Male External Genital Organs
Question 1. What are male External Genital Organs?
Answer:
Anatomically, the male external genital organs include the penis, urethra, and scrotum. However clinically it also includes spermatic cords, testes, and epididymis.
Question 2. Describe the Penis in brief under the following headings:
- Penis Definition:
- Penis Parts
- Penis Structure of body
- Penis Arterial supply
- Penis Venous drainage
- Penis Lymphatic drainage
- Penis Innervation
- Penis Mechanism of erection and
- Penis Applied anatomy.
Answer:
1. Penis Definition:
Penis is a male organ of copulation and deposits semen into the vagina. The urethra within it provides a common passage to both urine and semen. Parts
Read And Learn More: Anatomy Question And Answers
2. Penis consists of two parts:
- Root, an attached portion.
- Body, a free pendulous portion.
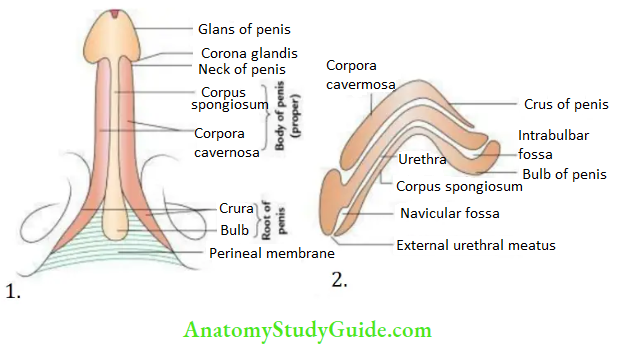
3. Penis Structure of Body:
- The root consists of two crura and a bulb. The crura are attached to the ischiopubic mnrami and covered by ischiocavernosus muscles.
- The bulb of the penis is attached to the inferior aspect of the perineal membrane and covered by the bulbospongiosus muscle.
- The body is a free pendulous part with an enlarged conical free end, the glans of the penis.
The body consists of three elongated masses of erectile tissue:
Two corpora cavernosa were placed dorsally one on either side and one corpus spongiosum was placed ventrally in the midline. The corpora cavernosa are surrounded by a common fibrous sheath called tunica albuginea while corpus spongiosum is surrounded separately by a thin layer of tunica albuginea.
Coverings:
From superficial to deep penis is covered by skin, superficial fascia, and deep fascia (Buck’s fascia). The skin of the penis is thin, dark, and hairless. At the neck of the penis, it is folded on itself to form the prepuce or foreskin, which covers the glans penis to a variable extent.
Question 3. Define prepuce. Describe briefly phimosis, paraphimosis, and circumcision.
Answer:
The prepuce is a fold of skin that covers the glans penis. Normally it can be retracted back to expose the glans of the penis.
- Phimosis: It is a condition in which the foreskin (prepuce) is too tight to be pulled back to reveal glans, i.e. narrowing of the distal end of the prepuce.
- Paraphimosis: In this condition, the retracted foreskin can not be returned back to its normal position. It gets stuck on the glans posteriorly.
- Circumcision: It is the removal of the foreskin of the penis.
4. Penis Arterial supply:
The penis has a rich blood supply through four pairs of arteries:
- Deep arteries of the penis
- Dorsal arteries of the penis
- Arteries of bulb
- Superficial arteries from superficial pudendal arteries
5. Penis Venous drainage:
By two veins: Superficial and deep dorsal veins of the penis.
6. Penis Lymphatic drainage:
Lymph from the glans penis is drained into deep inguinal lymph nodes particularly in the lymph node of Cloquet, while lymph from the rest of the penis, skin, and prepuce is drained into the medial group of superficial inguinal lymph nodes.
7. Innervation:
- Sensory innervation, by the dorsal nerve of the penis and ilioinguinal nerve.
- Motor (somatic) innervation, by the perineal branch of the pudendal nerve.
- Automatic innervation, by inferior hypogastric plexus via prostatic plexus. The parasympathetic fibers (S2, S3, and S4) are vasoconstrictors, while sympathetic fibers are vasodilators.
8. Penis Mechanism of erection:
- Following parasympathetic stimulation, the cavernous spaces of the penis get filled and dilated with blood from the helicine arteries.
- This leads to compression of veins egressing from corpora cavernosa, impeding the return of venous blood. Consequently, the corpora cavernosa and corpus spongiosum become engorged with blood causing the penis to become long, hard, and warm – the erection of penis. Which is essential for copulation.
9. Penis Applied anatomy:
- Impotence: Loss of erection of the penis.
- Priapism: Persistent erection of the penis.
- Peyronie’s disease/chordee: Bending of the penis during erection. It occurs due to the formation of localized fibrous plaque in corpora cavernosa. It is often associated with hypospadias.
- Phimosis.
- Paraphimosis.
- Circumcision
Question 4. What is a scrotum? Enumerate the layers of the scrotal wall.
Answer:
Scrotum Anatomy
Scrotum is a large pendulous fibromuscular cutaneous bag lying below the pubic symphysis and posteroinferior to the penis.
Scrotum Contents:
- Testes
- Epididymis
- Spermatic cords (lower part)
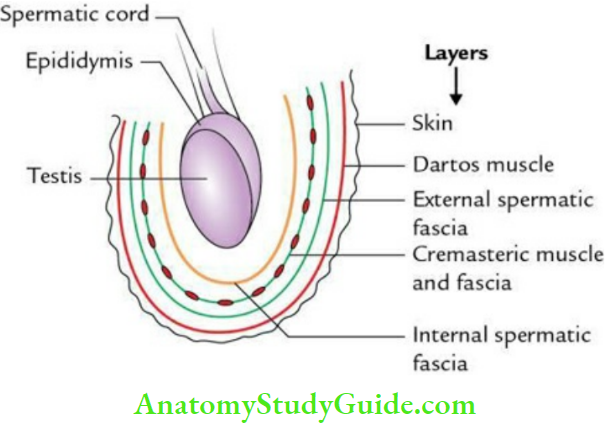
Scrotum Layers:
From without inward, these are
- Skin, which is thin and rugose
- Superficial fascia containing dartos muscle (smooth muscle)
- External spermatic fascia derived from the external oblique
- Cremasteric fascia and muscle derived from the internal oblique
- Internal spermatic fascia derived from fascia transversalis
Note: All the layers of the anterior abdominal wall continue in the scrotal wall except the transversus abdominis muscle, which does not continue into the scrotal wall.
Scrotum Anatomy
Scrotum Nerve supply
- Anterior 1/3rd of scrotum by L1 spinal segment through:
- Ilioinguinal nerve
- Genital branch of genitofemoral nerve
- Posterior 2/3rd of the scrotum by S3 spinal segment through:
- Posterior scrotal nerve, a branch of the pudendal nerve
- Perineal branch of the posterior cutaneous nerve of the thigh
Question 5. Write a short note on the pampiniform plexus of the testis and discuss its applied anatomy.
Answer:
Pampiniform plexus:
The pampiniform plexus is a plexus of veins emerging from the testis. This plexus is arranged into two groups: the anterior group around the testicular artery and the posterior group around the vas deferens.
The fate of pampiniform plexus:
- At the superficial inguinal ring, it condenses to form 4 veins which join at the deep inguinal ring to form 2 veins.
- Beyond the deep inguinal ring, these 2 veins unite to form a single testicular vein, which drains into the inferior vena cava on the right side and the left renal vein on the left side.
Pampiniform plexus Applied anatomy:
Varicocele:
It is a clinical condition in which veins of the pampiniform plexus become dilated, tortuous, and elongated. It mostly occurs on the left side because
- The left testicular vein drains at a right angle in the left renal vein; hence, venous pressure is high in the left testicular vein,
- The left testicular vein is compressed by a loaded constipated sigmoid colon, and
- Blockage of the left renal vein due to invasion by a malignant tumor growing in the left kidney.
- The last two factors impede the return of venous blood by the left testicular vein.
Clinically, varicocele presents:
- Vague, dragging sensations and aching pain in the scrotum
- On palpation, the veins of the pampiniform plexus feel like a ‘bag of worms.
Scrotum Anatomy
Question 6. Describe the Testis under the following headings:
Answer:
- Testis Introduction
- Testis External features
- Testis Coverings
- Testis Structure
- Testis Arterial supply
- Testis Venous drainage
- Testis Nerve supply
- Testis Lymphatic drainage and
- Testis Applied anatomy.
Answer:
1. Testis Introduction:
- The testis is an internal male reproductive organ present in the scrotum one on either side of the median plane.
- It is suspended in the scrotum by the spermatic cord.
- It lies obliquely in the scrotum (tilted forward and laterally) as a result, its lower pole is directed backward and medially.
- The left testis lies at a lower level than the right testis because the left testis migrates early and has a longer spermatic cord.
2. Testis External features:
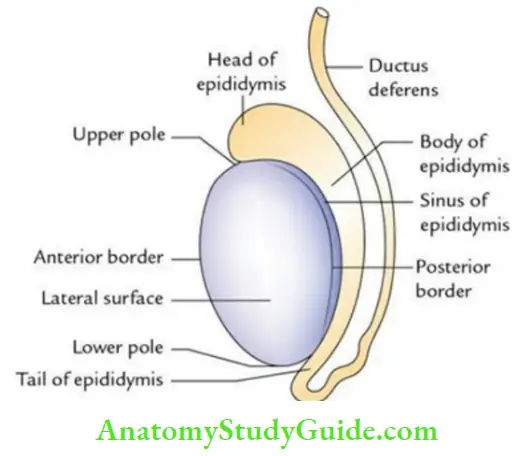
- Shape: Ellipsoid.
- Dimension: Length 5 cm; breadth 2.5 cm; anteroposterior dimension 3 cm.
- Weight: 10–15 gm.
- 2 Poles: Upper and lower.
- 2 Borders: Anterior and posterior.
- 2 Surfaces: Medial and lateral.
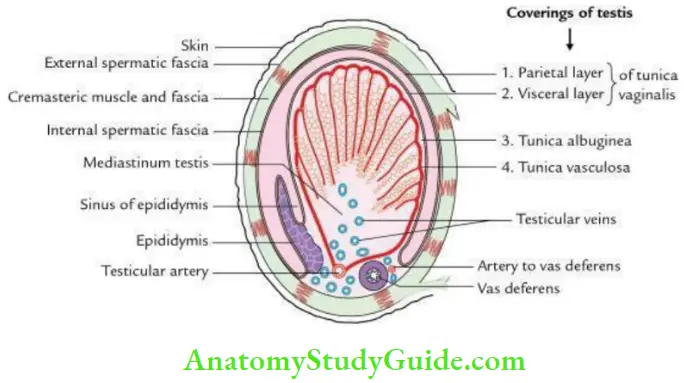
3. Testis Coverings:
- The testis is covered by 3 coats. From superficial to deep, these are:
- Tunical vaginalis, a serous coat consisting of visceral and parietal layers
- Tunica albuginea, a white dense fibrous coat
- Tunica vasculosa, a vascular coat.
- The surface of the testis is covered by the visceral layer of tunica vaginalis (closed peritoneal sac) except where the testis attaches to the epididymis.
- A slit-like recess of tunica vaginalis between the body of the epididymis and the posterolateral surface of the testis is called the sinus of the epididymis.
4. Testis Structure:
Testis Macroscopic structure:
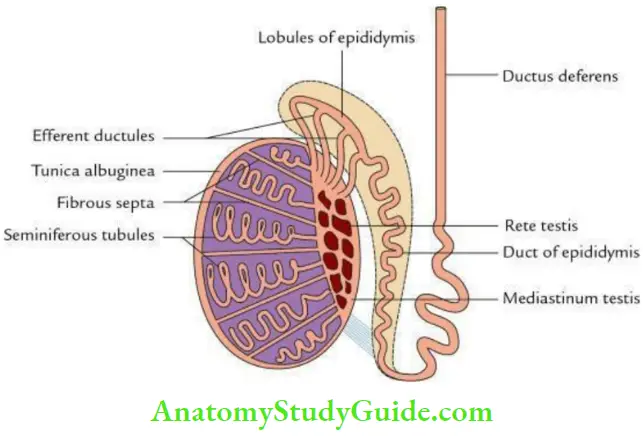
A section through the testis presents the following macroscopic features:
- White dense fibrous coat (tunica albuginea) covers the testis all around, which is thickened posteriorly to form mediastinum testis.
- Fibrous septa extending from mediastinum testis to tunica albuginea divide the testis into 200 to 300 lobules. Each lobe contains 2–3 coiled seminiferous tubules.
- Seminiferous tubules open into the network of channels (rete testis) within mediastinum testis by 20 to 30 straight tubules formed by the anastomoses of seminiferous tubules.
- Efferent ductules connect the rete testis to the upper end of the epididymis.
Microscopic/histological structure:
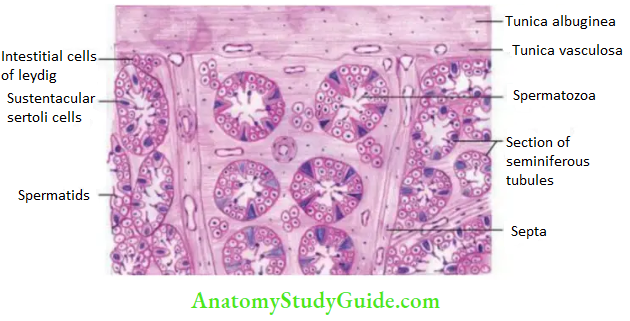
The histological section of the testis presents the following features :
- Coiled seminiferous tubules sectioned in various planes.
- Columns of four to eight layers of spermatogenic cells lie between the basement membrane and the lumen of the tubule.
- Presence of Leydig cells between the seminiferous tubules.
- Presence of spermatozoa in the lumen of the tubule.
- Presence of Sertoli/supporting cells between the cells of the spermatogenic lineage.
Note:
Testis Function
Spermatogenic cells are arranged in columns between Sertoli cells and from superficial to deep these are:
- Spermatogonium: lies near the basement membrane. They have clear cytoplasm, and their nuclei show a chromatin network.
- Primary spermatocyte: Lies next to spermatogonium. They are large cells with spherical nuclei.
- Secondary spermatocyte: Situated next to primary spermatocyte. They are small, and their nuclei show mitotic divisions.
- Spermatid: Located near the lumen. They are small and have rounded nuclei.
- Spermatozoa: Small cells with tail present in the lumen.
- Sertoli cells: Large elongated pyramidal cells, wedged between the columns of spermatogenic cells.
- Leydig cells: Lie in interstitial spaces between tubules either in single or in clumps.
5. Testis Function – Testis Arterial supply:
Testicular artery (main artery of testis):
It arises from the abdominal aorta at the level of L2 vertebra. At the posterior border of the testis, it divides into small and large branches.
- Small branches enter the posterior border.
- Long branches pierce the tunica albuginea and run on the surface of the testis to ramify and form tunica vasculosa.
Artery to vas deferens, a branch of the inferior vesical artery, also sometimes supplies the testis.
6. Testis Venous drainage:
- By testicular vein into the inferior vena cava on the right side and left renal vein on the left side.
- The testicular vein is formed by the condensation of the pampiniform plexus.
- Initially, they are 4 in number at the superficial inguinal ring and then become 2 at the deep inguinal ring. Later these 2 veins join to form a single testicular vein.
Testis Function Note:
The temperature of blood in the testis is maintained by a counter-current heat exchange mechanism. The temperature difference of blood flowing in the testis is 3° to 4°.
7. Testis Nerve supply:
By sympathetic fibers derived from T10 spinal segment reach the testis through renal and aortic plexuses.
8. Testis Lymphatic drainage:
The lymph from the testis is drained into pre-aortic and para-aortic lymph nodes at the level of L2 vertebra.
9. Testis Applied anatomy:
- Varicocele: It is dilatation and tortuosity of veins of pampiniform plexus
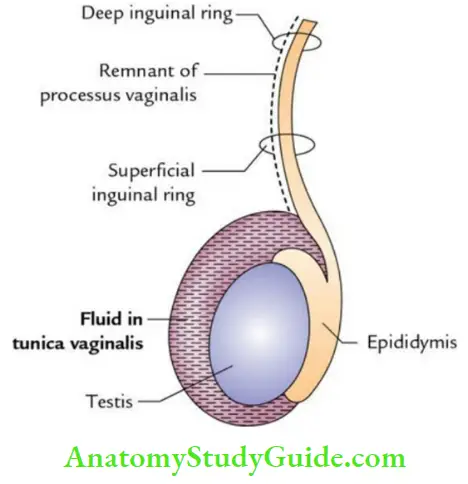
- Hydrocele: It is accumulation of fluid in the tunica vaginalis of testis’
Tumors of the testis:
- The two main varieties of testicular tumors are seminoma (carcinoma of the seminiferous tubules) and teratoma (malignant change in the totipotent cells).
- The cancer cells from the testis spread upward via the lymph vessels to the lumbar (pre- and para-aortic) lymph nodes at the level of L1/L2 vertebra and produce secondary tumors in the abdomen.
Torsion of the testis:
- It is a clinical condition in which rotation of the scrotum occurs around the spermatic cord within the scrotum.
- It commonly affects active young people and children and is accompanied by severe pain.
Question 7. Describe the development of Testis. Write a note on its descent and associated congenital anomalies.
Answer:
Development of the Testis:
The testis develops retroperitoneally on the posterior abdominal wall from a mesodermal genital ridge just medial to the developing kidney the mesonephros at the level of T10 to T12 segments.
The details are as follows:
Testis Indifferent stage:
- It begins in the 4th week of intrauterine life.
- The genital ridge is oval in shape and covered by coelomic epithelium.
- It differentiates into outer part called the cortex and an inner part called the medulla.
- The surface epithelial cells proliferate to form finger-like cords, which penetrate the mesenchyme of the genital ridge. These cords are called primitive sex cords.
- The primordial germ cells from the wall of the yolk sac (derived from epiblast) migrate and get incorporated in the sex cords.
Testis Definitive stage:
- It begins in the 7th week of intrauterine life.
- The indifferent gonad begins to develop into testis under the influence of the SRY gene of the Y chromosome.
- The primary sex cords increase in length and extend into the medulla. Towards the hilum, these cords break up into tiny cell strands that anastomose with each other. They become canalized and form rete testis.
- The sex cords in cortex become horseshoe-shaped and canalized to form seminiferous tubules.
- The dense fibrous layer (tunica albuginea) develops around the developing testis.
- The rete testis gets connected with the mesonephric tubules and mesonephric duct.
- The mesonephric tubules become efferent ductules, whereas the mesonephric duct gives rise to epididymis, vas deferens, seminal vesicle, and ejaculatory duct.
Note:
Sources of origin of various cell types of testis:
- Primordial germ cells are endodermal in origin and are derived from the wall of the yolk sac (recently, it is thought that they are derived from epiblast).
- Sertoli cells are derived from coelomic epithelium.
- Leydig cells are derived from the mesenchymal cells of the mesonephros.
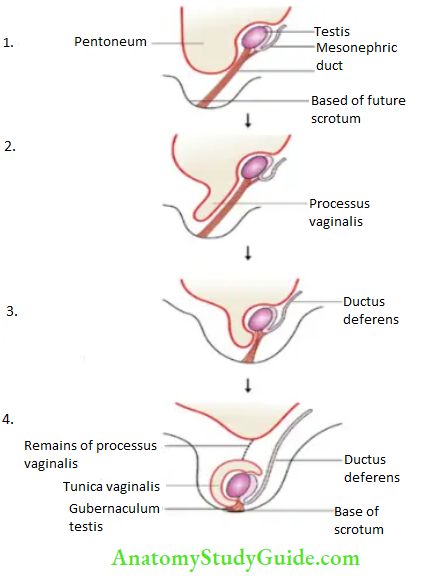
Descent of testis:
The testis begins to descend in the 2nd month of intrauterine life to reach the scrotum.
- Reaches iliac fossa by 3rd month
- Reaches deep inguinal ring by 6th month
- Transverses inguinal canal during 7th month
- Reaches superficial inguinal ring by 8th month
- Reaches in the scrotum (near the bottom) by the 9th month
Factors responsible for the descent of the testis are grouped as:
- Male sex hormones and maternal gonadotrophins (the most important factor)
- Gubernaculum testis and differential growth of body wall
- High intra-abdominal temperature, not suitable for spermatogenesis
- Formation of the inguinal bursa, an outpouching of the various layers of the anterior abdominal wall to form the scrotum
- Formation of process vaginalis, a diverticulum of the peritoneal cavity that guides the descent of the testis
- Squeezing action of inguinal muscles as the testis enters into the inguinal canal
- A specific neurotransmitter called CGRP (calcitonin gene-related peptide) is released by genitofemoral nerve fibers supplying muscular fibers of the gubernaculum
Congenital anomalies of descent:
These anomalies of descent are of two types
- Cryptorchidism (undescended testis) and
- Ectopic testis (abnormally placed testis).
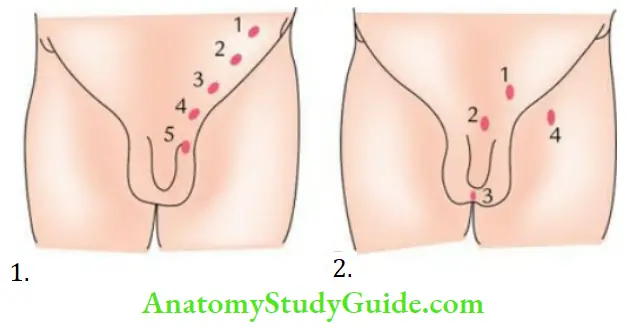
Congenital anomalies Cryptorchidism:
The descent of the testis may be arrested at any point along its normal route of journey.
Depending upon the location, it is classified into the following types:
- Lumbar, if located in the abdomen (1).
- The Iliac fossa is located at the deep inguinal ring (2).
- Inguinal, if located within the inguinal canal (3).
- Pubic, is located at the superficial inguinal ring (4).
- Scrotal, is located high up in the scrotum (5).
Note:
- The complications of cryptorchidism are: improper spermatogenesis and
- Development of malignancy. The unilateral absence of the testis in the scrotum is called monarchism, while the bilateral absence of the testis is called anorchism.
Ectopic testis (maldescent of testis) :
In this condition, the testis successfully descends along its normal path up to the superficial inguinal ring, but thereafter, it deviates from the normal path and reaches at sites other than the scrotum.
The common sites of ectopic testis are:
- In the superficial fascia of the anterior abdominal wall above the superficial inguinal ring (1)
- At the root of the penis/in front of the pubis (2)
- In the perineum (3)
- In the femoral region of the thigh (4)
Question 8.Write a short note on the Epididymis.
Answer:
Epididymis Pain
The epididymis is an elongated comma-shaped structure, which lies on to the superior and posterolateral surface of the testis. It is made up of highly coiled tubes.
Epididymis Parts:
- From above downward, the epididymis is divided into three parts: head, body, and tail.
- The head (the upper expanded part) is connected to the upper pole of testis by efferent ductules and consists of highly coiled efferent ductules.
- The body (middle part) and tail (lower narrow part) are made up of a single highly coiled duct of epididymis, which emerges from the tail as the vas deferens.
Epididymis Functions:
- Reception of spermatozoa from testis
- Storage and maturation of spermatozoa
- Absorption of extra fluid
- Addition of substances to the seminal fluid to nourish the maturating spermatozoa
- Transfer of mature sperms into vas deferens
Epididymis Pain
Epididymis Arterial supply:
By testicular artery.
Question 9.Give the histological features of the epididymis.
Answer:
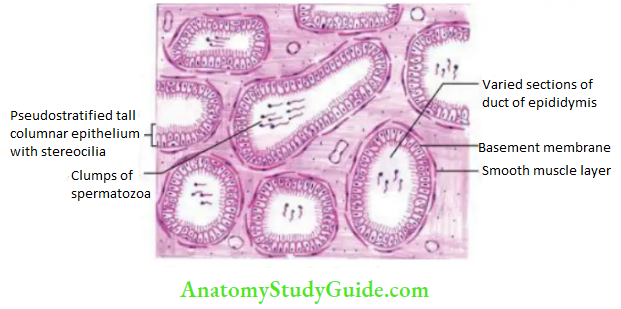
The histological section of epididymis presents the following features:
Epididymis Pain
- A number of tubules of various shapes and sizes.
- Tubules are lined by pseudostratified tall columnar epithelium. The tall columnar cells possess nonmotile stereocilia.
- Presence of bunches of spermatozoa in lumen of tubules.
- Lamina propria is a thin fibrous layer surrounded by a thin muscle layer made up of circularly placed smooth muscle fibers.
Leave a Reply