The Breast
Normal Structure
Microanatomy of the breast reveals 2 types of tissue components epithelial and stromal. In a fully-developed non-lactating female breast, the epithelial component comprises less than 10% of the total volume but is more significant pathologically since the majority of lesions pertain to this portion of the breast.
Table of Contents
Epithelial Component: The epithelial component of the breast consists of 2 major parts terminal duct-lobular unit (Tdlu) which performs the main secretory function during lactation and a large duct system which performs the function of collection and drainage of secretions; both are interconnected to each other.
Read And Learn More: Systemic Pathology Notes
- The breast is divided into about 20 lobes. Each lobe consists of breast lobules which drain
their secretions through its collecting duct system and opens into the nipple through its own main excretory duct, the lactiferous duct. - The segment of the lactiferous duct subjacent to the nipple shows a small dilatation called a lactiferous sinus.
- Each lactiferous duct has its own collecting duct system which has branches of smaller diameter, ultimately terminating peripherally as terminal ducts (or Tdlu) in the breast lobules.
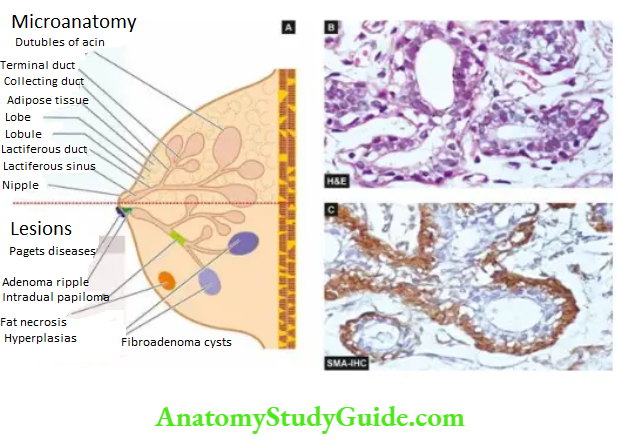
- The entire ductal-lobular epithelial system has a bilayered lining: the inner epithelium with secretory and absorptive function, and an outer supporting myoepithelial lining, both having characteristic ultrastructure and immunoreactivity.
- The inner epithelium stains are positive for epithelial membrane antigen (EMA) and lactalbumin while the myoepithelium is positive for smooth muscle actin (SMA) and S-100.
Stromal Component: The supportive stroma of the breast consists of a variable amount of loose connective tissue and adipose tissue during different stages of reproductive life.
- The stromal tissue of the breast is present at 2 locations intralobular and interlobular stroma. Intralobular stroma encloses each lobule, and its acini and ducts, and is chiefly made of loose connective tissue, myxomatous stroma and a few scattered lymphocytes.
- Interlobular stroma separates one lobule from the other and is composed mainly of adipose tissue and some loose connective tissue.
- The most important disease of the breast is cancer. However, there are a few inflammatory lesions, benign tumours and tumour-like lesions which may be confused clinically with breast cancer. These pathologic lesions are described first, followed by an account of breast cancer.
Inflammatory Conditions
Inflammation of the breast is called mastitis. Important types of mastitis are acute mastitis and breast abscess, chronic mastitis, mammary duct ectasia (or plasma cell mastitis), traumatic fat necrosis and galactocele.
Acute Mastitis And Breast Abscess:
- Acute pyogenic infection of the breast occurs chiefly during the first few weeks of lactation and sometimes by eczema of the nipples.
- Bacteria such as staphylococci and streptococci gain entry into the breast by the development of cracks and fissures in the nipple.
- Initially, a localised area of acute inflammation is produced which, if not effectively treated, may cause single or multiple breast abscesses.
- Extensive necrosis and replacement by fibrous scarring of the breast with retraction of the nipple may result.
Granulomatous Mastitis:
Although chronic non-specific mastitis is uncommon, chronic granulomatous inflammation in the breast may occur as a result of the following:
- Systemic non-infectious granulomatous disease example as part of systemic sarcoidosis, Wegener’s granulomatosis.
- Infections example tuberculosis which is not so uncommon in developing countries like India and may be misdiagnosed clinically as breast cancer owing to axillary nodal involvement. Tubercle bacilli reach the breast by haematogenous, lymphatic or direct spread, usually from the lungs or pleura.
- Pathologically, typical caseating tubercles with discharging sinuses through the surface of
the breast are found. ZN staining may demonstrate acid-fast bacilli. - Fungal infection of the breast may occur in immunocompromised patients. Actinomycosis infection of the breast may also incite granulomatous inflammation.
- Pathologically, typical caseating tubercles with discharging sinuses through the surface of
- Silicone breast implants implanted on breast cancer patients after mastectomy or as breast augmentation cosmetic surgery may rupture or silicone may slowly leak into surrounding breast tissue.
- This incites chronic inflammatory reactions of lymphocytes, macrophages and foreign body giant cells. Eventually, a surrounding fibrous capsule forms and after a long period it may even be calcified.
- Idiopathic granulomatous mastitis is an uncommon form of reaction around lobules and ducts in the absence of any known aetiology.
- The exact pathogenesis is not known but probably it is a form of hypersensitivity reaction to the luminal secretion of the breast epithelium during lactation.
Mammary Duct Ectasia:
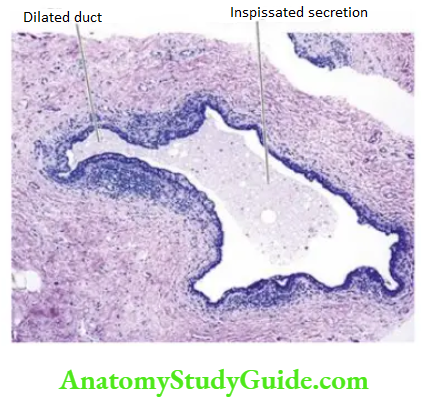
- Mammary duct ectasia is a condition in which one or more of the larger ducts of the breast are dilated and filled with inspissated secretions. These are associated with periductal and interstitial chronic inflammatory changes.
- Duct ectasia affects women in their 4th to 7th decades of life. The patients may remain asymptomatic or there may be nipple discharge, retraction of the nipple due to fibrous scarring and clinically palpable dilated ducts in the subareolar area.
- The lesion may be mistaken for carcinoma of the breast. The etiology of the condition remains unknown but it begins with dilatation and rupture of ducts which incites periductal inflammation, followed by periductal fibrosis.
- Plasma cell mastitis is a variant of duct ectasia or periductal mastitis. It occurs a few years following cessation of lactation.
Grossly, the condition appears as a single, poorly-defined indurated area in the breast with ropiness on the surface. The cut section shows dilated ducts containing cheesy inspissated secretions.
Histologically, the features are as under:
- Dilated ducts with either necrotic or atrophic lining by flattened epithelium and lumen containing granular, amorphous, pink debris and foam cells.
- Periductal and interstitial chronic inflammation, chiefly lymphocytes, and histiocytes with multinucleate histiocytic giant cells.
- Periductal fibrosis and hyperelastosis.
- Occasionally, there may be the obliteration of the ducts by fibrous tissue and a varying amount of inflammation which is termed obliterative mastitis.
- In plasma cell mastitis, the infiltrate has an impressive number of plasma cells, or sometimes a granulomatous reaction.
Fat Necrosis:
Focal fat necrosis in an obese woman with pendulous breasts is generally initiated by trauma that
is followed by an inflammatory reaction. The condition presents as a well-defined mass with indurated appearance.
Grossly, the excised lump has a central pale cystic area of necrosis.
Histologically, there is disruption of the regular pattern of lipocytes with the formation of lipid-filled spaces surrounded by neutrophils, lymphocytes, plasma cells and histiocytes having foamy cytoplasm and frequent foreign body giant cell formation. In the late stage, there is replacement fibrosis and even calcification.
Galactocele:
A galactocele is a cystic dilatation of one or more ducts occurring during lactation. The mammary duct is obstructed and dilated to form a thin-walled cyst filled with milky fluid. Rarely, the wall of the galactocele may get secondarily infected.
Inflammatory Conditions:
- Acute pyogenic infection of the breast (mastitis) during lactation or eczema of the nipple, if not treated timely, may be followed by chronic mastitis or abscess.
- Mammary duct ectasia involves one or more of the larger ducts of the breast which are dilated and filled with inspissated secretions, followed by periductal inflammation.
- Plasma cell mastitis is in its variant form.
- Granulomatous mastitis may occur following microbial infections, implants, noninfectious inflammatory conditions or may be idiopathic.
- Fat necrosis of the breast may occur following trauma.
- Galactocele is a cystic dilatation of one or more ducts during lactation.
Benign Epithelial Proliferations
Benign proliferative conditions include two entities: fibrocystic lesions, and gynaecomastia in male breast.
Fibrocystic Lesions:
This group includes various conditions which have the common benign proliferation of epithelial components of the breast. As per the latest WHO histologic classification of breast tumours, the following terms are proposed for epithelial changes and associated fibrosclerosis:
- Epithelial hyperplasia (without or with atypia)
- Adenosis (types: sclerosing, apocrine, micro glandular)
- Radial scar (or complex sclerosing lesion)
In a given case, these pathologic changes may be present in varying combinations and proportions. It is important to identify the spectrum of histologic features by core needle biopsy or cytologic findings by Fnac in fibrocystic changes since only a certain subset of changes have an increased risk of development of breast cancer. Accordingly, these epithelial lesions are discussed below under three headings:
- Non-proliferative fibrocystic change
- Proliferative fibrocystic disease without atypia
- Proliferative fibrocystic disease with atypia (atypical ductal hyperplasia)
- It may be noted from the above nomenclature that the first group has a suffix ‘change’ which may be physiological but the second and third groups have a suffix ‘disease’ due to the clinicopathologic significance of epithelial proliferation and presence or absence of atypia.
- Fibrocystic changes are quite common benign breast lesions and are frequently bilateral, producing vague ‘lumpy’ breasts rather than a palpable lump in the breast.
- Its incidence has been reported to range from 10-20% in adult women, most often between 3rd and 5th decades of life, with a dramatic decline in its incidence after menopause suggesting the role of oestrogen in its pathogenesis.
- It was previously termed benign mammary dysplasia but it is currently known that all forms of fibrocystic changes are neither a disease nor dysplasia.
Non-Proliferative Fibrocystic Change:
- Non-proliferative fibrocystic change, also called simple fibrocystic change, is regarded as a physiologic change. It includes three common features formation of cysts of varying size, increase in fibrous stroma and adenosis.
- Cysts are formed by dilatation of obstructed collecting ducts, obstruction being caused by periductal fibrosis following inflammation or fibrous overgrowth from oestrogen stimulation.
Morphologic Features Grossly, the cysts are rarely solitary but are usually multifocal and bilateral. They vary from microcysts to 5-6 cm in diameter.
Usually, the large cyst is rounded, and translucent with bluish colour prior to opening (blue-dome cyst). On opening, the cyst contains thin serous to haemorrhagic fluid.
Microscopically, simple fibrocystic change includes the following features:
- Cyst formation There is the distortion of terminal ductular lobular units and the formation of cysts. The lining of cysts may show a variety of appearances flattened, atrophic, apocrine change or apocrine metaplasia.
- Fibrosis There is increased fibrous stroma surrounding the cysts and a variable degree of stromal lymphocytic infiltrate.
- Adenosis refers to the proliferation of lobular units per TDLU. Adenosis is a normal process during pregnancy and lactation. In fibrocystic change, adenosis may be focally present which is lined by benign columnar cells however, when it shows proliferation and atypia in lining cells, it may be an early precursor lesion of breast cancer.
Proliferative Fibrocystic Disease Without Atypia:
Proliferative fibrocystic disease of the breast without atypia includes three entities: epithelial hyperplasia, sclerosing adenosis, and complex sclerosing lesion (or radial scar):
1. Epithelial Hyperplasia: or epithelioid is defined as an increase in the layers of epithelial cells over the basement membrane to four or more layers in the ducts or lobules:
- In the ducts, it is called epithelial ductal hyperplasia or usual ductal hyperplasia. When
benign intraductal epithelial proliferation forms papillary structures in the ducts, it is called
ductal papillomatosis. - In the lobules, it is termed lobular hyperplasia, a condition that must be distinguished from adenosis in which there is an increase in the number of ductules or acini.
Microscopically, epithelial hyperplasia is characterised by epithelial proliferation more than its normal double layer without architectural abnormalities or cytologic atypia; however, the proliferated cells are variable in shape and size:
- Mild hyperplasia of ductal epithelium consists of 2-4 layers of cells above the basement membrane, present focally or evenly throughout the duct.
- Moderate hyperplasia is the proliferation of 4 or more layers of benign ductal epithelium over the basement membrane.
- Florid hyperplasia is associated with a tendency to fill the ductal lumen with proliferated epithelium. It may have one of the two patterns:
- a solid pattern filling the entire lumen with cells, and
- the cribriform pattern forming fenestrations in the proliferated cells in ductal lumina.
- Ductal papillomatosis is focal benign epithelial proliferations into the lumina of ducts, forming papillary epithelial projections over the fibrovascular core.
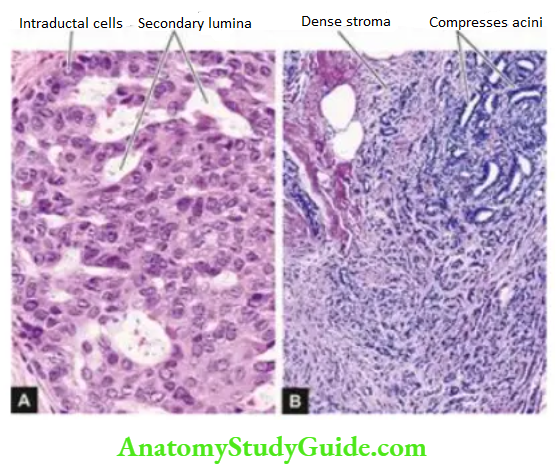
2. Sclerosing Adenosis: a benign proliferation of distorted ductules or acini and dense stromal fibrosis. The lesion may be present as diffusely scattered microscopic foci in the breast parenchyma or may form an isolated palpable mass which may simulate an infiltrating carcinoma, both clinically and pathologically.
Grossly, the lesion may be coexistent with other components of fibrocystic disease or may form an isolated mass which has hard cartilage-like consistency, resembling an infiltrating carcinoma.
Microscopically, there is the proliferation of ductules or acini and fibrous stromal overgrowth. The histologic appearance may superficially resemble infiltrating carcinoma but differs from the latter in having maintained lobular pattern and lack of infiltration into the surrounding fat.
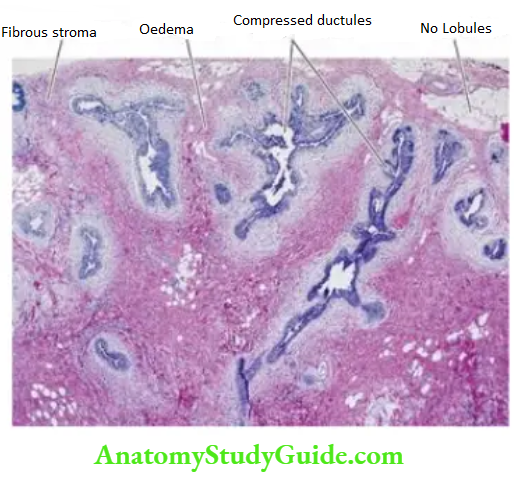
3. Complex Sclerosing Lesion (Radial Scar): It is a variant of sclerosing adenosis having stellate-shaped architecture and is larger than sclerosing adenosis.
Grossly, the lesion is a stellate-shaped scar with central sclerosis and elastosis.
Microscopically, the ducts are obliterated and compressed into tubular structures due to dense scarring. These ducts appear to radiate as tubular lumina from the centre.
The epithelial cells lining these compressed ducts may have variable degrees of hyperplasia, adenosis and cystic dilatation. This entity superficially mimics infiltrating carcinoma but the pattern is best appreciated under low-power microscopy.
Proliferative Fibrocystic Disease With Atypia (Atypical Hyperplasia)
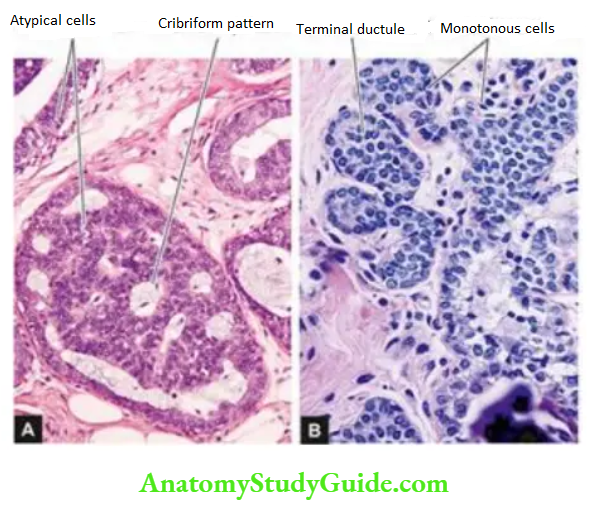
Atypical hyperplasia is characterised by the proliferation of epithelial cells with some architectural and cytologic features suggestive of malignancy but not diagnostic of carcinoma in situ (ductal or DCIS, lobular or LCIS).
Grossly, the lesion may be solitary or multicentric and is usually small (2-3 mm).
Microscopically, the atypical hyperplasia may be ductal or lobular type.
- Atypical ductal hyperplasia (Adh) has the following features:
- Ducts are filled with proliferated cells that may form various patterns: solid, cribriform (sharply punched out spaces), microcapillary, tufts, or cellular bridges.
- Individual cells are relatively monomorphic and admixed with foci of hyperplasia without atypia.
- Small size is considered by many workers as a criterion for distinction from DCIS. Atypical lobular hyperplasia (ALH) is usually an incidental finding in a core biopsy. The features resemble LCIS but the changes are not present uniformly throughout the lobule.
- Proliferated cells occupy 50% or more of the acini in a lobule.
- Involved acini in a TDLU are slightly distended with cells i.e. shape of acini containing proliferated epithelial cells is similar to uninvolved acini.
- Intracytoplasmic mucin is not present.
- The cells are small, monotonous and loosely cohesive.
Prognostic Significance:
The degree and type of epithelial and mesenchymal changes in fibrocystic lesions have variable prognostic implications as under:
- Simple fibrocystic change or non-proliferative fibrocystic change does not carry any increased risk of developing invasive breast cancer later.
- Proliferative fibrocystic disease without atypia (or benign proliferative disease) cases have a 1.5 to 2 times increased risk for the development of invasive breast cancer.
- Proliferative fibrocystic disease with atypia (or atypical hyperplasia): Both ADH and ALH cases have a 4-5 higher risk of developing breast cancer later; in addition, ALH has a higher risk of ipsilateral breast involvement. Patients with a family history of breast cancer are still at higher risk.
Gynaecomastia:
Gynaecomastia is a unilateral or bilateral enlargement of the male breast. Since the male breast does not contain secretory lobules, the enlargement is mainly due to the proliferation of ducts and increased periductal stroma.
Gynaecomastia occurs in response to hormonal stimulation, mainly oestrogen. Such excessive oestrogenic activity in males is seen in young boys between 13 and 17 years of age (pubertal gynaecomastia), in men over 50 years (senescent gynaecomastia), in endocrine diseases associated with increased oestrogenic or decreased androgenic activity example in hepatic cirrhosis, testicular tumours, pituitary tumours, carcinoma of the lung, exogenous oestrogen therapy as in carcinoma of the prostate and testicular atrophy in Klinefelter’s syndrome (secondary gynecomastia), and lastly, enlargement without any obvious cause (idiopathic gynecomastia).
Morphologic Features Grossly, one or both the male breasts are enlarged having smooth glistening white tissue.
Microscopically, there are 2 main features:
- The proliferation of branching ducts displays epithelial hyperplasia with the formation of papillary projections at places.
- Increased fibrous stroma with, myxoid appearance.
Benign Epithelial Proliferations:
- Fibrocystic lesions of the breast are of three types: nonproliferative fibrocystic change, proliferative fibrocystic disease without atypia, and proliferative fibrocystic disease out atypia,
- Fibrocystic change of the breast is characterised by cystic dilatation of terminal ducts, a relative increase in inter- and intralobular fibrous tissue, and adenosis. It does not carry any increased risk of breast cancer development later.
- Proliferative fibrocystic disease without atypia is characterised by usual epithelial hyperplasia of variable degree, sclerosing adenosis and radial scar (complex sclerosing lesion). These changes have a 1.5 to 2 times higher risk of breast cancer later.
- Proliferative fibrocystic disease with atypia is characterised by ductal or lobular atypical hyperplasia (ADH or ALH). This group of changes has a 4 to 5 times increased risk of breast cancer development later.
- Unilateral or bilateral enlargement of the male breast is known as gynecomastia; it is mainly due to the proliferation of ducts and increased periductal stroma.
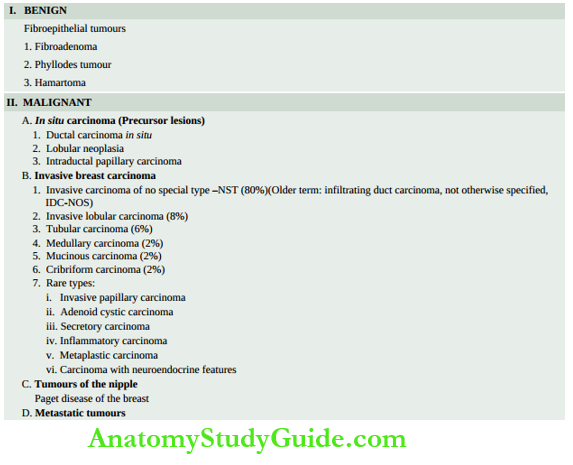
Benign Fibroepithelial Tumours
Two main examples of fibroepithelial (biphasic) tumours of the breast are fibroadenoma and phyllodes tumour. Besides, a benign papillary tumour, intraductal papilloma, is also discussed here.
Fibroadenoma:
- Fibroadenoma or adenofibroma is a benign biphasic tumour of fibrous and epithelial elements. It is the most common benign tumour of the female breast. Though it can occur at any age during reproductive life, most patients are between 15 to 30 years of age.
- Clinically, fibroadenoma generally appears as a solitary, discrete, freely mobile nodule within the breast. Rarely, a fibroadenoma may contain in situ or invasive lobular or ductal carcinoma, or the carcinoma may invade the fibroadenoma from the adjacent primary breast cancer.
Morphologic Features Grossly, a typical fibroadenoma is a small (2-4 cm diameter), solitary, well-encapsulated, spherical or discoid mass. The cut surface is firm, grey-white, slightly myxoid and may show slit-like spaces formed by compressed ducts. Occasionally, multiple fibroadenomas may form part of fibrocystic disease and are termed fibroadenomatosis.
- Less commonly, a fibroadenoma may be fairly large in size, up to 15 cm in diameter, and is called a giant fibroadenoma but lacks the histologic features of osteosarcoma phyllodes (discussed later).
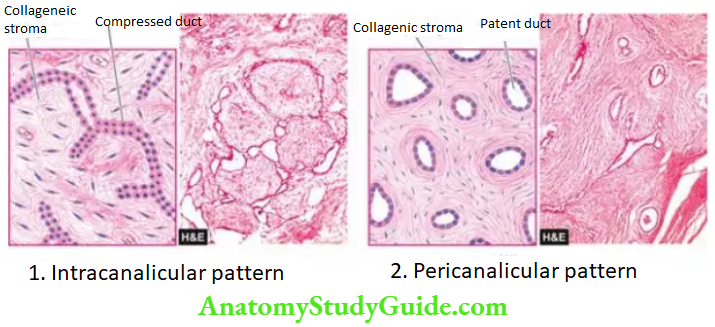
- Microscopically, fibrous tissue comprises most of a fibroadenoma. The arrangements between fibrous overgrowth and ducts may produce two types of patterns which may coexist in the same tumour. These are intracanalicular and pericanalicular patterns:
- Intracanalicular pattern: is one in which the stroma compresses the ducts so that they are reduced to slit-like clefts lined by ductal epithelium or may appear as cords of epithelial elements surrounding masses of fibrous stroma.
- Pericanalicular pattern: is characterised by encircling masses of fibrous stroma around the patent or dilated ducts.
- The fibrous stroma may be quite cellular, or there may be areas of hyalinised collagen. Sometimes, the stroma is loose and myxomatous.
Variants: A few morphologic variants of fibroadenomas have been described:
- Complex fibroadenoma is composed of cysts>3 mm in size, sclerosing adenosis, calcifications and papillary apocrine hyperplasia.
- Juvenile fibroadenoma is an uncommon variant of fibroadenoma which is a larger and rapidly growing mass seen in adolescent girls but fortunately does not recur after excision.
- Occasionally, the fibrous tissue element in the tumour is scanty, and the tumour is instead predominantly composed of closely-packed ductular or acinar proliferation; this is termed a tubular adenoma. Similarly, if an adenoma is composed of acini with secretory activity, it is called lactating adenoma seen during pregnancy or lactation.
- Unlike fibroadenoma, both tubular adenoma and lactating adenomas are not true biphasic tumours but are actually examples of benign epithelial hyperplasia but are listed here since they are named adenomas.
Phyllodes Tumour:
- Cystosarcoma phyllodes was the nomenclature given by Müller in 1838 to an uncommon bulky breast tumour with a leaf-like gross appearance (phyllodes=leaf-like) having aggressive clinical behaviour. Most patients are between 30 to 70 years of age.
- Grossly, the tumour resembles a giant fibroadenoma but is distinguished histologically from the latter by more cellular connective tissue. Later, the WHO classification of breast tumours proposed the term ‘phyllodes tumour’ in place of the misleading term ‘osteosarcoma phyllodes’.
- Phyllodes tumours can be classified into benign, borderline and malignant on the basis of histologic features of stromal cells. Local recurrences are much more frequent than metastases.
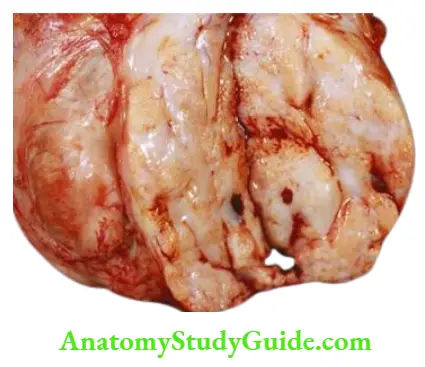
Morphologic Features Grossly, the tumour is generally large, 10-15 cm in diameter, round to oval, bosselated, and less fully encapsulated than a fibroadenoma. The cut surface is grey-white with cystic cavities, areas of haemorrhages, necrosis and degenerative changes.
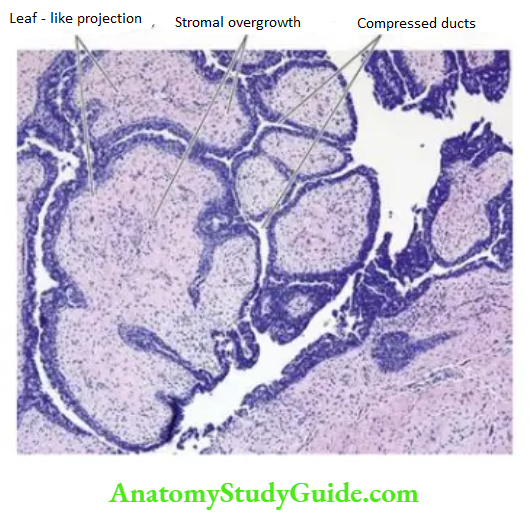
Histologically, the phyllodes tumour is composed of an extremely hypercellular stroma, accompanied by benign compressed ductal structures. Thus, the phyllodes tumour resembles fibroadenoma except for a leaf-like pattern of growth due to marked intracanalicular stromal proliferation.
The histologic criteria considered to distinguish benign, borderline and malignant categories of phyllodes tumours are based on the following cellular features of stroma:
- frequency of mitoses,
- cellular atypia,
- degree of stromal hypercellularity, and
- infiltrative margins.
About 20% of phyllodes tumours are histologically malignant and less than half of them may metastasise.
Intraductal Papilloma:
Intraductal papilloma is a benign papillary tumour occurring most commonly in a lactiferous duct or lactiferous sinus near the nipple. Clinically, it produces serous or serosanguineous nipple discharge. It is most common in 3rd and 4th decades of life.
Morphologic Features Grossly, intraductal papilloma is usually solitary, small, less than 1 cm in diameter, and commonly located in the major mammary ducts close to the nipple. Less commonly, there is multiple papillomatosis which is more frequently related to papillary carcinoma.
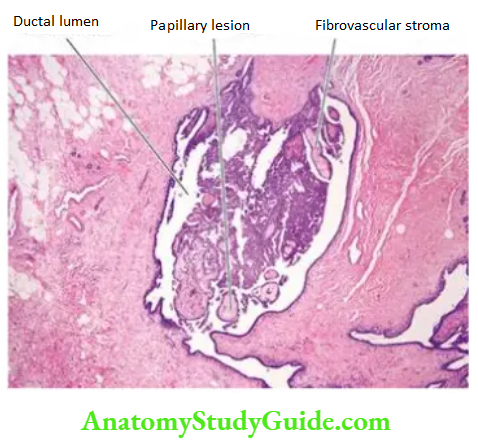
Histologically, an intraductal papilloma is characterised by multiple papillae having well-developed fibrovascular stalks attached to the ductal wall and covered by benign cuboidal epithelial cells supported by myoepithelial cells.
An intraductal papillary carcinoma is distinguished from intraductal papilloma in having severe cellular atypia, pleomorphism, absence of myoepithelial cells, multilayering and presence of mitotic.
Benign Fibroepithelial Tumours:
- Fibroadenoma is a benign biphasic tumour of fibrous and epithelial elements and is the most common benign tumour of the female breast at a young age.
- Phyllodes tumour is a large tumour having leaf-like stromal overgrowth and compressed ductules. It can be classified into benign, borderline and malignant on the basis of the histologic features of stromal cells.
- Intraductal papilloma is a benign tumour of the lactiferous sinus in the nipple having papillary architecture.
Carcinoma In Situ And Invasive Breast Cancer
Cancer of the female breast is among the commonest of human cancers throughout the world. Its incidence varies in different countries. In the United States, carcinoma of the breast constitutes about 25% of all cancers in females and causes approximately 20% of cancer deaths among females.
- However, there has been some decline in mortality from breast cancer in recent years in developed countries due to both early diagnosis and modern therapy.
- Cancer of the male breast, on the other hand, is quite rare and comprises 0.2% of malignant tumours (the ratio between male-female breast cancer is 1:150).
- The incidence of breast cancer is highest in the perimenopausal age group and is uncommon before the age of 25 years.
- Clinically, breast cancer usually presents as a solitary, painless, palpable lump which is detected quite often by self-examination. The higher the age, the more the chances of breast lump turning out to be malignant.
- Thus, all breast lumps, irrespective of the age of the patient must be removed surgically. Currently, the emphasis is on early diagnosis by triple approach palpation, mammography, and fine needle aspiration cytology (Fnac).
- Additional techniques such as stereotactic biopsy and frozen section are immensely valuable to the surgeon for immediate pathological diagnosis in doubtful cases.
Risk (Epidemiologic) Factors:
Many risk factors have been identified for the development of breast cancer in women:
1. Geographic and racial factors: The incidence of breast cancer is about 4-6 times higher in developed countries (North America, North Europe, Australia), intermediate in Southern European and Latin American countries, and low in developing countries of Asia and Africa, with the exception of Japan.
- Breast cancer in Hispanic and African-American women tends to occur at an earlier age and the disease is more advanced at presentation.
- These geographic and racial differences are considered to be related to modifiable risk factors such as diet and environment because immigrants to the US or their daughters have an incidence at par with the local population.
2. Family history: First-degree relatives (mother, sister, daughter) of women with breast cancer have a 2 to 6-fold higher risk of developing of breast cancer. The risk is proportionate to a few factors:
- Number of blood relatives with breast cancer.
- Younger age at the time of development of breast cancer.
- Bilateral cancers.
- High-risk cancer families having breast and ovarian carcinomas.
3. Menstrual and obstetric history: Total length of menstrual life is directly related to increased risk. Thus, there is an increased risk of breast cancer development in women who had early menarche, nulliparity, late age of first childbirth and delayed menopause.
4. Fibrocystic change, particularly when associated with atypical epithelial hyperplasia, has about a 5-fold higher risk of developing breast cancer subsequently.
5. Miscellaneous factors: These include a host of following environmental influences and dietary factors associated with increased risk of breast cancer:
- Consumption of large amounts of animal fats, high-calorie foods
- Cigarette smoking
- Alcohol consumption
- Breast augmentation surgery
- High breast density
- Exposure to ionising radiation during breast development
Identification of a transmissible retrovirus in the early 20th century, mouse mammary tumour virus (MMTV), also called Bittner milk factor, transmitted from the infected mother mice to the breastfed daughter mice, prompted researchers to look for a similar agent in human breast cancer.
Though no such agent has yet been identified, there are reports of the presence of reverse transcriptase in breast cancer cells.
Etiology And Pathogenesis:
Overall, two major etiologic factors in the pathogenesis of breast cancer are: hormonal and genetic.
1. Hormonal Factors: Breast cancer is a hormone-dependent disease. There is sufficient evidence to suggest that excess endogenous oestrogen or exogenously administered oestrogen for a prolonged duration is an important factor in the development of breast cancer. Evidence in support of the relationship between increased risk with oestrogen excess is as follows:
- Women with prolonged reproductive life, with menarche setting in at an early age and menopause relatively late, have a greater risk.
- Higher risk in unmarried and nulliparous women than in married and multiparous women.
- Women with first childbirth at a late age (over 30 years) are at greater risk.
- Lactation and breastfeeding reduce the risk of breast cancer.
- Bilateral oophorectomy reduces the risk of the development of breast cancer.
- Functioning ovarian tumours (granulosa cell tumour) which elaborate oestrogen is associated with an increased incidence of breast cancer.
- Hormone replacement therapy (HRT) administered to postmenopausal women may result in an increased risk of breast cancer.
- Long-term use of oral contraceptives containing balanced oestrogen-progesterone preparations do not pose an increased risk.
- Men who have been treated with oestrogen for prostatic cancer have an increased risk of developing cancer of the male breast.
Normal breast epithelium possesses oestrogen and progesterone receptors. Breast cancer cells secrete many growth factors which are oestrogen-dependent. In this way, the interplay of high circulating levels of oestrogen, oestrogen receptors and growth factors bring about the progression of breast cancer.
2. Genetic Factors: About 10% of breast cancers have been found to have inherited mutations. These mutations include the following, the most important of which is the breast cancer (Brca) susceptibility gene in inherited breast cancer:
- Barca 1 gene located on chromosome 17, a DNA repair gene, is implicated in both breast and ovarian cancer in inherited cases. BRCA1 deletion is seen in about two-thirds of women with inherited breast cancer having family history but BRCA1 mutation is uncommon in sporadic cases.
- The protein product of the Brca gene is a cell cycle-regulated protein and it can be detected by immunohistochemistry. Men who have mutated Brca1 have an increased risk of developing cancer of the prostate but not of the male breast.
- Barca 2 gene located on chromosome 13, another DNA repair gene, in its mutated form, has a similarly higher incidence of inherited cancer of the breast (one-third cases) and ovary in females, and prostate in men.
- In BRCA1 as well as BRCA2, both copies of the genes (homozygous state) must be inactivated for the development of breast cancer.
- Mutation in the p53 tumour suppressor gene on chromosome 17 as an acquired defect accounts for 40% of cases of sporadic breast cancer in women but rarely in women with a family history of breast cancer.
- p53 mutation is also seen in Li-Fraumeni syndrome having multiple cancers including breast cancer in young women; others are tumours of the brain, sarcomas, and adrenal cortical tumours.
- A variant form of Li-Fraumeni syndrome having CHEK2 mutation also accounts for some cases of inherited breast cancer.
- Other mutations seen less frequently in breast cancer include a mutated form of the ataxia telangiectasia (AT) gene, and the Pten (phosphate and tensin) tumour suppressor gene.
Classification:
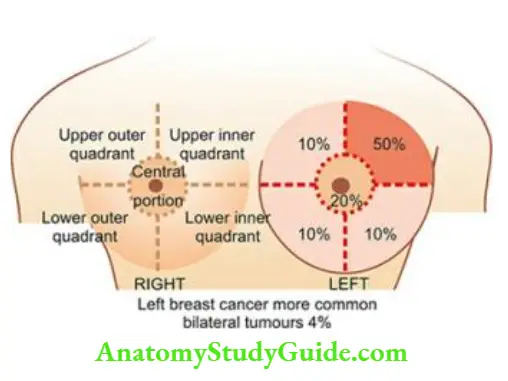
- Cancer of the breast occurs more often in the left breast than the right and is bilateral in about 4% of cases. Anatomically, the upper outer quadrant is the site of a tumour in half the breast cancers; followed in frequency by the central portion, and equally in the remaining both lower and the upper inner quadrants as shown.
- Carcinoma of the breast arises from terminal duct lobular units (TDLU) in 90% of cases while
the remaining 10% originate from the lobular epithelium. For variable periods of time, the tumour
cells remain confined within the ducts or lobules (non-invasive carcinoma) before they invade
the breast stroma (invasive carcinoma). - While only 2 types of non-invasive carcinoma have been described ductal carcinoma in situ (Dcis) and lobular carcinoma in situ (Lcis), there are several morphologic varieties of histological patterns of invasive carcinoma breast which have clinical correlations and prognostic implications.
- presents different morphologic types of carcinoma of the breast as proposed in the WHO classification. Important and common morphological forms are described below.
In Situ (Non-Invasive) Carcinoma:
In general, two types of non-invasive or in situ carcinoma ductal carcinoma in situ (or intraductal carcinoma) and lobular carcinoma in situ, are characterised histologically by the presence of tumour cells within the ducts or lobules respectively without evidence of invasion.
Ductal Carcinoma In Situ (DCIS):
- DCIS or intraductal carcinoma is confined within mammary TDLU. The tumour initially begins with atypical hyperplasia of ductal epithelium followed by filling of the duct with tumour cells.
- Clinically, it produces a palpable mass in 30-75% of cases and the presence of nipple discharge in about 30% of patients.
- Approximately a quarter of patients with intraductal carcinoma treated with excisional biopsy alone develop ipsilateral invasive carcinoma during a follow-up period of 10 years while the chance of contralateral breast cancer developing in patients with intraductal carcinoma is far less than that associated with in situ lobular carcinoma.
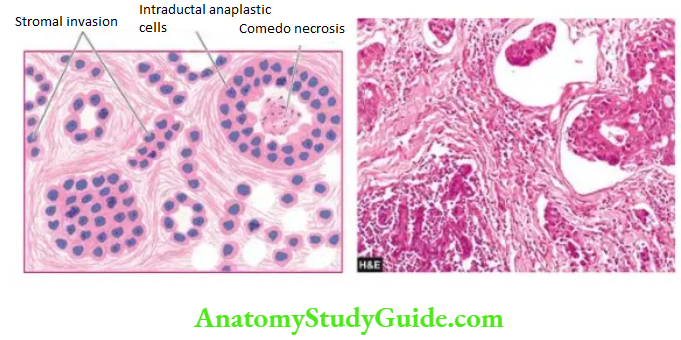
Morphologic Features Grossly, the tumour may vary from a small poorly-defined focus to a 3-5 cm diameter mass. On the cut section, the involved area shows cystically dilated ducts containing cheesy necrotic material (in comedo pattern), or the intraductal tumour may be polypoid and friable resembling intraductal papilloma (in the papillary pattern).
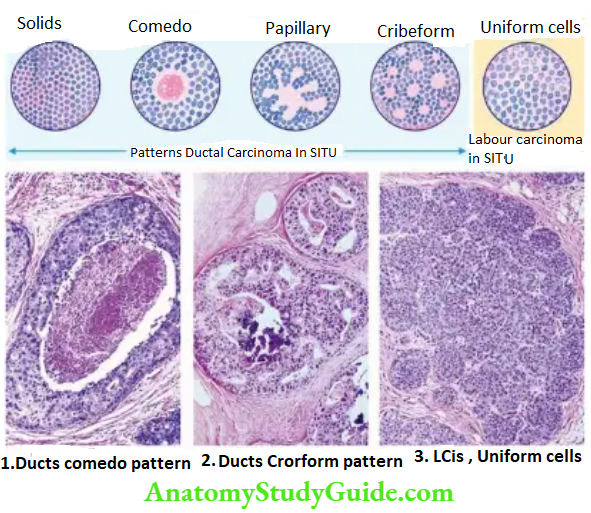
Histologically, the proliferating tumour cells within the ductal lumina may have 4 types of patterns in different combinations: solid, comedo, papillary and cribriform:
- Solid pattern is characterised by filling and plugging of the ductal lumina with tumour cells.
- Comedo pattern is centrally placed necrotic debris surrounded by neoplastic cells in the duct.
- The papillary pattern has the formation of intraductal papillary projections of tumour cells which lack a fibrovascular stalk so as to distinguish it from intraductal papilloma.
- The cribriform pattern is recognised by neat punched-out fenestrations in the intraductal tumour.
Based on nuclear grading, DCIS is classified into low, intermediate and high nuclear-grade lesions.
Lobular Carcinoma In Situ (Lcis):
Lobular carcinoma in situ is not a palpable or grossly visible tumour. Patients of in situ lobular carcinoma treated with excisional biopsy alone develop invasive cancer of the ipsilateral breast in about 25% of cases in 10 years as in intraductal carcinoma but, in addition, has a much higher incidence of developing contralateral breast cancer (30%).
Morphologic Features Grossly, no visible tumour is identified.
Histologically, in situ, lobular carcinoma is characterised by the filling up of terminal ducts and ductules or acini by rather uniform cells which are loosely cohesive and have small, rounded nuclei with indistinct cytoplasmic margins. These are usually multicentric and involve bilateral breasts.
Invasive (Infiltrating) Breast Carcinoma
Invasive Carcinoma Of No Special Type-Nst (Infiltrating Duct Carcinoma-Nos):
Invasive carcinoma of no special type (Nst) is the new nomenclature for the commonly used former infiltrating duct carcinoma-NOS (not otherwise specified) because the earlier term for a common form of breast cancer conveyed as if the tumour arises from ‘ducts’ while it actually arises in the Tdlu.
- Invasive carcinoma of NST is the classic breast cancer and is the most common histologic pattern accounting for 80% of cases of breast cancer. In fact, this is the pattern of cancer for which the terms ‘cancer’ and ‘carcinoma’ were first coined by Hippocrates.
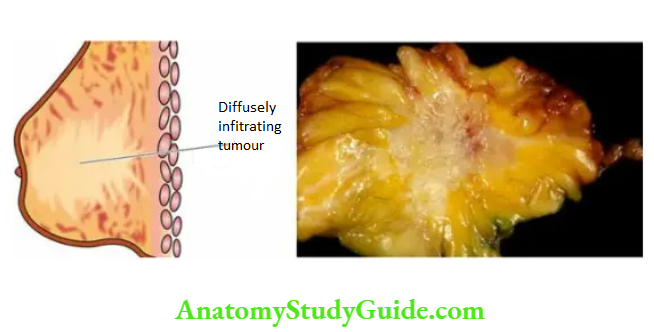
- Clinically, the majority of infiltrating duct carcinomas have a hard consistency due to dense collagenous stroma (scirrhous carcinoma).
- They are found more frequently in the left breast, often in the upper outer quadrant. Retraction of the nipple and attachment of the tumour to the underlying chest wall may be present.
Morphologic Features Grossly, the tumour is irregular, 1-5 cm in diameter, hard cartilage-like mass that cuts with a grating sound. The sectioned surface of the tumour is grey-white to yellowish with chalky streaks and often extends irregularly into the surrounding fat.
Histologically, as the name NST or NOS suggests, the tumour is different from other special types in lacking a regular and uniform pattern throughout the lesion. A variety of histologic features commonly present are as under:
- Anaplastic tumour cells form solid nests, cords, poorly-formed glandular structures and some intraductal foci.
- Infiltration by these patterns of tumour cells into diffuse fibrous stroma and fat.
- Invasion into perivascular and perineural spaces as well as lymphatic and vascular invasion.
Invasive (Infiltrating) Lobular Carcinoma:
Invasive lobular carcinoma comprises about 10% of all breast cancers. This peculiar morphologic form differs from other invasive cancers in being more frequently bilateral; and within the same breast, it may have a multicentric origin.
Morphologic Features Grossly, the appearance varies from a well-defined scirrhous mass to a poorly-defined area of induration that may remain undetected by inspection as well as on palpation.
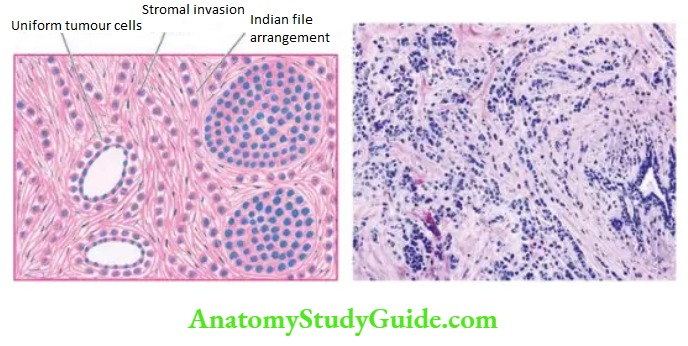
Histologically, there are 2 distinct features:
- Pattern A characteristic single file (Indian file) linear arrangement of stromal infiltration by the tumour cells with very little tendency to gland formation is seen. Infiltrating cells may be arranged concentrically around ducts in a target-like pattern.
- Tumour cytology Individual tumour cells resemble cells of in situ lobular carcinoma. They are round and regular with very little pleomorphism and infrequent mitoses. Some tumours may show signet-ring cells distended with cytoplasmic mucin.
Tubular Carcinoma:
Tubular carcinoma comprises about 6% of cases of invasive ductal carcinoma and has a more favourable prognosis. These tumours are generally small (~1 cm diameter), ill-defined and gritty nodules.
Histologically, the tumour is highly well-differentiated having the following characteristics:
- Pattern The tumour is almost exclusively composed of tubules having angulated shape.
- Tumour cells The tumour cells are regular and form a single layer in well-defined tubules.
- Stroma Tubules are quite evenly distributed in a dense fibrous stroma.
It may be mentioned here that the presence of tubules in other histologic types of breast cancer assigns them a better prognosis (see under grading). Another rare variant forming a cribriform pattern may be seen in tubular carcinoma and has a similar better prognosis.
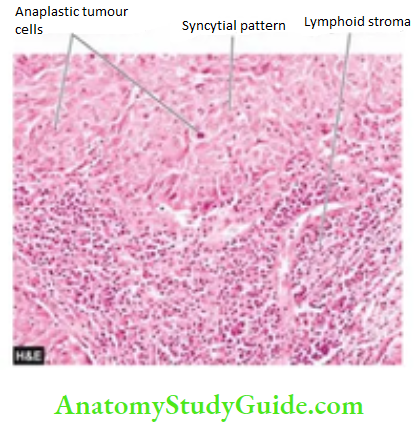
Medullary Carcinoma:
Medullary carcinoma is a variant of ductal carcinoma and comprises about 2% of all breast cancers. The tumour has a significantly better prognosis than the usual infiltrating duct carcinoma, probably due to a good host immune response in the form of lymphoid infiltrate in the tumour stroma.
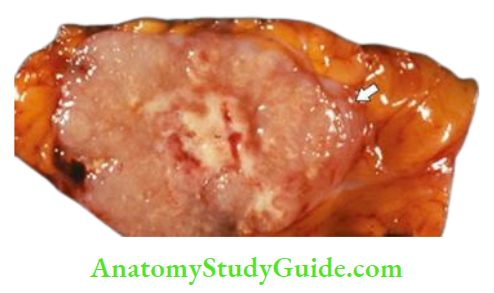
Grossly, the tumour is characterised by a large, well-circumscribed, rounded mass that is typically soft and fleshy or brain-like and hence the alternative name of ‘encephaloid carcinoma’. The cut section shows areas of haemorrhage and necrosis.
Histologically, medullary carcinoma is characterised by 2 distinct features:
Tumour cells Sheets of large, pleomorphic tumour cells with abundant cytoplasm, large vesicular nuclei and many bizarre and atypical mitoses are diffusely spread in the scanty stroma.
Stroma The loose connective tissue stroma is scanty and usually has a prominent lymphoid component as aggregates and infiltrates.
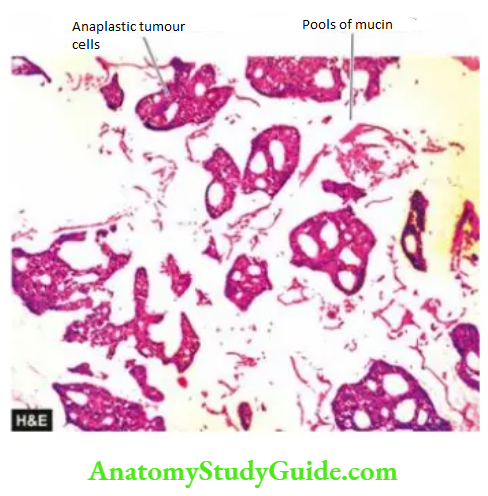
Mucinous Carcinoma:
Mucinous or colloid carcinoma of breast cancer is seen in about 2% of cases, occurs more frequently in older women and is slow-growing. Colloid carcinoma has a better prognosis than the usual infiltrating duct carcinoma.
Grossly, the tumour is usually a soft and gelatinous mass with well-demarcated borders.
Histologically, colloid carcinoma contains a large amount of extracellular epithelial mucin and acini filled with mucin. Cuboidal to tall columnar tumour cells, some showing mucus vacuoles, are seen floating in large lakes of mucin.
Cribriform Carcinoma:
Cribriform carcinoma is an uncommon invasive breast cancer in which the dominant pattern is cribriform i.e. fenestrations in the solid areas of malignant cells that produce a Swiss-cheese pattern. It may exist in pure form but more commonly is present in one of the other histologic patterns.
Other Morphologic Types
A few other uncommon morphologic forms of invasive breast carcinoma having clinical significance have been recognised:
- Papillary carcinoma: It is a rare variety of infiltrating duct carcinoma in which the stromal
invasion is in the form of papillary structures. - Adenoid cystic carcinoma: Adenoid cystic or invasive cribriform carcinoma is a unique histologic pattern of breast cancer in which there is stromal invasion by islands of cells having characteristic cribriform (fenestrated) appearance. The tumour has an excellent prognosis.
- Secretory (Juvenile) carcinoma: This pattern is found more frequently in children and young girls and has a better prognosis. The tumour is generally circumscribed which on histologic examination shows abundant intra- and extracellular PAS-positive clear spaces due to the secretory activity of tumour cells.
- Inflammatory carcinoma: of the breast is a clinical entity and does not constitute a histological type. The term has been used for breast cancers in which there is redness, oedema, tenderness and rapid enlargement.
- Inflammatory carcinoma is associated with extensive invasion of dermal lymphatics and has a dismal prognosis.
- Metaplastic carcinoma: Rarely, invasive ductal carcinomas, besides epithelial elements, may have various components of metaplastic alterations such as squamous metaplasia, cartilaginous and osseous metaplasia, or their combinations.
- The term metaplastic carcinoma includes various categories such as carcinosarcoma, spindle cell carcinoma, carcinoma with osteoclast-like giant cells and squamous cell carcinoma.
- Carcinoma with neuroendocrine differentiation: Low-grade carcinoma with neuroendocrine features in at least 50% of cells is given this nomenclature, while high-grade tumours of neuroendocrine differentiation are called small cell carcinomas.
Paget’S Disease Of The Nipple
Paget’s disease of the nipple is an eczematoid lesion of the nipple, often associated with invasive or non-invasive ductal carcinoma of the underlying breast. The nipple bears a crusted, scaly and eczematoid lesion with a palpable subareolar mass in about half the cases.
- Most of the patients with palpable mass are found to have infiltrating duct carcinoma, while those with no palpable breast lump are usually subsequently found to have ductal carcinoma in situ.
- The prognosis of patients with ductal carcinoma having Paget’s disease is less favourable than of those who have ductal carcinoma without Paget’s disease.
The pathogenesis of Paget’s disease of the breast is explained by the following 2 hypotheses:
- The tumour cells from the underlying ductal carcinoma have migrated up into the lactiferous ducts and invaded the epidermis producing skin lesions.
- An alternate theory, though less reliable than the former, is that Paget’s disease represents a form of carcinoma in situ of the epidermis itself.

Morphologic Features Grossly, the skin of the nipple and areola is crusted, fissured and ulcerated with oozing of serosanguineous fluid from the erosions.
Histologically, the skin lesion is characterised by the presence of Paget’s cells singly or in small clusters in the epidermis. These cells are larger than the epidermal cells, spherical, having hyperchromatic nuclei with a cytoplasmic halo that stains positively with mucicarmine.
In these respects, Paget’s cells are adenocarcinoma-type cells. In addition, the underlying breast contains invasive or non-invasive duct carcinoma which shows no obvious direct invasion of the skin of the nipple.
Grading, Staging And Prognosis
Pathologic Grading:
The following pathologic parameters are used for the management and determination of the clinical course of the disease:
- The histologic type of tumour: Based on the classification described, various microscopic types of breast cancer can be subdivided into 3 histologic grades:
- Non-metastasising—Intraductal and lobular carcinoma in situ.
- Less commonly metastasising—Medullary, colloid, papillary, tubular, cribriform, adenoid cystic (invasive cribriform), and secretory (juvenile) carcinomas.
- Commonly metastasising—Infiltrating duct, invasive lobular, and inflammatory carcinomas.
- Microscopic grade: Widely used system for microscopic grading of breast carcinoma is the Nottingham modification of the Bloom-Richardson system. It is based on 3 features:
- tubule formation;
- nuclear pleomorphism; and
- mitotic count.
- Tumour size: There is generally an inverse relationship between the diameter of primary breast cancer at the time of mastectomy and long-term survival.
- Axillary lymph node metastasis: Survival rate is based on the number and level of lymph nodes involved in metastasis. The more the number of regional lymph nodes involved, the worse the survival rate. Involvement of the lymph nodes from proximal to distal axilla (level 1 superficial axilla, to level 3 deep axilla) is directly correlated with the survival rate.
- In this regard, identification and dissection of the sentinel lymph node followed by its histopathologic examination have attained immense prognostic value (The sentinel lymph node is the first node in the vicinity to receive drainage from primary cancer it stands ‘sentinel’ over the tumour).
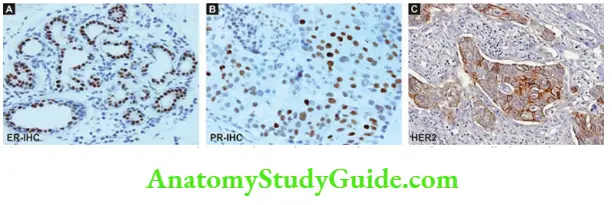
- Oestrogen and progesterone receptors (ER/PR): Oestrogen is known to promote breast cancer. The presence or absence of hormone receptors on the tumour cells can help in predicting the response of breast cancer to endocrine therapy.
- Accordingly, patients with high levels of ER and PR on breast tumour cells have a slightly better prognosis. A recurrent tumour that is receptor-positive is more likely to respond to anti-oestrogen therapy than one that is receptor-negative.
- Her2/neu overexpression: Her2/neu (also called erbB2), a member of the family of epidermal growth factors, is a transmembrane protein having tyrosine kinase activity. It can be detected by immunohistochemistry or by fluorescence in situ hybridisation (Fish) And Is Considered As A Good Predictive Marker.
- An Individual Having overexpression of Her2/neu by tumour cells is likely to respond to a higher dose of Herceptin therapy but is not related to other forms of chemotherapy.
- DNA content: Tumour cell subpopulations with aneuploid Dna content as evaluated by mitotic markers (example Ki-67) or by flow cytometry have a worse prognosis than purely diploid tumours.
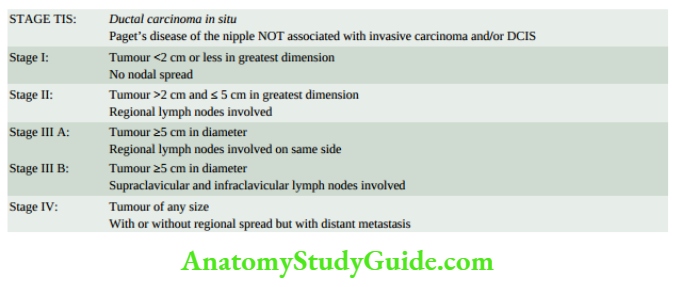
Clinical Staging:
The American Joint Committee on Cancer (AJCC) staging has modified the TNM (primary tumour, nodal, and distant metastasis) staging proposed by UICC (Union International for Control of Cancer) and is shown.
- The spread of breast cancer to axillary lymph nodes occurs early. Later, however, distant spread by lymphatic route to internal mammary lymphatics, mediastinal lymph nodes, supraclavicular lymph nodes, pleural lymph nodes and pleural lymphatics may occur.
- Common sites for haematogenous metastatic spread from breast cancer are the lungs, liver, bones, adrenals, brain and ovaries. Breast is one of the most suspected sources of inapparent primary carcinoma in women presenting with metastatic carcinoma.
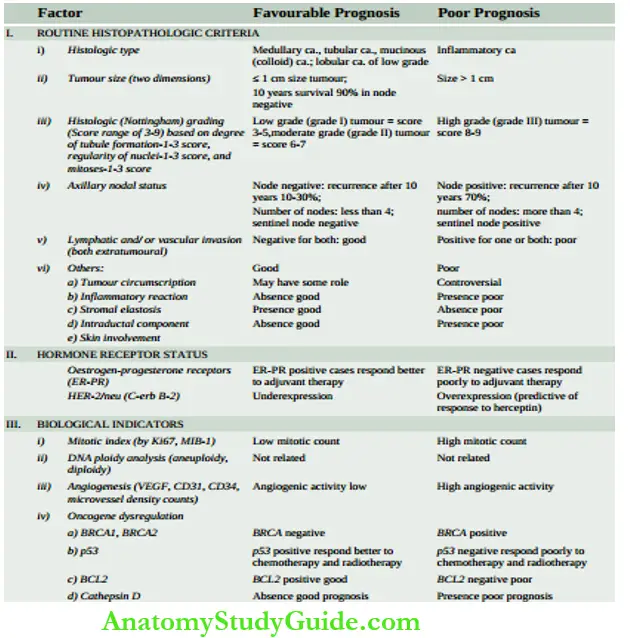
Prognostic Factors In Breast Cancer:
Based on current knowledge gained by breast cancer screening programmes in the West employing mammography and stereotactic biopsy, various breast cancer risk factors and prognostic factors have been described. These prognostic factors are divided into the following 3 groups:
Potentially pre-malignant lesions: These conditions are as under:
- Atypical ductal hyperplasia is associated with a 4-5 times increased risk than women of the same age. Such lesions are commonest in the age group of 45-55 years.
- Clinging carcinoma is a related lesion in the duct but different from carcinoma in situ and has a lower risk of progression to invasive cancer than in situ carcinoma.
- Fibroadenoma is a long-term risk factor (after over 20 years) for invasive breast cancer, the risk being about twice compared to controls.
2. Breast carcinoma in situ: Following factors act as determinants:
- Ductal carcinoma in situ (comedo and non-comedo subtypes) is diagnosed on the basis of three histologic features nuclear grade, nuclear morphology and necrosis, while lobular neoplasia includes the full spectrum of changes of lobular carcinoma in situ and atypical lobular hyperplasia.
- Ductal carcinoma in situ is more important and demands the most attention. Comedo type of in situ carcinoma has a higher recurrence rate.
- Breast conservative therapy is used more frequently nowadays in carcinoma in situ which requires consideration of three factors for management: margins, extent of disease, and biological markers.
- The biological markers such as p53 and BCL-2 have low positivity in high-grade in situ ductal carcinoma and there is a likelihood of recurrences after conservative surgery.
3. Invasive breast cancer: Prognostic and predictive factors for invasive breast cancer have been extensively studied by univariate analysis (examining a single factor separately) as well as by multivariate analysis (comparing the value of various factors included in a study). These can be broadly divided into 3 groups:
- Routine histopathology criteria,
- Hormone receptor status, and
- Biological indicators.
A summary combining all these factors is given. Overall, taking the most important parameter of node-positive or node-negative breast cancer, the prognosis varies a localised form of breast cancer without axillary lymph node involvement has a survival rate of 84% while the survival rate falls to 56% with nodal metastases.
4. Molecular classification: More recently, based on gene profiling of breast cancer by microarray, a molecular classification has been proposed.
- It takes into consideration patterns of gene expression by breast cancer which may be one of the four types luminal type A or B, HER2/neu type, basal-like type, and normal breast-like type.
- Out of all these, the basal-like type has the worst prognosis while luminal type A responds well to endocrine therapy and has a good prognosis. However, this classification is yet to get universal acceptance.
Carcinoma in Situ and Invasive Breast Cancer:
- Cancer of the breast is common and many risk factors have been identified: geographic and racial variation, family history, menstrual and obstetrical history, oestrogen excess and heredity.
- Initially, the tumour cells remain confined within the TDLU or lobules (non-invasive or in situ carcinoma) which may be ductal carcinoma in situ (Dcis) and lobular carcinoma in situ (Lcis).
- The most common invasive breast cancer is invasive carcinoma of no special type-NST (earlier called infiltrating duct carcinoma-not otherwise specified-NOS); others are lobular, medullary, colloid, cribriform, tubular and some less common types.
- Histologic grading and clinical staging of breast cancer determine the management and clinical course of breast cancer.
- A few salient factors for favourable prognosis are tumour size < 1 cm, histologic types (medullary, tubular, colloid, cribriform), grade I tumour, node-negative, ER-PR positive, and Her2/neu underexpressed.
Leave a Reply