Nutritional Diseases
Nutritional Requirement:
Table of Contents
The nutritional status of society varies according to the socioeconomic conditions. In the Western world, the nutritional imbalance is more often a problem accounting for increased frequency of obesity, while in developing countries of Africa, Asia and South America, chronic malnutrition is a serious health problem, particularly in children.
Read And Learn More: General Pathology Notes
Before describing nutritional diseases, it is essential to know the components of normal and adequate nutrition. For good health, humans require energy-providing nutrients (proteins, fats and carbohydrates), vitamins, minerals, water and some non-essential nutrients.
Energy:
- The requirement of energy by the body is calculated in Kcal per day.
- In order to retain a stable weight and undertake day-to-day activities, the energy intake must match the energy output.
- The average requirement of energy for an individual is estimated by the formula:
- 900+10w for males, and 700+7w for females (where w stands for the weight of the individual in kilograms).
- Since the requirement of energy varies according to the level of physical activities performed by the person, the figure arrived at by the above formula is multiplied by: 1.2 for a sedentary person, 1.4 for a moderately active person and 1.8 for a very active person.
Proteins:
- Dietary proteins provide the body with amino acids for endogenous protein synthesis and are also a metabolic fuel for energy (1 g of protein provides 4 Kcal).
- Nine essential amino acids (histidine, isoleucine, leucine, lysine, methionine/cystine, phenylalanine/tyrosine, threonine, tryptophan and valine) must be supplied by dietary intake as these cannot be synthesised in the body.
- The recommended average requirement of proteins for an adult is 0.6,g/kg of the desired weight per day. For a healthy person, 10-14% of caloric requirement should come from proteins.
Fats:
- Fats and fatty acids (in particular linolenic, linoleic and arachidonic acid) should comprise about 35% of the diet.
- In order to minimise the risk of atherosclerosis, poly-unsaturated fats should be limited to <10% of calories and saturated fats and trans-fats should comprise <10% of calories while monounsaturated fats to constitute the remainder of fat intake (1 g of fat yields 9 Kcal).
Carbohydrates:
- Dietary carbohydrates are the major source of dietary calories, especially for the brain, RBCs and muscles (1 g of carbohydrate provides 4 Kcal).
- At least 55% of the total caloric requirement should be derived from carbohydrates.
Vitamins:
- These are mainly derived from exogenous dietary sources and are essential for maintaining the normal structure and function of cells.
- A healthy individual requires 4 fat-soluble vitamins (A, D, E and K) and 11 water-soluble vitamins (C, B1 or thiamine, B2 or riboflavin, B 3or niacin/nicotinic acid, B5 or pantothenic acid, B6 or pyridoxine, folate/folic acid, B12 or cyanocobalamin, choline, biotin, and flavonoids).
- Vitamin deficiencies result in individual deficiency syndromes or may be part of a multiple deficiency state.
Minerals:
- A number of minerals like iron, calcium, phosphorus and certain trace elements (for example Zinc, Copper, Selenium, Iodine, Chlorine, Sodium, Potassium, Magnesium, Manganese, Cobalt, and Molybdenum etc) are essential for health.
- Their deficiencies result in a variety of lesions and deficiency syndromes.
Water :
- Water intake is essential to cover the losses in faeces, urine, exhalation and insensible loss so as to avoid under or over-hydration.
- Although the body’s water needs vary according to physical activities and weather conditions, the average requirement of water is 1.0-1.5 ml water/ Kcal of energy spent. Infants and pregnant women have relatively higher requirements for water.
Non-essential nutrients:
- Dietary fibre is composed of cellulose, hemicellulose and pectin, though considered non-essential.
- Important due to their beneficial effects in lowering the risk of colonic cancer, diabetes and coronary artery disease.
Pathogenesis Of Deficiency Diseases
Nutritional deficiency disease develops when essential nutrients are not provided to the cells adequately. Nutritional deficiency may be of 2 types:
- Primary deficiency: This is due to either the lack or decreased amount of essential nutrients in diet.
- Secondary or conditioned deficiency: Secondary or conditioned deficiency is malnutrition occurring as a result of various factors. These are as under:
- Interference with ingestion for example, Gastrointestinal disorders such as malabsorption syndrome, chronic alcoholism, neuropsychiatric illness, anorexia, food allergy, and pregnancy.
- Interference with absorption, for example, Sypermotility of the gut, achlorhydria, and biliary disease.
- Interference with utilisation, for example, Liver dysfunction, malignancy, and hypothyroidism.
- Increased excretion, for example, Lactation, Perspiration, and Polyuria.
- Increased nutritional demand, for example, Fever, pregnancy, lactation, and Hyperthyroidism.
Irrespective of the type of nutritional deficiency (primary or secondary), nutrient reserves in the tissues begin to get depleted, which initially result in biochemical alterations and eventually lead to functional and morphological changes in tissues and organs.
In the following pages, a brief account of nutritional excess (i.e. obesity) is followed by a description of multiple or mixed deficiencies ( for example, Starvation, Protein-energy malnutrition, Metals and trace element deficiency, Disorders of vitamins), and finally, relationship of diet and cancer is presented.
Obesity
Dietary imbalance and overnutrition may lead to obesity. Obesity is defined as an excess of adipose tissue that imparts health risk; a body weight of 20% excess over ideal weight for age, sex and height is considered a health risk. The most widely used method to gauge obesity is body mass index (BMI) which is equal to weight in kg/height in m2. A cut-off BMI value of 30 is used for obesity in both men and women.
Etiology:
Obesity results when caloric intake exceeds utilisation. The imbalance of these two components can occur in the following situations:
- Inadequate pushing of oneself away from the dining table causes overeating.
- Insufficient pushing of oneself out of the chair leads to inactivity and a sedentary lifestyle.
- Genetic predisposition to develop obesity.
- Diets are largely derived from carbohydrates and fats than protein-rich diets.
- Secondary obesity may result following a number of underlying diseases such as hypothyroidism, Cushing’s disease, insulinoma and hypothalamic disorders.
Pathogenesis:
The lipid storing cells, adipocytes comprise the adipose tissue and are present in vascular and stromal compartments in the body.
Besides the generally accepted role of adipocytes for fat storage, these cells also release endocrine-regulating molecules.
- These molecules include energy regulatory hormone (leptin), cytokines (TNF-α and interleukin-6), insulin sensitivity regulating agents (adiponectin, resistin and RBP4), prothrombotic factors (plasminogen activator inhibitor), and blood pressure regulating agent (angiotensinogen).
- Adipose mass is increased due to the enlargement of adipose cells due to excess of intracellular lipid deposition as well as due to increase in the number of adipocytes.
- The most important environmental factor is excess consumption of nutrients which can lead to obesity.
- However, underlying molecular mechanisms of obesity are beginning to unfold based on observations that obesity is familial and is seen in identical twins.
- Recently, two obesity genes have been found: The ob gene and its protein product leptin, and the db gene and its protein product leptin receptor.
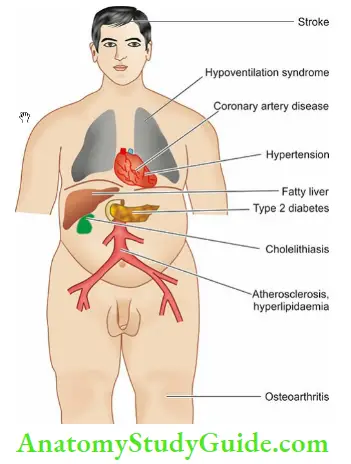
Sequelae Of Obesity:
Marked obesity is a serious health hazard and may predispose to a number of clinical disorders and pathological changes described below and illustrated in.
Morphologic Features:
Obesity is associated with increased adipose stores in the subcutaneous tissues, skeletal muscles, and internal organs such as the kidneys, heart, liver and omentum; fatty liver is also more common in obese individuals. There is an increase in both size and number of adipocytes i.e. there is hypertrophy as well as hyperplasia.
Effects Of Obesity:
These are as under:
- Hyperinsulinaemia: Increased insulin secretion is a feature of obesity. Many obese individuals exhibit hyperglycaemia or frank diabetes despite hyperinsulinaemia. This is due to a state of insulin resistance consequent to tissue insensitivity.
- Type 2 diabetes mellitus: There is a strong association of type 2 diabetes mellitus with obesity. Obesity often exacerbates the diabetic state and in many cases weight reduction often leads to amelioration of diabetes.
- Hypertension: A strong association between hypertension and obesity is observed which is perhaps due to increased blood volume. Weight reduction leads to significant reduction in systolic blood pressure.
- Hyperlipoproteinaemia: The plasma cholesterol circulates in the blood as low-density lipoprotein (LDL) containing most of the circulating triglycerides. Obesity is strongly associated with VLDL and mildly with LDL. Total blood cholesterol levels are also elevated in obesity.
- Atherosclerosis: Obesity predisposes to the development of atherosclerosis. As a result of atherosclerosis and hypertension, there is increased risk of myocardial infarction and stroke in obese individuals.
- Nonalcoholic fatty liver disease (NAFLD): Obesity contributes to the development of NAFLD which may progress further to cirrhosis of the liver.
- Cholelithiasis: There is a six times higher incidence of gallstones in obese persons, mainly due to increased total body cholesterol.
- Hypoventilation syndrome (Pickwickian syndrome): This is characterised by hypersomnolence, both at night and during the day in obese individuals along with carbon dioxide retention, hypoxia, polycythaemia and eventually right-sided heart failure (Mr Pickwick was a character, fat boy, in Charles Dickens’s Pickwick Papers. The term Pickwickian syndrome was first used by Sir William Osler for the sleep-apnoea syndrome).
- Osteoarthritis: These individuals are more prone to develop degenerative joint disease due to , wear and tear following trauma to joints as a result of large body weight.
- Cancer: Diet rich in fats, particularly derived from animal fats and meats, is associated with higher incidence of cancers of the colon, breast, endometrium and prostate.
Starvation
Starvation is a state of overall deprivation of nutrients. Its causes may be the following:
- Deliberate fasting—religious or political
- Famine conditions in a country or community, or
- Secondary undernutrition such as due to chronic wasting diseases (infections, inflammatory conditions, liver disease), cancer etc.
- Cancer results in malignant cachexia as a result of which cytokines are elaborated for example ,Tumour necrosis factor-α, Elastases, Proteases etc.
A starved individual has lax, dry skin, wasted muscles and atrophy of internal organs:
Metabolic Changes
The following metabolic changes take place in starvation:
Glucose: Glucose stores of the body are sufficient for one day’s metabolic needs only.
- During fasting state, insulin-independent tissues such as the brain, blood cells and renal medulla continue to utilise glucose while insulin-dependent tissues like muscle stop taking up glucose.
- This results in the release of glycogen stores of the liver to maintain normal blood glucose levels.
- Subsequently, hepatic gluconeogenesis from other sources such as the breakdown of proteins takes place.
Proteins:
- Protein stores and the triglycerides of adipose tissue have enough energy for about 3 months in an individual.
- Proteins break down to release amino acids which are used as fuel for hepatic gluconeogenesis so as to maintain the glucose needs of the brain.
- This results in nitrogen imbalance due to the excretion of nitrogen compounds as urea.
Fats:
- After about one week of starvation, protein breakdown is decreased while triglycerides adipose tissue breakdown to form glycerol and fatty acids.
- The fatty acids are converted into ketone bodies in the liver which are used by most organs including brain in place of glucose.
- Starvation can then continue till all the body fat stores are exhausted following which death occurs.
Protein-Energy Malnutrition
The inadequate consumption of protein and energy as a result of primary dietary deficiency or conditioned deficiency may cause loss of body mass and adipose tissue, resulting in protein energy or protein-calorie malnutrition (PEM or PCM).
The primary deficiency is more frequent due to socioeconomic factors limiting the quantity and quality of dietary intake, particularly prevalent in the developing countries of Africa, Asia and South America. The impact of deficiency is marked in infants and children.
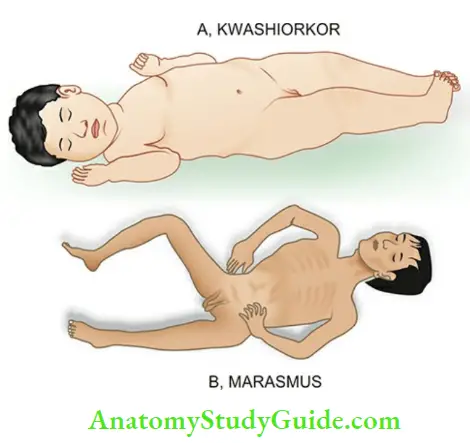
The spectrum of clinical syndromes produced as a result of PEM includes the following:
- Kwashiorkor which is related to protein deficiency though calorie intake may be sufficient.
- Marasmus is starvation in infants occurring due to overall lack of calories.
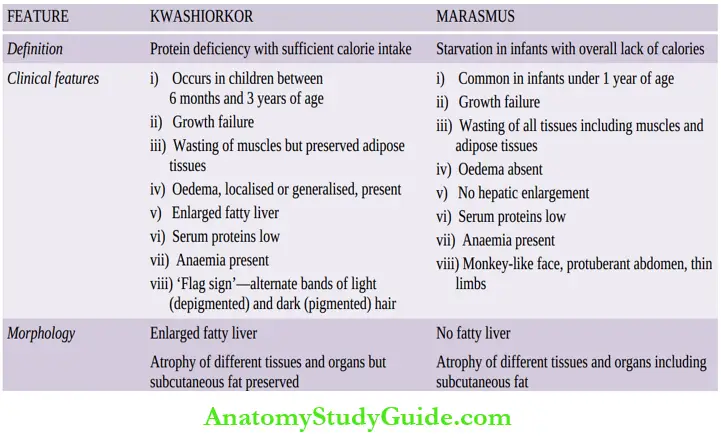
The salient features of the two conditions are contrasted in Table. However, it must be remembered that mixed forms of kwashiorkor-marasmus syndrome may also occur.
Metals And Trace Elements
Several minerals in trace amounts are essential for health since they form components of enzymes and cofactors for metabolic functions.
Besides calcium and phosphorus required for vitamin D manufacture, others include:
- Iron
- Copper
- Iodine, Zinc
- Selenium
- Manganese
- Nickel
- Chromium
- Molybdenum
- Fluorine.
However, out of these, the dietary deficiency of the first five trace elements is associated with deficiency states later.
These are as under:
- Iron: Microcytic hypochromic anaemia.
- Calcium: Reduced bone mass, osteoporosis.
- Phosphorus: Rickets, osteomalacia.
- Copper: Muscle weakness, neurologic defect, anaemia, growth retardation.
- Iodine: Goitre and hyperthyroidism, cretinism.
- Zinc: Growth retardation, infertility, alopecia.
- Selenium: Cardiomyopathy, muscle degeneration.
- Fluoride: Dental caries.
- Manganese: Impaired growth and skeletal development.
- Molybdenum: Severe neurological abnormalities.
Nutritional Diseases:
- For good health, humans require energy-providing nutrients (proteins, fats and carbohydrates), vitamins, minerals, water and some non-essential nutrients.
- The nutritional deficiency may be primarily due to either the lack or decreased amount of essential nutrients in diet, or secondary or conditioned deficiency occurring as a result of various factors such as interference in ingestion, absorption, excretion, or increased nutritional demand.
- Dietary imbalance and overnutrition may lead to obesity. Effects of obesity are hyperinsulinaemia, type 2 diabetes, hypertension, atherosclerosis, non-alcoholic fatty liver disease, cholelithiasis, hyperventilation, and osteoarthritis.
- Starvation is a state of overall deprivation of nutrients i.e. glucose, proteins and fats. Inadequate consumption of protein and energy cause loss of body mass and adipose tissue, resulting in protein energy or protein-calorie malnutrition (PEM or PCM).
It is of 2 types:
- Kwashiorkor which is related to protein deficiency though calorie intake may be sufficient, and marasmus which is starvation in infants occurring due to overall lack of calories.
- Besides calcium and phosphorus, several trace elements required in diet may produce deficiency states. The most important ones are due to iron, copper, iodine and zinc.
Contrasting features of kwashiorkor and marasmus:
Leave a Reply