
Wire Ligature Splint
It is a rigid splint and may impinge on the gingival tissues causing inflmmation.
Flexible Splint
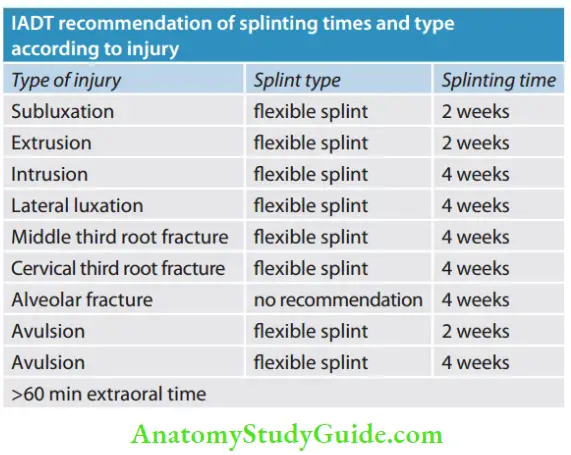
Composite and wire splints, orthodontic wire and bracket splints, and titanium trauma splints are types of flexible splints. These allow physiologic movement to the tooth during the healing phase reducing the chances of ankylosis. The IADT guidelines recommend a flexible splint for all injury classifications except for alveolar fracture where no recommendation is given.
Contraindications of Replantation:
- Compromised medical status of the patient
- Extensive damage to supporting tissues of the tooth
- Child’s stage of dental development in which there are chances of ankylosis are more
- Legal consequences:
- Delaying reimplantation
- Improper handling and transportation of the tooth
- Reimplanting a primary tooth
- Not providing the tetanus prophylaxis
- Incomplete examination of the surrounding traumatized tissue for tooth fragments
- Failure to warn patients that any trauma to teeth may disrupt the neurovascular supply and lead to long-term pulp necrosis or root resorption.
Leave a Reply