Milestone In Periapical Radiographic Interpretation Of Dental Structures
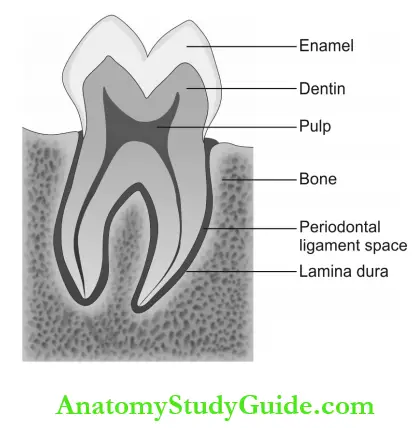
Table of Contents
Read And Learn More: Oral Medicine and Radiology Question And Answers
Milestone In Periapical Radiographic Interpretation Of Image Nomenclatures
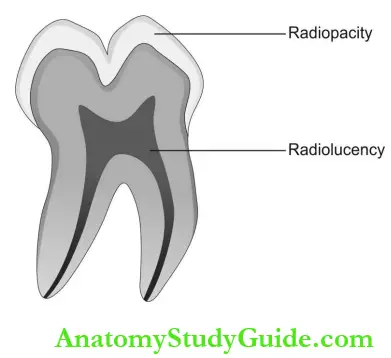
- Radiolucency: An area of darkness on a radiograph that indicates an object of low density which allows complete or partial penetration of X-rays.
- Radiopacity: An area of lightness on a radiograph indicating the density of an object that prevents the penetration of X-rays.
- Interpretation: Radiographic interpretation is the ability to assess and recognize the image revealed by a radiograph to diagnose a lesion, disease or condition revealed clinically.
Milestone In Periapical Radiographic Interpretation Diagnostic Quality Of Radiographs
Diagnostic Prichard criteria: To determine the adequate diagnostic accuracy of periapical radiographic angulation:
- The radiograph should show the tips of molar cusps without or with little revealing of the occlusal surface. Enamel caps and pulp chambers should be clearly outlined.
- Open interproximal spaces.
- Proximal contacts should not overlap unless teeth are malpositioned.
- Anatomical Landmarks: The following structures are more frequently seen in the intraoral periapical images.
Milestone In Periapical Radiographic Interpretation Landmarks In Maxilla
Midpalatine suture: Vertical radiolucent line present in the midline between two maxillary central incisors.
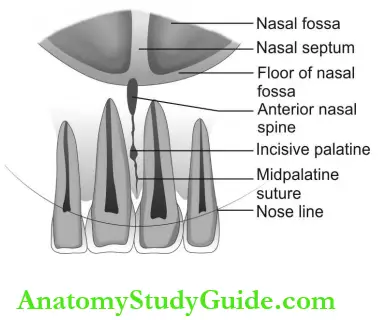
Incisive foramen or anterior palatine fossa: Round or ovoid radiolucent structure measuring less than 6 mm in diameter present between the roots of two maxillary central incisors, slightly above the root apices.
Anterior nasal spine: Radiopaque structure in the midline above the incisive foramen.
Nasal septum: Thick radiopaque line present in the midline and separates two nasal fossa. Y line of Ennis: The floor of the nasal fossa and anterior wall of the maxillary sinus intersect and form an inverted “Y” (upside down – X) line known as the Y line of Ennis.
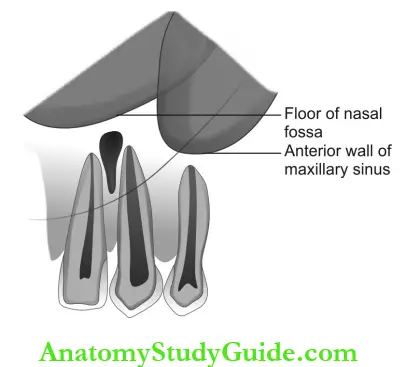
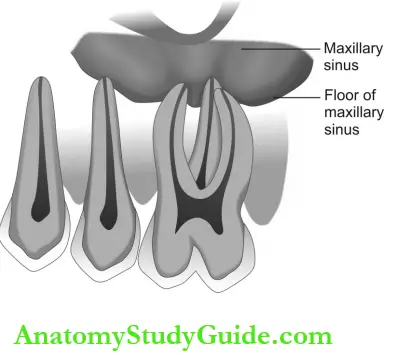
The floor of maxillary sinus: Delicate, curvy, radiopaque line that overlaps the roots of maxillary premolars and molars or dips between the roots of premolars and molars. It encircles a radiolucent maxillary sinus.
- Maxillary sinus:
- The well-defined radiolucent structure above the maxillary premolars and molars overlapping their root apices.
- Sometimes, fine radiopaque lines may run within the radiolucent space and compartmentalize the space indicating sinus septa.
- Pneumatization: Expansion of the maxillary sinus floor and invasion into the edentulous alveolar process.
- Malar or zygomatic process: Thick, “U” shaped radiopaque structure that superimposes the roots of maxillary molars.
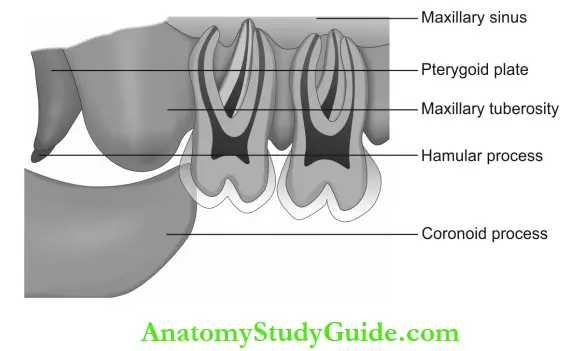
- Maxillary tuberosity: Round radiopaque projection representing the end of the maxillary process. It is seen distal to the maxillary 3rd molar.
- Coronoid process of the mandible: Radiopaque structure resembling finger pad (proximal phalanx), present distal to and overlapping the crown of maxillary 3rd molar.
Landmarks In Mandible:
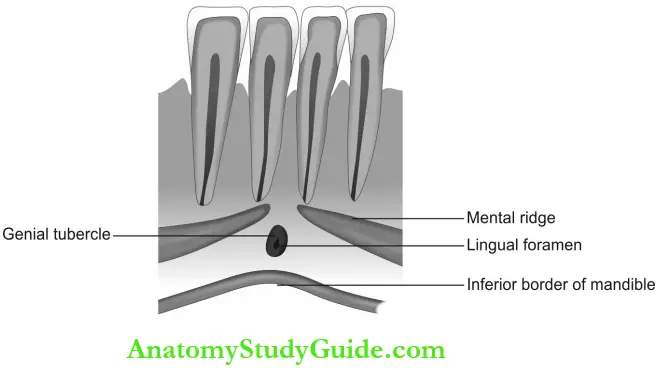
- Lingual foramen: Small radiolucent dot surrounded by a radiopaque periphery, seen in the mandibular anterior alveolar process along the midline and well below the roots of central incisors. Nutrient vessels pass through this foramen.
- Genial tubercles: Round radiopaque structure that surrounds the lingual foramen.
- They are otherwise known as superior and inferior mental spines which are 4 in number and coalesced. On close observation of the radiograph, we can see 2 on either side of the lingual foramen. Along the superior mental spines, genioglossal muscle is attached and on inferior mental spines, geniohyoid muscle is attached.
Mandibular Canine:
- Mental ridge: Appears as an inverted ‘v-shaped structure that extends between the premolars and crosses the midline at the inferior border of the mandible and apices of anterior teeth.
- Mental fossa: Faint, diffused radiolucency overlying the apical 3rd of roots of mandibular incisors. Care should be taken to avoid misinterpretation as pathology.
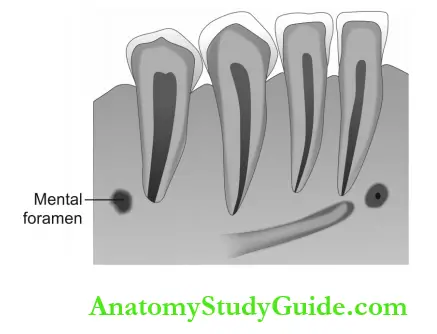
- Mental foramen: Round, radiolucent structure present between the roots of mandibular premolars.
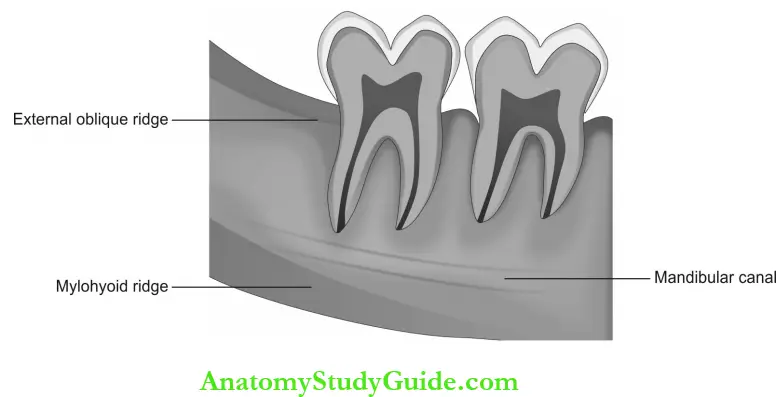
Mandibular Molar:
- External oblique ridge: A thin radiopaque line that extends from the anterior border of the ramus of the mandible and slides down to the cervical region of 3rd molar.
- Internal oblique ridge: A thin radiopaque line that runs below and in close approximation with the external oblique ridge.
- Mylohyoid ridge: Radiopaque line running posteroanterior from the 3rd molar to the premolar region along the root apices.
- Inferior alveolar canal or mandibular canal: Radiolucent line running postero- anteriorly from the lingual foramen on the ramus of mandible and ends at the mental foramen. Two thin radiopaque lines outline this radiolucent canal both superiorly and inferiorly representing cortical bone boundaries.
- Submandibular gland fossa: Occasionally seen as a diffuse area of radiolucency below the root apices of mandibular molars.
Milestone In Periapical Radiographic Interpretation Normal Anatomical Structures
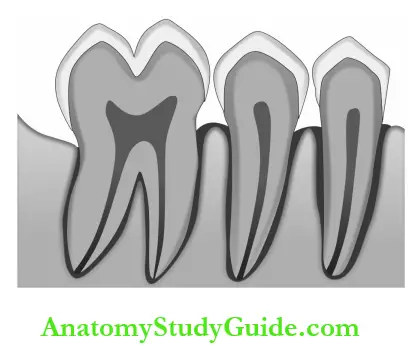
Pulp cavity: The pulp cavity is the central part of the tooth known as the pulp chamber which extends into the root as the root canal, which opens into the periodontium via apical foramen and is enclosed all around by dentin.
Healthy periapical tissues exhibit the following important features:
- Lamina dura: A thin, continuous radiopaque line adjacent to the radiolucent line.
- Periodontal ligament space (PDL): A thin, continuous radiolucent line around the outline of the root.
- The trabecular pattern and density of the surrounding cancellous bone.
Lamina Dura:
- It appears as a radiopaque line that covers the alveolar socket and extends on the top of the interdental bone.
- Because the facial and lingual bony plates are obscured by dense root structures, radiographic evaluation of bone changes in periodontal disease is based mainly on the interdental septa.
- With periodontal disease, the crestal lamina dura is indistinct, irregular, fuzzy, and radiolucent. Its appearance in the radiograph is influenced by the shape and position of the root and angulation of the X-ray beam.
Periodontal ligament space: With disease, the periodontal ligament space may appear at varying thicknesses that can show that the disease involvement is not consistent around the entire root.
Alveolar bone and crest:
- Normal alveolar bone-supporting dentition has a characteristic radiographic appearance. It exhibits a thin opaque cortical bone that covers the alveolar crest. The height of the crest lies at a level approximately 0.5-2.0 mm below the level of cementoenamel junctions (CEJ) and is continuous with the lamina dura of adjacent teeth.
- The distance considered as normal in young individuals would be from 1 to 2 mm between the cementoenamel junction and the bone crest.
- Crest is the most coronal portion of the alveolar process.
- Between incisor teeth, the alveolar crest will usually appear pointed. In posterior teeth, it appears flat and will be parallel to a line between the adjacent CEJs where the enamel thins and disappears.
- When viewing the lamina dura and the periodontal ligament, only the interproximal portions are visible. The buccal and lingual areas are not seen in the radiograph.
- It shows signs of apical recession with age or in periodontal diseases. Widening of the periodontal ligament space and loss of lamina dura can be interpreted as resorption of the alveolar bone.
Furcation:
- The root complex is divided into two parts as root body and root cone. Furcation is the area at which the roots are separated.
- The part of the root before furcation is called as root body and the part of the root following the furcation area is known as the root cone.
- Widening of PDL space at the apex of the inter-radicular bony crest of the furcation is an indication of periodontal disease.
Trabecular bone: It is composed of thin radiopaque plates and rods surrounded by many small radiolucent marrow compartments
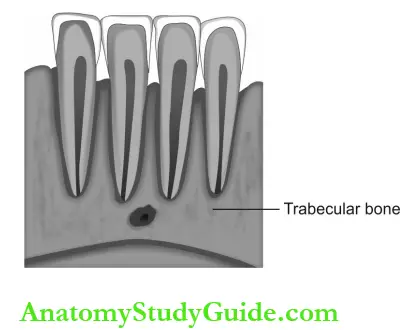
.
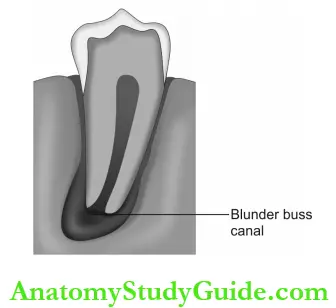
Blunder buss canal: Incompletely formed root with open apex in which the apical diameter of the pulp canal is greater than the coronal diameter. The canal walls are flared and diverged with funnel-shaped apex.
Leave a Reply