Acute Inflammation —Factors Determining Variation In Response, Morphologic Patterns, Systemic Effects, Outcome
The acute inflammatory response discussed above is general and is applicable to all types of etiologic agents. However, it is known that there are variations in response based on host and etiologic agent; variations in morphologic patterns based on duration, type of exudates and type of tissue involved; the appearance of systemic effects in some types of acute inflammation but not all; and variable outcome based on certain factors. These aspects are discussed below.
Read And Learn More: General Pathology Notes
Factors Determining Variation In Response:
Although acute inflammation is typically characterised by vascular and cellular events with the transmigration of neutrophilic leucocytes, not all examples of acute inflammation show infiltration by neutrophils.
On the other hand, some chronic inflammatory conditions are characterised by neutrophilic infiltration. For example, typhoid fever is an example of acute inflammatory process but the cellular response in it is lymphocytic; osteomyelitis is an example of chronic inflammation but the cellular response in this condition is mainly neutrophilic admixed with other chronic inflammatory cells.
The variation in inflammatory response depends upon a number of factors and processes. These may pertain to the organisms and the host:
Factors Involving The Organisms:
- Types of injury and infection: For example, skin reacts to herpes simplex infection by the formation of vesicle and to streptococcal infection by the formation of boil; the lung reacts to pneumococci by the occurrence of lobar pneumonia while to tubercle bacilli it reacts by granulomatous inflammation.
- Virulence: Many species and strains of organisms may have varying virulence for example, The three strains of C. diphtheriae (gravis, intermedius and mitis) produce the same diphtherial exotoxin but in different amounts.
- Dose: The concentration of organism in small doses produces usually local lesions while larger dose results in more severe spreading infections.
- Portal of entry: Some organisms are infective only if administered by a particular route for example, Vibrio cholerae is not pathogenic if injected subcutaneously but causes cholera if swallowed.
- Product of organisms: Some organisms produce enzymes that help in the spread of infections for example,Hyaluronidase by Clostridium welchii, streptokinase by streptococci, staphylokinase and coagulase by staphylococci.
Factors Involving The Host:
- Systemic diseases: Certain acquired systemic diseases in the host are associated with impaired inflammatory response for example Diabetes mellitus, chronic renal failure, cirrhosis of the liver, chronic alcoholism, and bone marrow suppression from various causes (drugs, radiation, idiopathic). These conditions render the host more susceptible to infections.
- Immune status of host: Patients who are immunosuppressed from congenital or acquired immunodeficiency have lowered inflammatory response and the spread of infections occurs rapidly for example, In AIDS, congenital immunodeficiency diseases, diabetes mellitus, protein-calorie malnutrition, and starvation.
- Congenital neutrophil defects: Congenital defects in neutrophil structure and functions result in reduced inflammatory response.
- Leukopenia: Patients with low WBC count with neutropenia or agranulocytosis develop spreading infection.
- Site or type of tissue involved: For example, the lung has a loose texture as compared to bone
and, thus, both tissues react differently to acute inflammation. - Local host factors: For instance, ischaemia, the presence of foreign bodies and chemicals causes necrosis and thus causes more harm.
Morphologic Patterns Of Acute Inflammation:
Inflammation of an organ is usually named by adding the suffix -itis to its Latin name for example, Appendicitis, Hepatitis, Cholecystitis, Meningitis etc. All these conditions.
However, a few general morphologic patterns of acute inflammation are described below
1. Classification Of Inflammatory Reaction;
An inflammatory lesion is classified based on duration, type of exudates and anatomic location affected:
- Duration: Inflammation is acute when the onset of inflammatory reaction is early and last short duration, while chronic inflammation appears after delay and is long-lasting. Subacute inflammation lasts for a few weeks.
- Type of exudates: Inflammation is accompanied with the appearance of escaped plasma into tissue spaces or body cavities which determines the morphologic type of inflammation:
- Serous, when the fluid exudate resembles serum or is watery for example, Pleural effusion in tuberculosis, blister formation in burns.
- Fibrinous, when the fibrin content of the fluid exudate is high e.g. in pneumococcal and rheumatic pericarditis.
- Purulent or suppurative exudate is the formation of creamy pus as seen in infection with pyogenic bacteria e.g. abscess, or acute appendicitis.
- Haemorrhagic, when there is vascular damage e.g. acute haemorrhagic pneumonia in influenza.
- Catarrhal, when the surface inflammation of epithelium produces increased secretion of mucus, for example, the common cold.
- Anatomic location of injury: Morphologic changes vary depending upon the anatomic location of the injury i.e. in solid tissues and organs (e.g. hepatitis, pyelonephritis etc), or epithelium-lined surfaces (for example, Colitis, Cholecystitis etc), or serosal surfaces of serous cavities (for example, pleuritis, pericarditis etc).
2. Pseudomembranous Inflammation:
It is an inflammatory response of mucous surface (oral, respiratory, bowel) to toxins of diphtheria or irritant gases. As a result of the denudation of epithelium, plasma exudes on the surface where it coagulates, and together with necrosed epithelium, forms a false membrane that gives this type of inflammation its name.
3. Ulcer:
Ulcers are local defects on the surface of an organ produced by inflammation. Some common sites for ulcerations are the stomach, duodenum, intestinal ulcers in typhoid fever, intestinal tuberculosis, bacillary and amoebic dysentery, ulcers of legs due to varicose veins etc.
In the acute stage, there is infiltration by polymorphs with vasodilatation while long-standing ulcers develop infiltration by lymphocytes, plasma cells and macrophages with associated
fibroblastic proliferation and scarring.
4. Suppuration (Abscess Formation):
When acute bacterial infection is accompanied by intense neutrophilic infiltrate in the inflamed tissue, it results in tissue necrosis.
A cavity is formed which is called an abscess and contains purulent exudate or pus and the process of abscess formation is known as suppuration. The bacteria which cause suppuration are called pyogenic for example, Staphylococcus aureus.
Microscopically, pus is creamy or opaque in appearance and is composed of numerous dead as well as living neutrophils, some red cells, fragments of tissue debris and fibrin. In old pus, macrophages and cholesterol crystals are also present.
An abscess may be discharged to the surface due to increased pressure inside or may require drainage by the surgeon. Due to tissue destruction, the resolution does not occur but instead healing by fibrous scarring takes place.
Some of the common examples of abscesses are as under:
- Boil or furuncle which is an acute inflammation via hair follicles in the dermal tissues.
- Carbuncle is seen in untreated diabetics and occurs as a loculated abscess in the dermis and soft tissues of the neck.
5. Cellulitis:
It is a diffuse inflammation of the soft tissues resulting from the spreading effects of substances like hyaluronidase released by some bacteria.
6. Bacterial Infection Of The Blood:
Bacteria after gaining entry into the blood may produce the following 3 patterns:
- Bacteraemia: Bacteraemia is defined as presence of a small number of bacteria in the blood which do not multiply significantly. They are commonly not detected by direct microscopy. Blood culture is done for their detection for example, Infection with Salmonella typhi, Escherichia coli, and Streptococcus viridans.
- Septicaemia: Septicaemiameans presence of rapidly multiplying, highly pathogenic bacteria in the blood for example, Pyogenic cocci, bacilli of plague etc. Septicaemia is generally accompanied by systemic
effects like toxaemia, multiple small haemorrhages, neutrophilic leucocytosis and disseminated intravascular coagulation (DIC). - Pyaemia: Pyaemia is the dissemination of small septic thrombi in the blood which produce their effects at the site where they travel to be lodged.
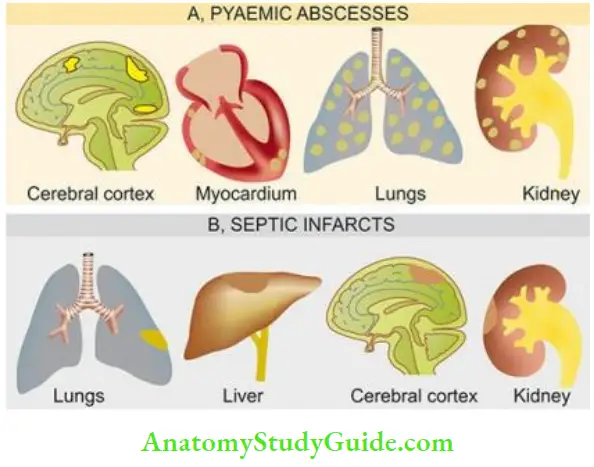
- This can result in pyaemic abscesses or septic infarcts:
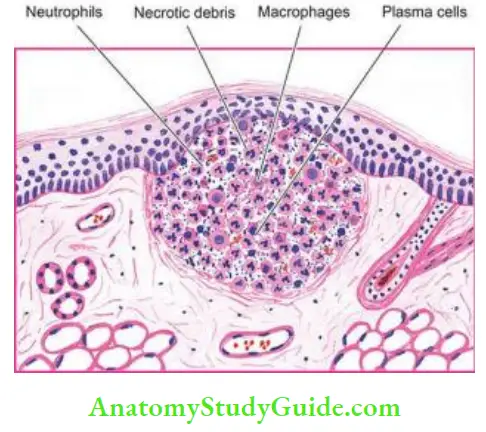
- Pyaemic abscesses: Pyaemic abscesses: are multiple small abscesses in various organs such as in the cerebral cortex, myocardium, lungs and renal cortex, resulting from very small emboli fragmented from septic thrombus.
- Microscopy: Microscopy of pyaemic abscess shows a central zone of necrosis containing numerous bacteria, surrounded by a zone of suppuration and an outer zone of acute inflammatory cells
- Septic infarcts: Septic infarcts result from the lodgement of larger fragments of septic thrombi in the arteries with relatively larger foci of necrosis, suppuration and acute inflammation for example, Septic infarcts of the lungs, liver, brain, and kidneys from septic thrombi of leg veins or from acute bacterial endocarditis.
Systemic Effects Of Acute Inflammation:
The account of acute inflammation given so far now above is based on local tissue responses. However, many examples of acute inflammation are associated with systemic effects as well.
These include fever, leucocytosis, acute phase reactant proteins, lymphangitis-lymphadenitis and shock.
1. Fever: Fever occurs when acute inflammation is accompanied by bacteraemia. The occurrence of fever is mediated through the release of factors like prostaglandins, interleukin-1 and TNF-α in response to infection.
2. Leucocytosis:
A rise in total leucocyte count commonly accompanies acute inflammatory reactions, usually in the range of 15,000-20,000/µl. When the counts are higher than this with ‘shift to left’ of myeloid cells, the blood picture is described as a leukemoid reaction. Usually, leucocytosis in bacterial infections is neutrophilic; in viral infections lymphocytic; and in parasitic infestations, eosinophilic. Typhoid fever, an example of acute inflammation, however, induces leucopenia with relative lymphocytosis.
3. Acute Phase Reactants:
A variety of acute phase reactant (APR) proteins are released in plasma in response to tissue trauma and infection. Their major role is to protect the normal cells from the harmful effects of toxic molecules generated in inflammation and to clear away the waste material.
APRs include the following:
- Certain cellular protection factors (for example, α1-antitrypsin, α1-chymotrypsin, α2-antiplasmin, and plasminogen activator inhibitor): They protect the tissues from cytotoxic and proteolytic damage.
- Some coagulation proteins (for example, Fibrinogen, plasminogen, von Willebrand factor, factor
- They generate factors to replace those consumed in coagulation.
- Transport proteins (for example, Ceruloplasmin, haptoglobin): They carry generated factors.
- Immune agents (for example, Serum amyloid A and P component, C-reactive protein or CRP): CRP is
an opsonising agent for phagocytosis and its levels are a useful indicator of inflammation in the
body. - Stress proteins (for example, Heat shock proteins—HSP, ubiquitin): They are molecular chaperons
which carry the toxic waste within the cell to the lysosomes. - Antioxidants (for example, Ceruloplasmin): Active in the elimination of excess of oxygen free radicals. The APR are synthesised mainly in the liver, and to some extent in macrophages.
APR along with systemic features of fever and leucocytosis is termed ‘acute phase response’. Deficient synthesis of APR leads to severe form of the disease in the form of chronic and repeatedinflammatory responses.
4. Lymphangitis-Lymphadenitis:
The lymphatics and lymph nodes that drain the inflamed tissue show reactive inflammatory changes in the form of lymphangitis and lymphadenitis.
This response represents either a nonspecific reaction to mediators released from inflamed tissue or is an immunologic response to a foreign antigen. The affected lymph nodes may show hyperplasia of lymphoid follicles (follicular hyperplasia) and proliferation of mononuclear phagocytic cells in the sinuses of lymph nodes (sinus histiocytosis).
5. Septic Shock:
Occurrence of shock is a serious manifestation in severe and fulminant cases of acute microbial inflammation. A massive release of cytokine TNF-α, a mediator of inflammation, in response to severe tissue injury or infection results in profuse systemic vasodilatation, increased vascular permeability and intravascular volume loss.
The net effect of these changes is hypotension and shock. Systemic activation of the coagulation pathway may occur leading to microthrombi throughout the body and result in disseminated intravascular coagulation (DIC), bleeding and death.
Outcome Of Acute Inflammation:
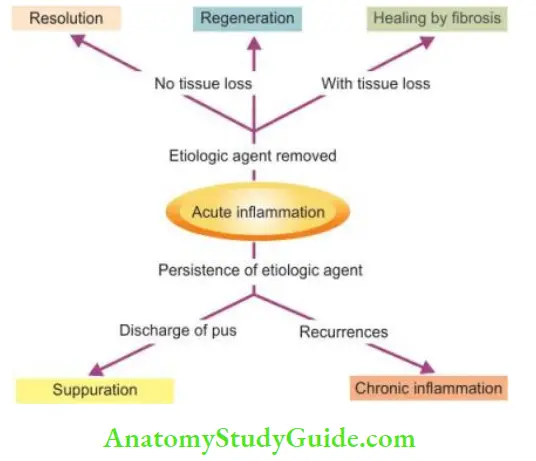
The acute inflammatory process can culminate in one of the following outcomes :
- Resolution: It means a complete return to normal tissue following acute inflammation. This occurs when tissue changes are slight and the cellular changes are reversible for example, in Resolution in lobar pneumonia.
- Fibrous Healing: While superficial injury in acute inflammation results in repair by
regeneration, more extensive tissue injury causing destructive loss of tissue is repaired by healing
with fibrosis. - Suppuration: When the pyogenic bacteria causing acute inflammation result in severe tissue necrosis, the process progresses to suppuration. Initially, there is intense neutrophilic infiltration.
- Subsequently, mixture of neutrophils, bacteria, fragments of necrotic tissue, cell debris and fibrin comprise pus which is contained in a cavity to form an acute abscess.
- The abscess, if not drained, may get organised in time by dense fibrous tissue (chronic abscess), and even get calcified.
- Chronic Inflammation: Persisting or recurrent acute inflammation may progress to chronic inflammation in which the processes of inflammation and repair proceed side by side.
Acute Inflammation — Factors Determining Response, Morphology, Systemic Effects, Outcome:
- There is variation in inflammatory response depending upon factors pertaining to the organisms (type, virulence, dose, route of entry) and host factors (systemic diseases, immune status, defect in neutrophil function, type of tissue).
- In general, inflammation is classified into acute or chronic based on duration, type of tissue affected and type of exudates.
- Morphologic patterns of acute inflammation are various forms of exudates, pseudomembranous inflammation, ulcers, abscesses, cellulitis, and bacterial infection through blood (bacteraemia, septicaemia, pyaemia).
- Besides causing local effects, many examples of acute inflammation produce systemic manifestations such as fever, leucocytosis, realease of acute phase react proteins, lymphangitis-lymphadenitis, and in fulminant cases, septic shock.
- Acute inflammation may have a variety of outcomes: resolution by regeneration, repair by fibrous healing, suppuration, or may progress to chronic inflammation.
Leave a Reply