Meckels Diverticulum With A Band
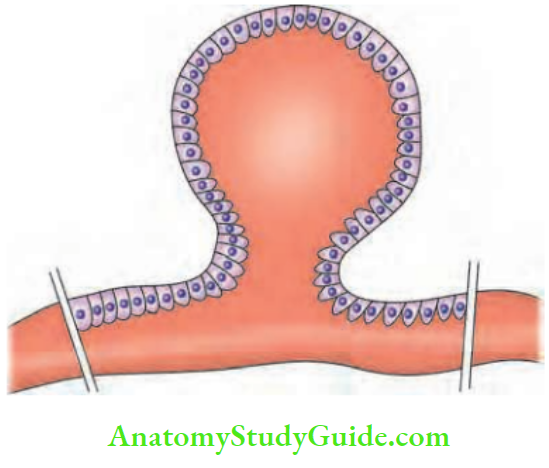
It is a congenital diverticulum which occurs due to persistent intestinal end of vitellointestinal duct. Being congenital, it has all the layers of the bowel. Hence, it is a true diverticulum.
Table of Contents
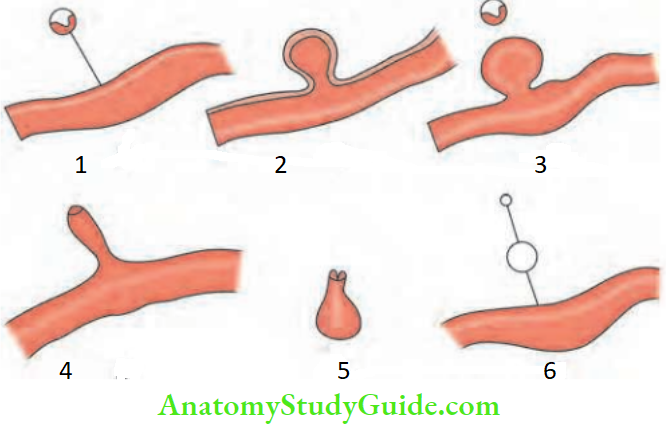
Anomalies of Vitellointestinal Duct:
- Fibrous band: A fibrous band results when entire duct is obliterated and the bowel can twist around the band, resulting in volvulus.
- Persistent intestinal end: Meckel’s diverticulum.
- Meckel’s diverticulum: Meckel’s diverticulum with the band attached to the umbilicus can give rise to intestinal obstruction.
- Umbilical fistula: Umbilical fistula results when the entire duct is patent.
- Even though it is connected to the terminal ileum, the opening is very small. The discharge is rarely faecal. Often, it is the mucus secreted from the lining of the duct (omphaloenteric fistula).
- Umbilical sinus: Umbilical sinus results due to persistent umbilical end discharging mucus. Slowly umbilical adenoma occurs and the epithelial lining of the sinus gets everted.
- Intra-abdominal cyst: Intra-abdominal cyst results when both ends are obliterated. The central portion of the duct persists and secretes mucus. This is very, very rare.
Meckeles Diverticulum With A Band
- It is present in 2% of the cases, 2 inches long, 2 feet away from the ileocaecal region in the antimesenteric border (ileal duplication can occur in the mesenteric border). It is two times more common in females.
- Symptomatic cases are below 2 years of age. In 12% of the patients, heterotopic gastric tissue is found which can produce peptic ulceration. In a few other patients, it can contain pancreatic and colonic tissue. Other anomalies.
Meckel’s1 Diverticulum and Other Associated Anomalies:
- Angiodysplasia of the caecum
- Anorectal atresia, atresia of the oesophagus
Rule Of 2 For Meckel’S Diverticulum:
- Incidence: 2%
- Location: 2 feet proximal to the ileocaecal junction
- Length: 2 inches long
- Ectopic tissue: 2 types—gastric and pancreatic
- Presentation: 2 years or below 2 years is the most common age
- Male: Female ratio—1:2
Meckel’s1 Diverticulum Clinical Presentation
1. Massive bleeding per rectum:
- In the form of melaena, it is not uncommon.
- In many other patients, mild chronic bleeding can result in anaemia. Blood is maroon coloured.
2. Acute Meckel’s diverticulitis:
Factors which precipitate diverticulitis are
- Peptic ulceration due to ectopic gastric mucosa of the diverticulum
- Ingested foreign material, for example, a stalk of vegetable, seeds, fish or chicken bones
- Faecolith (not common in ileum), tumours, worms causing stasis and bacterial infection
- Inflammation and ischaemia caused by torsion due to an associated band is called mesodiverticular band
- Association with acute appendicitis
Meckel’s1 Diverticulum Perforation
- It is impossible to differentiate it from a ruptured appendix. This is treated by laparotomy and resection of the diverticulum along with the adjacent intestine.
- In the majority of appendicular perforations, the local abscess will occur because of retrocaecal position of the appendix (70%). However, perforation of
- Meckel’s diverticulum, even though a rare cause of peritonitis, has a high mortality rate. This is because the infection spreads very fast as the diverticulum is intraperitoneal and contents are faeculent.
- As a cause of intestinal obstruction, when it is associated with a band or due to volvulus. It is the most common presentation in adults
- As a cause of intussusception: Here also, inflamed heterotopic tissue can be found in the diverticulum (2% cases).
- Pain: Pain can occur due to chronic peptic ulceration.
- Neoplasm: Carcinoids and GIST are more common in Meckel’s diverticulum than elsewhere in the small intestine although the presence of Meckel’s diverticulum itself is rare.
Meckel’s Diverticulum and Intestinal Obstruction:
- Intussusception
- Band
- Volvulus due to band
- Internal herniation beneath mesodiverticular band
- Diverticulitis with band
- Littre’s hernia
Meckel’s1 Diverticulum Investigations
- No investigation can prove a diagnosis of Meckel’s diverticulum. Small bowel enema may demonstrate the diverticulum if the opening is wide (fluoroscopy is ideal).
- 99mTc-labelled pertechnetate when given IV, may localise the heterotopic gastric mucosa in the Meckel’s diverticulum, in about 90% of patients.
- This radionuclide is taken up by mucin-secreting cells and parietal cells and it is secreted immediately. Thus, if 99mTc appears in the stomach as well as in another part of bowel, it indicates functioning heterotopic tissue.
- Even when bleeding is at a rate of 0.1 ml/minute, it can detect Meckel’s diverticulum. Hence, it is superior to angiography.
- Very useful in children with bleeding
Meckel’s1 Diverticulum Treatment
- Incidentally found Meckel’s during laparotomy for some other causes can be left alone, provided it has a wide mouth. However, a note of it must be made in the operation register.
- Meckel’s diverticulum with bleeding, band, perforation and narrow mouth is treated by removal of the diverticulum with adjacent intestine because the gastric tissue may often line the intestine also.
Indications for Removal of Incidentally Found Meckel’s Diverticulum:
- Children under 2 years of age
- Meckel’s with a band
- Meckel’s with adhesions
- Meckel’s with a narrow base
- Long Meckel’s diverticulum

Leave a Reply