Pediatrics History Taking Notes
History taking is an art and demands the skills of a lawyer, detective, and judge. It demands inquisitiveness, persistence, and tact.
Table of Contents
The physician should strive to obtain a lucid chronological story of the child’s illness with special emphasis on the mode of onset and course of events.
Pediatrics has been likened to veterinary medicine because young children cannot express their symptoms. The symptomatology in young children is often “colored” by the perceptions of “keepers”, the parents.
Read and Learn More Pediatric Clinical Methods Notes
An intelligent and observant mother can provide a satisfactory story of illness but at times may exaggerate facts due to her anxiety and concern.
Father spends little time with the child and is generally ill-informed about the child’s problems. Schoolgoing children can give a fair account of their physical difficulties and should always be encouraged to talk and explain their symptoms.
The physician must exhibit humility, concern, and politeness while recording history. He should be gentle, sympathetic, gracious, and kind in his approach but alert and attentive.
During history taking, provide positive non-verbal cues to enhance doctor-patient/parent communication.
You should lean forward, listen attentively with interest, maintain eye contact, nod appropriately, do not cross your arms or exhibit any sense of superiority or arrogance.
The clinician should maintain a friendly, warm, relaxed, unhurried, and informal atmosphere throughout the interaction with the family.
Always keep your mind open and receptive—even an experienced physician can learn something new from his patients and their attendants.
There is a popular saying, that a “smart mother or grandmother can make a better diagnosis than a dull doctor.”
The physician must remember that the patient is his honored client and he should relieve the anxiety of the parents and instill confidence in them towards himself during the interview.
However, he should not behave like an enthusiastic salesman by dramatizing the illness of the child.
It is often forgotten that while you are taking history and assessing the attendant and child, you are also being assessed by them on the basis of your behavior and approach.
Your facial expression, tone of voice, body language, and attitude of impatience, arrogance, disbelief, and reproach can all affect the outcome of communication between the doctor and patient/parents.
History-taking is the beginning of the most crucial doctor-patient (parent) relationship, which is essential for developing mutual trust and confidence.
The doctor must know his or her own personality, recognize weaknesses and develop strengths and abilities to improve his or her communication skills.
Assess the quality of the parent-child and parent-parent relationship while recording history and conducting a physical examination.
Unsatisfactory parent-child or motherfather interaction may lead to emotional deprivation or psycho-social and behavioral disorder in the child.
The consultation room should be well-lighted, comfortable, quiet, and decorated with toys and pictures to allay the anxiety of the child.
There should be no distractions or disturbing sounds, the mobiles should be kept on silent mode. Infants and young children should be offered a soft squeaky toy or a rattle to establish rapport while taking history.
Schoolgoing children feel at ease when they are directly asked their names, and details about school, hobbies, and health problems. While taking history, the child should be observed “sneakily” for facial appearance, discomfort, distress, and dyspnea.
Avoid staring at the child because children are often scared if you intently look into their eyes. Watch him without being watched by the child.
The child must visualize the physician as the friend of the mother and not a frightening figure who prescribes painful pricks and pungent potions.
The cordial atmosphere is crucial while recording history. The pediatrician is watching the child sneakily while
the child is “evaluating” the pediatrician with ease, confidence, and trust. In this situation, the child is likely to cooperate during the examination.
It must be remembered that most common diseases can be diagnosed by good history alone. Elicitation of history should continue during physical examination to seek additional information especially when unexpected abnormal physical findings are detected.
History and physical examination should be viewed in a continuum and one should influence the other.
The leads obtained on history should focus the physical examination on certain organs while the presence of positive physical findings should encourage the pediatrician to seek a more detailed review of certain symptoms pertaining to the involved system.
To gain the confidence of parents and children, the pediatrician should maintain a friendly, warm, unhurried, courteous, informal, and relaxed attitude throughout the assessment.
You must put the parent or attendant at ease and encourage him or her to talk freely. Never judge or belittle the mother, instead encourage and support her.
You should provide positive non-verbal cues to the family. Your behavior should not be influenced by the social status of the parents.
Instead, you must visualize God in every human being and feel honored that you have been given the responsibility to serve Him.
Basic Information
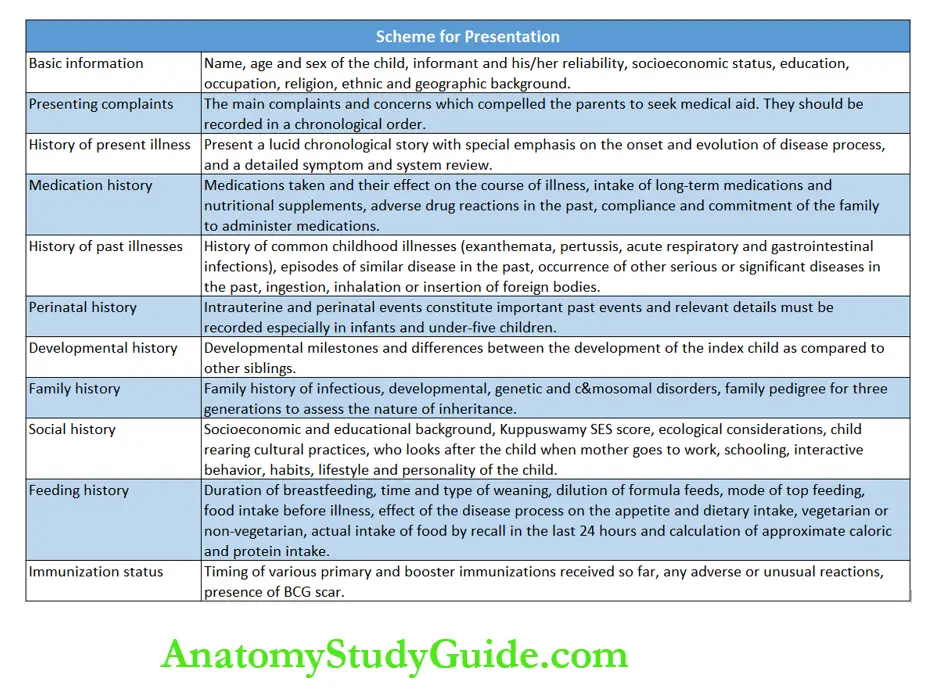
The salient components of history taking are summarized in. Informant (mother, father, relative, child, etc.), name, age (preferably date of birth), and sex of the patient should be enquired.
The parent’s name, age, address, telephone number, income, occupation, education, and religion should be recorded. The history may be unreliable due to the informant’s poor memory, intelligence, or education.
The origin and ethnic background of the family are important in some genetic diseases. Thalassemia traits and disease are common among migrants from West Pakistan.
Glucose-6 phosphate dehydrogenase deficiency is common among Parsis and North Indians while sickle cell disease is seen among tribal populations.
Key points for taking history
- Personal and demographic details
- Presenting complaints
- History of present illness
- Symptom review
- System review
- Medications received
- Past history
- Perinatal events
- Significant illnesses and accidents
- Physical growth and developmental milestones
- Family history
- Genetic diagram
- Social history and lifestyle
- Feeding history
- Immunization status
Presenting Complaints
The chief complaints for which the patient has been brought to the hospital should be recorded in chronological order according to the sequence of events. fever 5 days, headache 3 days, vomiting 3 days, convulsions 1 day, and loss of consciousness 12 hours.
The key symptoms obtained from history should initiate a cascade of logical reasoning, based on the experience and knowledge of the physician to consider plausible diagnostic possibilities or hypotheses for further probing.
History Of Present Illness
The mother should be encouraged to give details of the sequence of events during the illness without the help of leading questions.
You must put the parent or attendant at ease and encourage him or her to talk freely. The mode of onset, course of disease, and details of treatment already received must be recorded in all cases.
The parents are very keen to tell you what the previous doctor(s) thought about the child’s illness and often use terms like rheumatism, weak liver, acidity, tonsils, and migraine.
You should not brush them aside but assure them that you shall see all the documents and reports but “let me first understand or grasp the problem”.
A piece of detailed information about various symptoms manifested by the patient should be elicited symptom review). The symptoms are referable to various body systems and should be reviewed to identify the site of the disease (system review).
The history should provide information on whether the disease is localized to a particular body system or is generalized by involving several systems.
The purpose of a detailed review of symptoms is to identify the anatomical site(s) and etiology of the disease process. The clinical characteristics and morphology of common symptoms are given below.
Cry
The cry is the “language” of the child and an important signal of discomfort, boredom, or hunger. The intelligent mother can differentiate between the cry of a well-baby (hunger, wet napkin, boredom) from that of a sick baby.
Infants with painful conditions, like intestinal colic, acute otitis media, inflammatory or traumatic conditions of bones and joints, and torsion of the testis.
are likely to have incessant inconsolable crying and cannot be pacified by cuddling or feeding. A cry is an important symptom of hypoxia in infants with lower respiratory infections and obstructive airway disease.
A high-pitched shrill cry is a characteristic feature of cerebral irritation and raised intracranial tension (meningitis) and tetanus neon atom.
In some conditions, like arthritis, osteomyelitis, periosteitis, abscess, peritonitis, etc., the crying becomes worse when a child is picked up and the child is relatively comfortable when undisturbed.
A hoarse cry is a feature of “excessive crying”, cretinism, laryngitis, laryngotracheobronchitis, and paralysis of the left recurrent laryngeal nerve due to compression by the dilated main pulmonary trunk.
Crying due to temper tantrums or fussiness in healthy preschool children (6 months – 3 years) may be followed by a breath-holding spell. In a child with tetralogy of Fallot, crying is a feature of the cyanotic spell.
Fever
The normal body temperature is maintained within a narrow range of 98.2°F ± 0.7°F (36.8°C ± 0.4°C).
Fever is defined as an elevation of oral temperature above 100°F (>37.8°C). Hyperpyrexia is diagnosed when the rectal temperature exceeds 107°F (>41.5°C).
Onset (acute or insidious), duration, character (continuous, remittent, intermittent, step-ladder type, Pel-Ebstein, etc.), severity, chills, rigors, associated localizing symptoms, etc.
should be enquired about. PelEbstein relapsing fever is characterized by episodes of fever lasting for 3–10 days followed by afebrile periods of 3–10 days and is a classical feature of Hodgkin disease and other lymphomas.
Young children cannot complain of chills (perception of extreme cold) but rigors may be observed by the mother as goose skin, vigorous shaking movements, or tremors.
When body temperature never touches normal and daily fluctuations are less than 1°C, it is described as continuous fever.
When the daily fluctuations exceed 2°C, it is called a remittent or hectic temperature which is a characteristic feature of septicemia and Kawasaki disease.
Evening rise of fever occurs in most infections but is a characteristic feature of tuberculosis and juvenile rheumatoid arthritis.
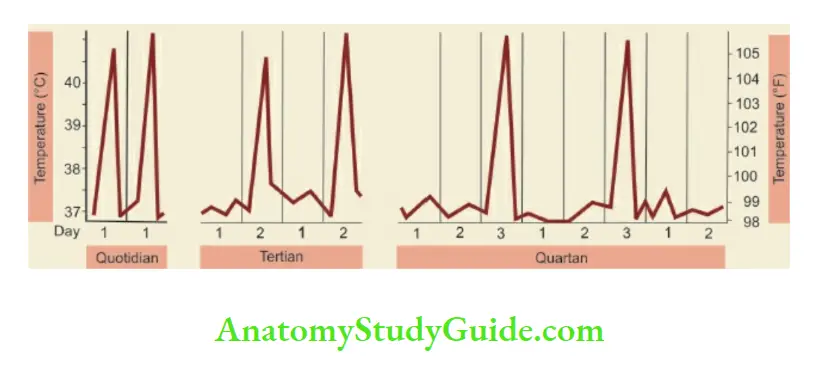
In intermittent pyrexia, the temperature may touch or remain normal daily (quotidian), every alternate day (tertian), or every two days (quartan).
Quotidian fever occurs due to several conditions including juvenile chronic arthritis, tertian fever occurs classically due to Plasmodium vivax malaria, and quartan fever because of Plasmodium malaria.
However, because of the widespread use of antipyretics and antibiotics, the classical pattern of fever is no longer seen.
During therapy, fever may settle down quickly within 6–12 hours with marked sweating (crisis) or slowly over several days (lysis).
Cough
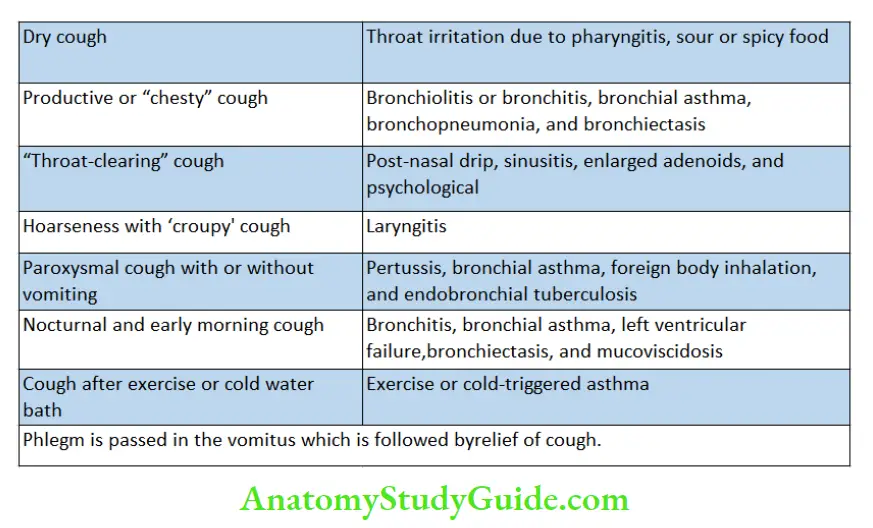
Duration, frequency, character (hacking, brassy, barking, paroxysmal followed by long and deep noisy inspiration, i.e. ‘whoop’), dry or productive, postural relationship, diurnal variations, and associated features should be recorded.
Ask whether the cough is dry or associated with a “chesty” sound. In children with bronchitis, wheezing, and congestive heart failure, cough is worse on lying down and during sleep. Cough is worse at night and early morning in children with bronchial asthma.
Infants do not expectorate but they swallow the phlegm and may vomit it out.
History of inhalation of a foreign body should always be enquired in any child with sudden onset of choking and cough with breathlessness and in children with recurrent or persistent pulmonary suppuration.
Many times clinical morphology of cough provides more useful information than findings on auscultation of the chest. The characteristic nature of various types of cough and the likely underlying causes are listed.
Vomiting
Regurgitation of feeds (possessing) is a common symptom in infants due to aerophagy. Some children are very vulnerable to vomit following a bout of cough or when food is forced or medicine is given.
Ask about the duration, severity, and frequency of vomiting and whether it is associated with nausea or anorexia. The presence of bile or fecal matter is suggestive of intestinal obstruction.
Blood-tinged vomiting (hematemesis) is a medical emergency. Aggravating factors and associated symptoms often provide clues to the diagnosis.
Association with fever, headache, neck rigidity, and alteration in consciousness are suggestive of meningitis, presence of abdominal distension, and absolute constipation with none of the flatus is suspicious of intestinal obstruction and the development of diarrhea is indicative of acute gastroenteritis.
Episodes of vomiting with fever, ketosis, and acidosis are suggestive of diabetic ketoacidosis, cyclical vomiting due to autonomic dysfunction, or visceral epilepsy.
Ask for symptoms of dehydration, such as excessive thirst, absence of sweating or tears, reduced frequency of passing urine, or anuria.
Diarrhea
Passing stools after each feed, due to exaggerated gastrocolic reflex, should not be mistaken for diarrhea. Diarrheal episodes are common in bottle-fed children due to the intake of contaminated or infected feeds.
Ask for a history of duration, severity, and frequency (purge rate) of diarrhea and associated symptoms, like fever, vomiting, and colicky abdominal pain.
Assess the bulk (small or bulky), consistency (watery, rice-water, semi-loose or semisolid), contents (undigested food particles, steatorrhea, froth, mucus, pus, blood), color (yellow, pale, green), and odor (foul-smelling, rancid) of stools.
Dysentery is characterized by the passage of blood and mucus in stools, tenesmus (frequent urge to defecate but with little evacuation), and rectal prolapse.
Ask for symptoms and correlates of dehydration, e.g. inadequate intake of fluids, excessive crying due to thirst, absence of sweat or tears, cold extremities, oliguria, and anuria.
Pain Abdomen
Duration, frequency, timing, site (vague, precise, localized, diffuse), severity (mild, moderate, severe, excruciating), character (burning, piercing, boring, colicky), radiation, precipitating, aggravating, and relieving factors, and associated symptoms should be recorded.
The characteristics of pain can be remembered by the acronym SOCRATES which stands for Site, Onset, Character, Radiation, Associated symptoms, Timing, Exacerbating and relieving factors, and Severity.
The child with recurrent abdominal pain, if puts his whole hand vaguely in an unconcerned manner over the center or whole of the abdomen to indicate the site of pain, is most likely having a functional or psychogenic disorder.
When pain abdomen is associated with pain at multiple body sites, like headache, chest pain, and body aches, it is likely to be functional rather than organic.
Episodes of momentary abdominal pain which occur at home and in relation to the intake of food, are usually due to attention-seeking behavior, or food fussiness.
When pain occurs in school or during play activity or a child wakes up with pain at night, it is likely to be due to organic causes. The common symptoms are referrable to various body systems listed.
It is important to give due credit to all observations of the parents, even if they do not fit into your line of thinking or diagnosis.
Parents often confuse pallor and jaundice, hematemesis and hemoptysis, rigors, and seizures, breath-holding spells and seizures, pus and wax in the ears, etc. and you must try to differentiate between them by asking appropriate leading questions.
Review of systems
General Features
- Breathing
- Fever
- Crying or lethargy
- Loss of appetite
- Pallor
- Lassitude, “off color”,
- fatigue, lack of interest in
- play activity
- Failure to thrive
Gastrointestinal system and abdomen
- Pain abdomen
- Dysphagia
- Vomiting
- Diarrhea or constipation
- Bulky or oily stool
- Dyspepsia
- Anorexia or excessive
- appetite
- Distension or “wind”
- Jaundice
- Anal itching
- Rectal prolapse
- Failure to thrive
Genitourinary system
- Pain abdomen
- Tight prepuce
- Breathing difficulty
- Wheezing
- Cyanosis and clubbing
- Vomiting preceded by cough
- Chest pain
Cardiovascular system
- Tachypnea and dyspnea
- Palpitations
- Feeding difficulties
- Puffiness of face and swelling of feet
- Cough in a supine position
- Cyanosis and clubbing
- Chest pain
Hematologic system
- Lassitude, irritability, fatigue, and exertional dyspnea
- Pica
- Petechiae and blood loss
- Bone pains
- Enlarged glands or swellings in the neck, axillae and
- groins
- Dietary and drug history
Central nervous system
- Crying, irritability, alterations in sleep, behavior and
consciousness - Learning disability
- Syncope
- Vertigo
History Of Medications
The history of current medications and their effect on the course of the disease process should be enquired. Ask whether the child is receiving any long-term medications, or nutritional supplements from any system of medicine.
Ask if the patient is taking any medications from the complementary and alternative systems.
Take note of diagnosis already made or medications being taken but never say a slighting word or talk ill of your practitioner colleague. History of any adverse or allergic reactions to any medications in the past should be asked and recorded.
Enquire if the child is known to be suffering from any genetic disorder (like G-6-PD deficiency or enzymopathy) which increases the risk of adverse reactions to certain medications.
Assess the likely compliance and commitment of the family to administer the medications in a dose, frequency, and duration as recommended by the physician.
History Of Past Illnesses
Ask for past history of common childhood diseases (recurrent upper respiratory infections, asthmatic bronchitis, diarrheal episodes, exanthemata, pertussis) and whether they ran a normal or complicated course.
Details of perinatal history, birth asphyxia, severe neonatal jaundice, and meningitis are important in a child with developmental retardation or seizures.
Delayed cry at birth is associated with seizures having onset within the first 36 hours of life, abnormal neurological behavior, and difficulties in self-feeding are suggestive of significant birth asphyxia.
In children suffering from asthma, epilepsy, nephrotic syndrome, arthritis, eczema, etc., inquiry should be made regarding the history of similar attacks and their frequency in the past.
Specific inquiries should be made regarding previous illnesses which may be related to the present symptoms or illness.
Past history of jaundice in a child with cirrhosis, joint pains in a child who is suspected to have rheumatic heart disease, recurrent chest infections in a patient with a left-to-right shunt so on and so forth.
Perinatal History
It is pertinent to ask about perinatal history when dealing with neonates or infants but may be ignored in older children with normal development.
Maternal diseases or medications during pregnancy (especially during the first trimester), presentation, mode, and place of delivery, first cry after birth, feeding difficulties during the neonatal period, jaundice, seizures, birth weight, and gestation should be recorded.
Developmental History
In children suspected to have delayed development or CNS disorder, a detailed developmental screening should be undertaken.
The precise timing of social smile, head control, rolling over, sitting, standing, walking, self-feeding and dressing, bladder and bowel control, and speech should be enquired about.
It is useful to compare the development of the index child with other normal siblings. It is easier for the mother to recall differences in the development of the index child as compared to other siblings rather than absolute ages for attaining various milestones of development.
Identify whether it is global developmental retardation, or retardation in a specific field, e.g.
delayed speech in the presence of normal motor development is indicative of deaf-mutism, while delayed standing and walking with normal social and adaptive development is indicative of protein energy malnutrition, and congenital dislocation of hips.
A detailed assessment of development is given in Chapter 6.
Family History
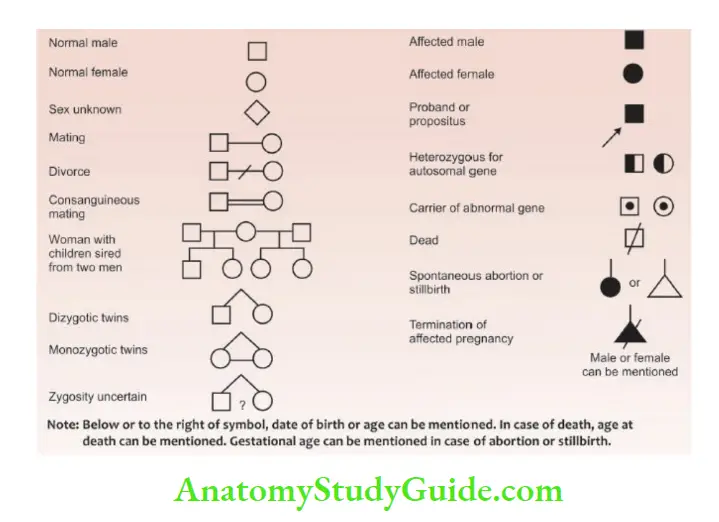
The family pedigree should be enquired and a genetic diagram or family tree of three generations constructed as shown in The details of symbols used for constructing a pedigree chart are shown.
Is the child adopted or biological? In an out-of-family adopted child, it is not possible to ascertain the genetic background.
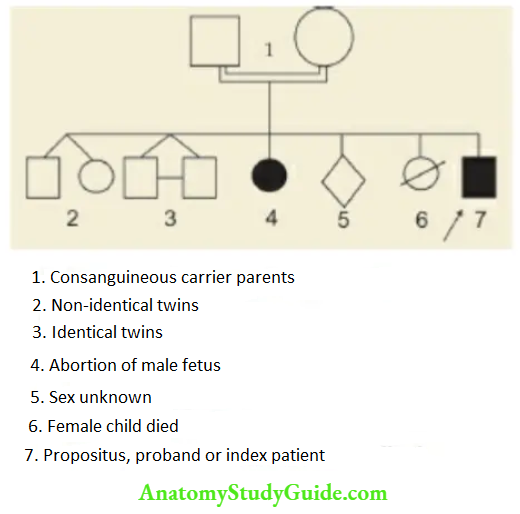
The family pedigree. Ask for information from both the parents and grandparents to identify the nature and mode of inheritance of genetic disorders.
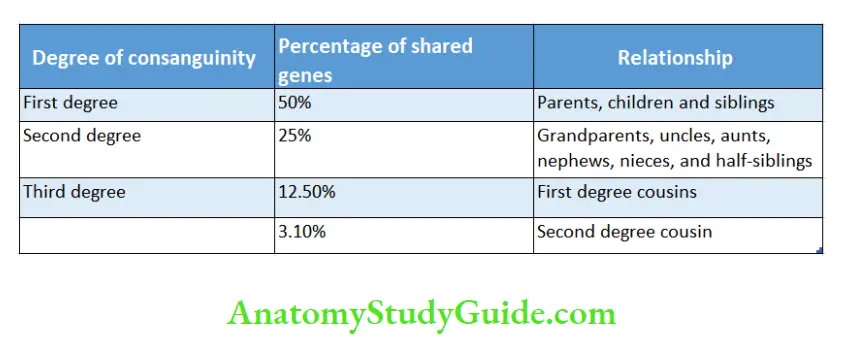
Consanguinity (blood relationship) refers to the kinship of common lineage or ancestry. The offspring of consanguineous parents are at a greater risk of suffering from certain genetic disorders because of the sharing of genes.
The closer the relationship between the parents, the greater the risk of genetic disorders. The most common consanguineous relationship is first cousins, in which the spouses share 1/8 (12.5%) of their genes.
History of contact with possible infectious illnesses should be sought, for example, viral fever, tuberculosis, leprosy, childhood infectious diseases, infective hepatitis, typhoid fever, scabies, and pyoderma.
The index case may be in the family, neighborhood, creche, or school. History of similar ailments in the family members should be asked when the genetic, infectious, or allergic disorder is strongly suspected.
In a child with a fever of acute onset, a history of fever and coryza among family contacts is highly suggestive of viral infection. Ask for a history of consanguinity among parents when a genetic disorder is suspected.
In case a particular disease is manifesting only among male siblings, it is suggestive of X-linked inheritance, for example, hemophilia, pseudohypertrophic muscular dystrophy, G-6-PD deficiency, etc.
Social History
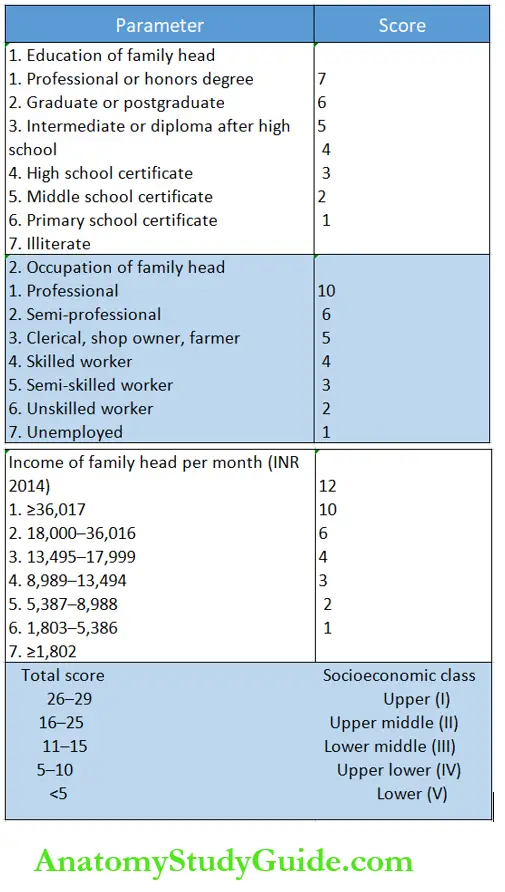
Socioeconomic status (SES) is an important determinant of the health and well-being of the family. The useful determinants of social status include education and occupation of the family head and his monthly income.
A number of scales are available to objectively assess the SES of the family but the Kuppuswamy scale is the most popular.
The steady inflation and resultant devaluation of the Indian rupee and increase in the consumer price index necessitate periodic revisions of the income variable.
Instead of the monthly income of the family head, it is more logical to know the total income or per capita income of the family.
Other variables, which are ignored in most SES scales, include habitat (rural, urban, semi-urban, or slums), type of housing or dwelling conditions, availability of safe drinking water, toilet facilities, and availability of reliable and affordable medical facilities within a reasonable distance.
If the mother is working, ask who looks after the child at home when she is away or if the child is left in a creche. Ask whether the family is nuclear or joint and whether grandparents are staying with the family or not.
Calculate per capita income by dividing the total income of the family by the number of family members. Housing conditions, toilet facilities sewage disposal, and water source should be asked.
Ethnic background and religion may provide clues to certain genetic disorders. Harmful social and cultural practices regarding child-rearing should be identified, for example, dummy nipple or pacifier, complementary bottle feeding, use of kajal, Janam ghatti, etc.
Ask whether the child is attending school or not, what is his rank in the class and whether the disease has interfered with his studies or not.
Assess the interactive behavior, habits, hobbies, interests, lifestyle, and personality of the child and how he differs from other siblings. Ask about the eating, sleeping, and toilet habits of the child.
Adolescent children should be encouraged to talk regarding their worries, anxieties, psychosexual difficulties, and substance abuse tendencies.
Ask whether any pets and animals are kept at home or courtyard. Enquiry should be made regarding smoking, intake of alcohol, or drug abuse by parent(s) which can adversely affect the family dynamics and child-rearing practices.
In an unexplained fever, ask for any history of travel to an endemic area.
Feeding History
The history of dietary intake is of special importance in children because they need food for activity, growth, and development. The energy or caloric requirements of infants per unit body weight are at least 4 times as compared to adults.
Ask whether the child received breastfeeding or not, whether it was exclusive or complemented with bottle feeding, frequency, type of schedule (time or demand), duration, and reasons for discontinuation of breastfeeding.
If top fed, age at start, nature of formula (dried milk or fresh milk), dilution, amount, frequency, and mode of feeding (bottle or cup and spoon or payday), should be enquired in detail.
Age at weaning, nature, and amount of semisolid food or other supplementary foods or vitamins and minerals given to the child should be asked.
Ask whether a family is vegetarian or non-vegetarian. Assess whether the child is having food fussiness and using “blackmailing” tactics because of overindulgence by parents and grandparents.
Is the child taking a balanced diet or having cravings for junk food with a poor intake of green leafy vegetables and fruits? Dietary intake just before the onset of illness and during illness should be enquired.
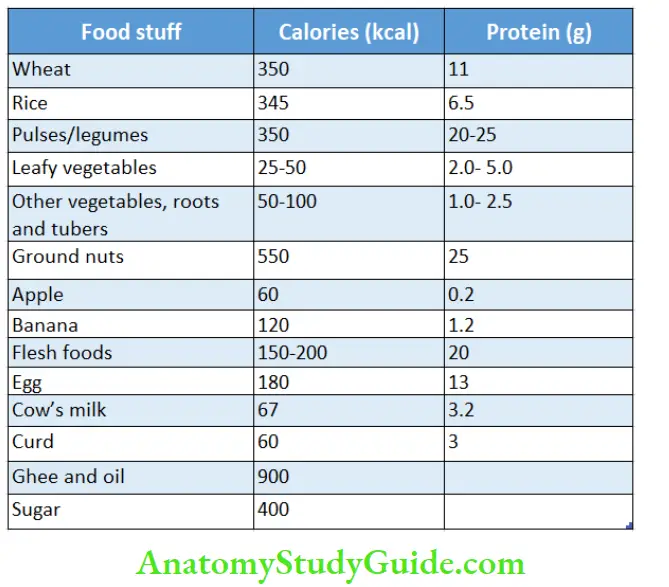
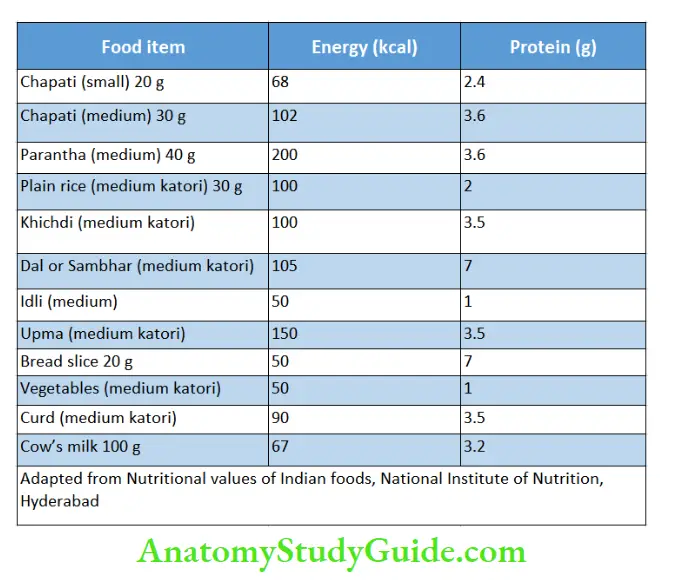
Ask in detail about the actual food intake during the last 24 hours to calculate approximate caloric and protein intake per day.
Adapted from Food and Health, Eds. VR Murthy, BR Rama Shastri, K Srilakshmi. National Institute of Nutrition, Hyderabad, 1979.
A standard hen’s egg weighs 50–60 g and provides 300 mg of cholesterol.
Khichdigruel and cooked pulses contain one part of dry foodstuff and 4 parts of water. Cooked rice contains one part of rice and one part of water.
The common home measures a Teaspoon of 5 ml, a tablespoon of 15 ml, a Katori or cup of 150 ml, and a glass of 250 ml. Average-sized chapati has 30 g wheat flour.
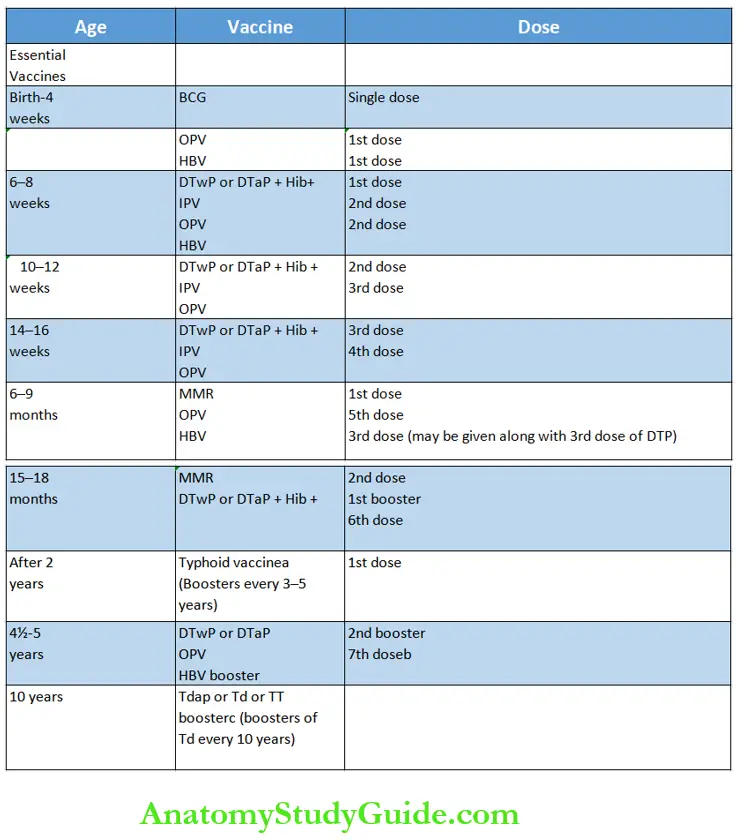
Immunization Status
Ask for various immunizations received so far. This information is useful to guide the diagnosis and ensure comprehensive management of the child. Look for scars of BCG vaccination during physical examination.
All children must be advised on feeding and immunizations whether they are attending OPD or discharged from the hospital. This outlines the current schedule of immunization recommended by the Indian Academy of Pediatrics.
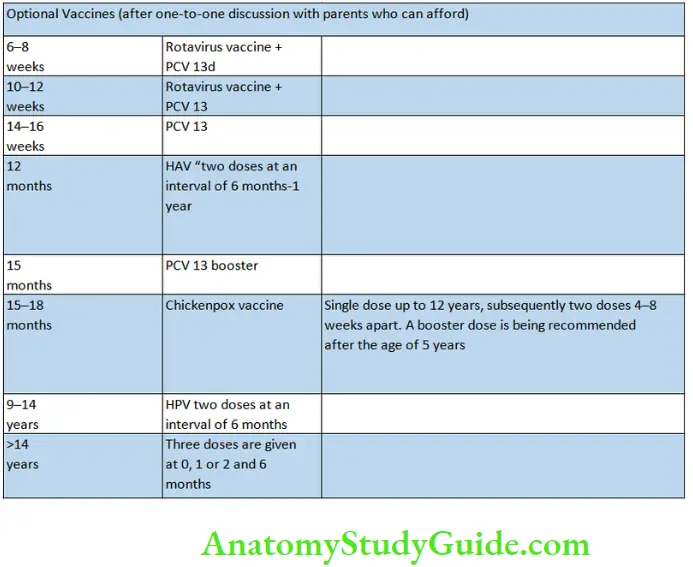
Additional Vaccines During Special Situations
IPV (injectable or inactivated polio vaccine) is given to immunocompromised or HIV-positive children. It is being administered routinely as a part of the post-polio eradication policy.
Meningococcal vaccine (during an epidemic, Haj pilgrims, sickle cell disease, CSF rhinorrhea). Polysaccharide vaccine is given in a single dose after 2 years followed by boosters every 3 years.
Pneumococcal polysaccharide vaccine. PPV 23 (chronic lung and heart disease, splenectomy, nephrotic syndrome, immunocompromised child).
Influenza cum swine flu vaccine (bronchial asthma, immunocompromised child). Initially, 2 doses are given 4 weeks apart in children between 6 months to 9 years, followed by yearly boosters at the onset of winter.
In children above 9 years, a single primary dose is recommended.
Anti-rabies vaccine ‘pre-exposure prophylaxis’ is given to high-risk individuals (children having pets, hostelers, postmen, veterinary doctors, wildlife or dog handlers) in 3 primary doses of 1.0 ml 1M on days 0, 7, and 21 or 28. A booster dose is given after one year and then every 5 years.
In immunized subjects, for post-exposure protection, only two doses are given on days 0 and 3. In these cases, there is no need to administer rabies immune globulins (RIG).
Cholera vaccine (to control epidemics, visitors to Kumbh Mela, and Haj pilgrims).
Japanese B encephalitis vaccine (in endemic areas, and during epidemics) is administered at 0.5 ml at 13 years, 1.0 ml at 3–10 years SC) in 3 primary doses 0, 7, 30 days, boosters at one year followed by boosters every 3 years.
Yellow fever (travelers to South Africa). Avoid pregnant women and infants below 6 months.
aVi capsular polysaccharide S. typhi type 2 conjugated to tetanus toxoid (Typbar TCV) can be given during 9–12 months
followed by a single booster at 2 years of age for lifelong protection.
Additional doses of oral polio vaccine given under the pulse polio immunization program must be taken by all children below the age of 5 years.
CPregnant women must receive 2 doses of TT or Td at 4-week intervals. The second dose should be taken at least 4 weeks before delivery.
dIn older children, single or two primary doses are given.
eLive hepatitis A vaccine (Biovac-A) is given in a single dose.
BCG: Bacillus Calmette-Guerin vaccine for TB, HBV: hepatitis B vaccine, DTP: triple antigen containing vaccines against diphtheria, tetanus, and pertussis (whooping cough), DTwP (whole cell pertussis), DTap (acellular pertussis),
PCV13: 13-valent pneumococcal conjugated vaccine,
PPV 23: 23-valent pneumococcal polysaccharide vaccine.
OPV: oral polio vaccine,
IPV: inactivated polio vaccine,
MMR: measles, mumps, and rubella vaccine, Tdap: tetanus toxoid with low dose diphtheria
and pertussis vaccine,
Td: dual vaccine with small dose diphtheria vaccine (5 Lf or 2 i.u.) which can be safely given to adults,
TT: tetanus toxoid,
Hib: Haemophilus influenza type b,
HAV: hepatitis A vaccine
Modern Trends In History Recording
1. Problem-Oriented Chart
It incorporates baseline conventional data plus a system review with a detailed list of problems, a plan of management for each problem, auditing, and computerization of data.
It is undergoing modifications and its biggest disadvantage is that it leads to depersonalization.
The acronym SOAP is used to document problem-oriented medical records where S stands for subjective, O for objective, A for assessment or differential diagnosis, and P for a plan of action.
Example: Rahul 2 years old boy from Ballabgarh township presented with
SOAP
S
- History of high grade, continuous fever of one-week duration.
- Semi-loose stools without any blood and mucus with a purge rate of 5–6 stools/day, and were treated with concentrated ORS and injectable antibiotics. Urine output was adequate.
- Vomitings for 2 days with a frequency of 5–6 times/day.
- One episode of generalized tonic-clonic seizures 12 hours ago.
- Altered sensorium for 12 hours.
O
Toxic sick semi-comatose child with stable vital signs. Rectal temperature 40°C. No evidence of dehydration or meningeal irritation.
The liver is 3 cm and the spleen is just palpable. Deep tendon jerks were exaggerated with bilateral extensor plantar but no focal neurological signs. Fundus examination was normal.
A
- Enteric fever with encephalopathy prolonged fever with diarrhea, splenomegaly, and altered sensorium. Seizures may occur but are uncommon. Shigella encephalopathy Fever preceded the onset of diarrhea which was non-invasive in
- character.
- Pyogenic meningitis history is rather long and there are no signs of meningeal irritation.
- Hypernatremic dehydration The onset of dehydration is often delayed and the use of concentrated ORS is well known to produce hypernatremia and seizures. However, high-grade fever and splenomegaly cannot be explained.
- Reye syndrome the presence of high-grade continuous fever and the onset of vomiting later during the disease is against this possibility.
- Brain abscesses the absence of any focal neurological signs and the lack of any predisposing conditions, like head injury, otitis media, and congenital cyanotic heart disease, are against this possibility.
P
Complete hemogram, serum electrolytes, blood glucose, liver and kidney function tests, stool microscopic examination and culture, widal test, blood culture, CSF examination, and contrast-enhanced CT scan of the head.
Administer IV fluids, and give appropriate antibiotics and anticonvulsants.
2. Flow Sheet Analysis
It has been proposed to simplify the diagnostic approach for community health workers by the use of algorithms.
3. Diagrammatic Summary
It is useful to ascertain and assimilate the information at a glance.
Maintain an accurate record of history, physical examination, and follow-up both in the hospital and ambulatory practice given the increasing incidence of medical litigation following the enactment of the Consumer Protection Act in 1986.
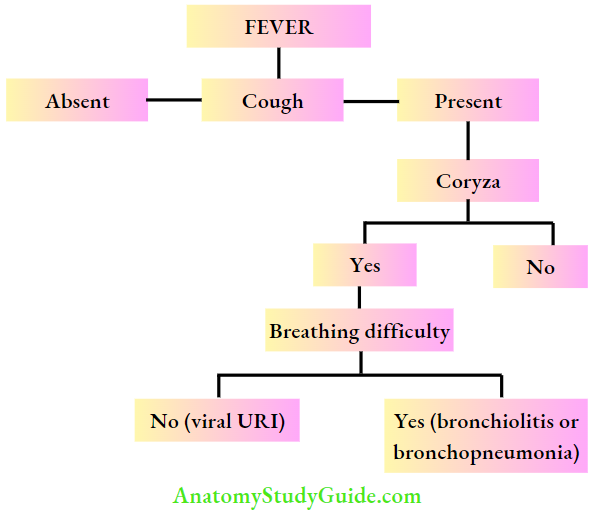
The algorithm gives a simplified step-wise approach to a health worker to identify the cause of fever in a child.
The presence of cough and coryza are useful clues localizing infection to the upper respiratory tract while breathing difficulty is diagnostic of acute lower respiratory tract infection.
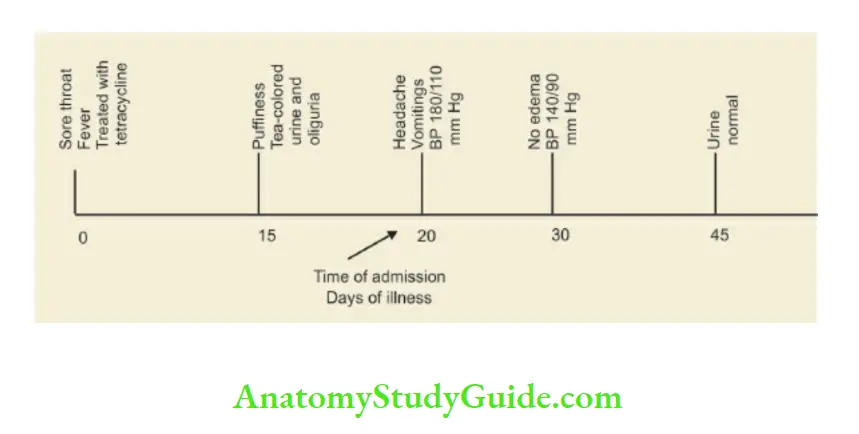
Typical diagrammatic summary of a child with post-streptococcal acute glomerulonephritis. Inappropriate treatment of streptococcal pharyngitis with tetracycline leads to classical manifestations of AGN followed by complete recovery.
Leave a Reply