Emetics And Antiemetics
Nausea denotes the feeling of impending vomiting, whereas vomiting refers to the forceful expulsion of the contents of the stomach and upper intestinal tract through the mouth. Retching is the laboured rhythmic respiratory activity that usually precedes vomiting.
Table of Contents
Read And Learn More: Pharmacology for Dentistry Notes
- Mechanism of vomiting The act of vomiting is controlled by vomiting centre in the medulla. Stimuli are relayed to this centre from peripheral areas, i.e. gastric mucosa and other parts of GIT. Sensory stimuli also arise within the central nervous system (CNS) itself (i.e. cerebral cortex and vestibular apparatus) – the impulses are transmitted to the vomiting centre.
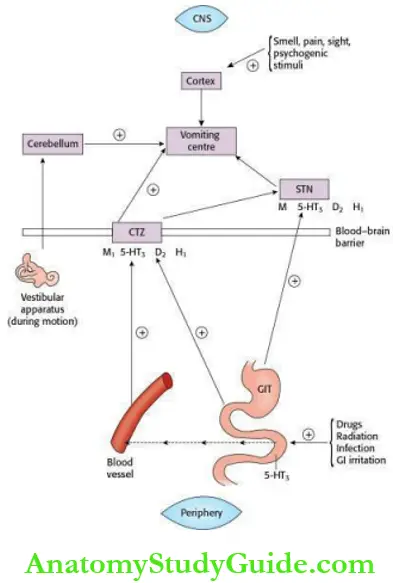 The lack of blood–brain barrier (BBB) at the chemoreceptor trigger zone (CTZ) allows it to be directly stimulated by blood-borne drugs and toxic substances. Nausea and vomiting may be the symptoms of pregnancy, serious organic disturbances of almost any of the viscera or may be produced by infection, drugs, radiation, painful stimuli, motion sickness, metabolic and emotional disturbances. The main neurotransmitters involved in the control of vomiting are acetylcholine (ACh), histamine, 5- hydroxytryptamine (5-HT) and dopamine.
The lack of blood–brain barrier (BBB) at the chemoreceptor trigger zone (CTZ) allows it to be directly stimulated by blood-borne drugs and toxic substances. Nausea and vomiting may be the symptoms of pregnancy, serious organic disturbances of almost any of the viscera or may be produced by infection, drugs, radiation, painful stimuli, motion sickness, metabolic and emotional disturbances. The main neurotransmitters involved in the control of vomiting are acetylcholine (ACh), histamine, 5- hydroxytryptamine (5-HT) and dopamine.
Emetics
The drugs that cause vomiting are called emetics. Examples are mustard, common salt, ipecac and apomorphine. Mustard and common salt are commonly used in household emetics. Syrup ipecac is a safer emetic than apomorphine. Emetics are indicated in certain cases of poisoning.
- Contraindications for the use of emetics are:
- Unconscious patients, because of risk of aspiration.
- Corrosive and caustic poisoning – further damage to the oesophageal lining occurs.
- Poisoning due to CNS stimulants – because of risk of precipitation of seizures.
- Kerosene poisoning – as aspiration may occur.
Antiemetics
The drugs that are used to prevent or control vomiting are called antiemetics.
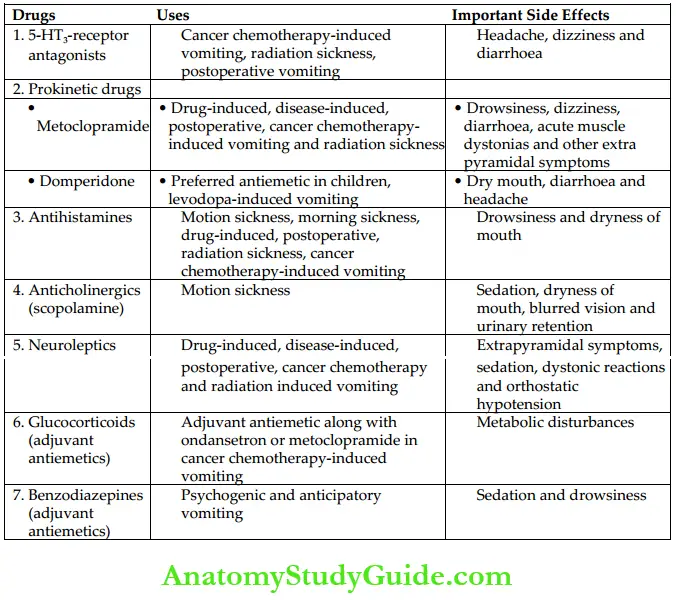
Antiemetics with Their Uses and Side Effects
- Classification
- 5-HT3-receptor antagonists: Ondansetron, granisetron, dolasetron, palonosetron, ramosetron.
- Prokinetic agents: Metoclopramide, domperidone
- Antihistamines (H1-blockers): Dimenhydrinate, diphenhydramine, cyclizine, meclizine, hydroxyzine, promethazine, doxylamine
- Anticholinergics: Scopolamine (hyoscine), dicyclomine
- Neuroleptics: Chlorpromazine, fluphenazine, prochlorperazine, haloperidol
- Neurokinin (NK1)-receptor antagonists: Aprepitant, fosaprepitant
- Adjuvant antiemetics:
- Glucocorticoids: Betamethasone, dexamethasone, methylprednisolone
- Benzodiazepines: Lorazepam, alprazolam
- Dronabinol, nabilone
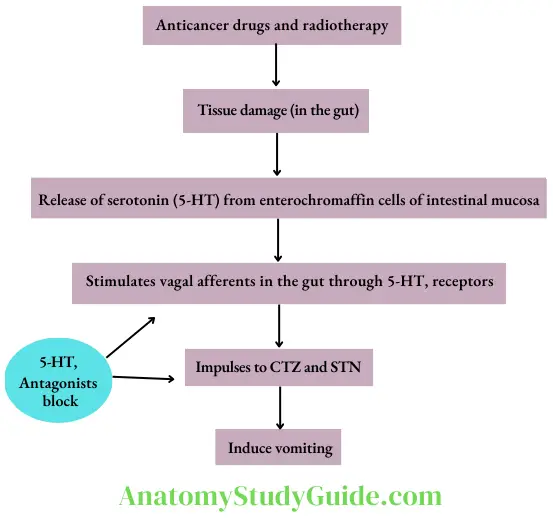
- 5-HT3-receptor antagonist Ondansetron is the prototype drug. Other drugs are granisetron, dolasetron, palonosetron and ramosetron. Their antiemetic effect is mainly due to the blockade of 5- HT3 receptors on vagal afferents in the gut (peripheral action). In addition, they also block 5-HT3 receptors in the CTZ and solitary tract nucleus (central action).
- Pharmacokinetics 5-HT3 antagonists are well absorbed after oral administration. The metabolites are excreted in urine and faeces. Some of these agents are also available for intravenous administration. Ondansetron can also be administered intramuscularly. Granisetron is more potent and longer-acting than ondansetron. A transdermal patch of granisetron is available for the prevention of cancer chemotherapy-induced vomiting. Palonosetron is the longest-acting 5HT3-receptor antagonist. Ramosetron can be administered orally as well as intravenously.
- Uses
- 5-HT3 antagonists are the most effective agents for the prevention and treatment of chemotherapy-induced nausea and vomiting. Combination with dexamethasone/diazepam/aprepitant enhances the antiemetic efficacy.
- They are also effective in hyperemesis of pregnancy, postoperative, post-radiation and drug-induced vomiting; but they are ineffective against motion sickness.
- Adverse effects of 5-HT3 antagonists are well tolerated. They may cause headaches, dizziness and diarrhoea.
Prokinetic Drugs
Drugs that promote coordinated movement of upper GIT and hasten gastric emptying are called prokinetic drugs. They include metoclopramide, domperidone and mosapride. Of these, metoclopramide and domperidone are used as antiemetics.
- Metoclopramide Metoclopramide is a dopamine (D2)-receptor antagonist. It has two important actions – central and peripheral.
- Central actions: The antiemetic effect of metoclopramide is mainly due to the blockade of D2 receptors in CTZ. At high concentrations, it also blocks 5-HT3 receptors in CTZ.
- Prokinetic effect on upper GIT: Metoclopramide enhances the release of ACh from myenteric neurons. This effect is due to D2-antagonism and 5-HT4 agonism in the GIT. Thus, peripherally, it has a prokinetic effect on upper GIT and enhances the rate of gastric and duodenal emptying.
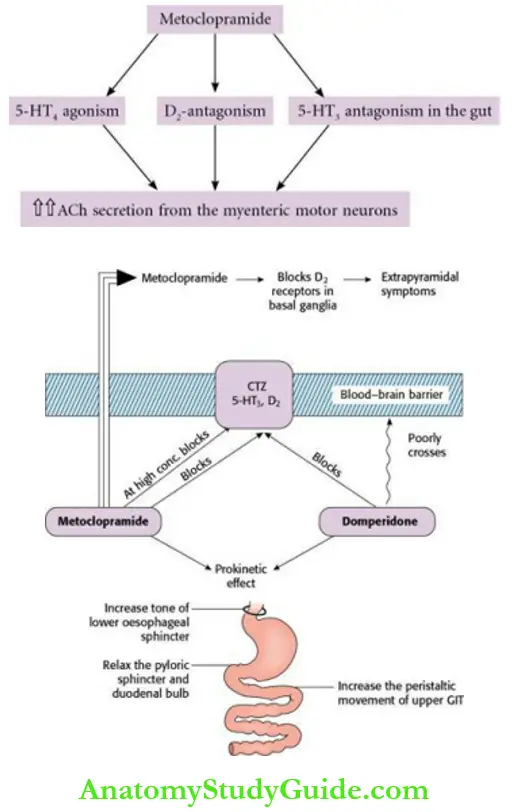
- The effects of metoclopramide on upper GIT are:
- Increase in tone of the lower oesophageal sphincter (LES).
- Increase in tone and amplitude of antral contractions.
- Relaxation of pyloric sphincter.
- Increase in the peristalsis of the small intestine.
- Thus, it promotes the forward movement of contents in the upper GIT. It does not have any significant effect on the motility of the colon.
- The effects of metoclopramide on upper GIT are:
- Pharmacokinetics Metoclopramide is rapidly absorbed after oral administration. It can also be administered by i.m. and i.v. routes. The onset of action is within half an hour after oral dose; and a few minutes after parenteral administration. It has a short half-life of 4 h; is poorly bound to plasma proteins; crosses BBB. The drug is partly metabolized and excreted in urine.
- Uses
- As an antiemetic: Metoclopramide is effective for the prevention and treatment of:
- Disease-associated vomiting.
- Drug-induced vomiting (not used to control levodopa-induced vomiting).
- Postoperative vomiting.
- Cancer chemotherapy-induced vomiting.
- Vomiting due to radiation sickness.
- It is less effective against motion sickness.
- Gastroesophageal reflux disease (GERD): Metoclopramide produces symptomatic relief in patients with reflux oesophagitis by increasing the tone of the lower oesophageal sphincter. By prokinetic effect, it also reduces the volume of gastroduodenal contents that reflux into the oesophagus. It is less effective than proton pump inhibitors (PPIs) and H2-blockers.
- To alleviate symptoms associated with gastric stasis in patients with diabetes, postoperative or idiopathic gastroparesis: Gastric stasis is characterized by upper abdominal discomfort, distension, bloating, nausea, vomiting, etc. By prokinetic effect, it controls the above symptoms.
- To stimulate gastric emptying before general anaesthesia in emergency surgeries.
- Metoclopramide has been used in the treatment of intractable hiccups.
- As an antiemetic: Metoclopramide is effective for the prevention and treatment of:
- Adverse effects They are drowsiness, dizziness and diarrhoea. Acute dystonias (spasms of muscles of the face, tongue, neck and back) can occur. Other extrapyramidal symptoms (EPS: tremor, rigidity, etc.) are due to the blockade of D2-receptors in basal ganglia (drug-induced Parkinsonism). Acute dystonias can be treated with centrally acting anticholinergics (for example benzhexol, benztropine) or antihistamines with anticholinergic action (for example promethazine, diphenhydramine). Long-term use may lead to gynaecomastia, galactorrhoea and menstrual irregularities Due to the blockade of the inhibitory effect of dopamine on prolactin release.
- Drug interactions Metoclopramide accelerates the absorption of diazepam but reduces digoxin absorption by its prokinetic effect.
- Domperidone
- It is a prokinetic agent and has effects almost similar to metoclopramide. Its antiemetic and prokinetic effects are due to the blockade of dopamine (D3)-receptors. It is less potent and less efficacious than metoclopramide. It poorly crosses BBB, hence extrapyramidal side effects are rare.
- Domperidone is a preferred antiemetic in children, as it rarely produces EPS. It counteracts vomiting induced by levodopa without affecting its anti-Parkinsonian effect, as it poorly crosses BBB. Hence, it is preferred over metoclopramide for treating vomiting induced by these drugs. Atropine blocks the prokinetic effect of metoclopramide but not that of domperidone.
- It is usually administered orally, but its oral bioavailability is low because of extensive first-pass metabolism; metabolized in the liver and metabolites are excreted in urine. The important side effects are dryness of mouth, diarrhoea, headache, skin rashes, galactorrhoea and menstrual irregularities.
- Other prokinetic agents are mosapride and itopride. Mosapride and itopride improve peristalsis. They are prescribed for motility disorders.
- Antihistamines (H1-blockers) H1-blockers are mainly useful for the prevention of motion sickness. They are also effective in morning sickness, postoperative and other types of vomiting. Dimenhydrinate, diphenhydramine, doxylamine, promethazine, cyclizine and meclizine are some of the H1-blockers that have antiemetic properties. Their antiemetic effect is due to sedative, H1 blockade and central anticholinergic actions. Cyclizine and meclizine have less sedative effects. Meclizine has a long duration of action (24 h).
- Anticholinergics Scopolamine (hyoscine) is the drug of choice to prevent motion (travel) sickness. It blocks afferent impulses from the vestibular apparatus to the vomiting centre by its anticholinergic action. Its sedative effect also contributes to its antiemetic effect. Scopolamine is not effective for other types of vomiting. Scopolamine is administered orally, intramuscularly or as a transdermal patch.
- Neuroleptics are potent antiemetics. Their antiemetic effect is due to the blockade of D2-receptors in the CTZ. In addition, they have anticholinergic and antihistaminic actions. Among these, prochlorperazine is commonly used as an antiemetic. They are effective in the treatment of vomiting due to drugs, uraemia and systemic infections. They are also useful for the treatment of chemotherapy and radiation-induced vomiting. They are less effective in motion sickness. The common side effects are sedation, muscle dystonias and other extrapyramidal symptoms, dryness of mouth, hypotension, etc.
- Neurokinin (NK1)-receptor antagonists Aprepitant (orally) and fosaprepitant (infused intravenously) are neurokinin-receptor antagonists. They block the action of substance P in CTZ and NTS. They are highly effective in the prevention of delayed emesis following moderately or highly emetogenic chemotherapy and increase the efficacy of standard antiemetic regimens (for example 5-HT3 antagonist + dexamethasone). They are well tolerated; flatulence can occur.
- Adjuvant antiemetics
- Glucocorticoids, such as dexamethasone, betamethasone and methylprednisolone are used as adjuvant antiemetics. These agents are commonly used in combination with ondansetron or metoclopramide in the treatment of anticancer drug-induced vomiting. The beneficial effect of steroids is due to their anti-inflammatory property.
- Benzodiazepines Lorazepam, diazepam and alprazolam are used to control psychogenic and anticipatory vomiting. The beneficial effect is mainly due to their sedative, amnesic and antianxiety effects.
- Dronabinol is useful in anticancer drug-induced vomiting not responding to other antiemetics.
Antidiarrhoeal Agents
Generally, the term ‘diarrhoea’ denotes the passage of unusually loose or watery stools at least three times or more in a 24-hour period(according to WHO).
Based on the pattern of onset, there are two types of diarrhoea, i.e. acute and chronic. In most cases, acute diarrhoea is caused by infectious agents. In acute diarrhoea, irrespective of the aetiology, emphasis is given to preventing dehydration, which is responsible for most mortalities.
Diarrhoea is called chronic when it persists for more than 2 weeks. In chronic diarrhoea, finding out the cause is important for effective management.
Management Of Diarrhoea
- Oral and parenteral rehydration
- Antimotility agents: Opioids –codeine, loperamide, diphenoxylate
- Antisecretory agents: Racecadotril, octreotide
- Probiotics
- Antimicrobial agents
- Oral rehydration solution (ORS)
- In acute diarrhoea, it is important to maintain water and electrolyte balance with proper fluid replacement (rehydration). Oral rehydration seems to be the simplest, safest and least expensive method of choice for acute diarrhoea. WHO-ORS contains sodium chloride 2.6 g, potassium chloride 1.5 g, sodium citrate 2.9 g and glucose 13.5 g. It has to be dissolved in 1 L of water. This provides sodium 75 mM, potassium 20 mM, chloride 65 mM, citrate 10 mM and glucose 75 mM. The total osmolarity is 245 mOsm/L.
- The amount of sodium and glucose is lower than those in older preparations; this promotes better absorption of water from the solution. Sodium and potassium are administered to replace the losses. Sodium is transported along with glucose by sodium-glucose cotransporter in the ileum. Citrate, a base, corrects acidosis. ORS decreases stool volume and vomiting. It is also effective in cholera. ORS is also useful in heat stroke and the maintenance of hydration in burn patients.
- In case of severe diarrhoea with dehydration, intravenous fluids are indicated. WHO recommends the use of zinc supplements (10–14 days) with ORS in acute diarrhoea in children. It decreases intestinal secretions, promotes the regeneration of intestinal epithelium and reduces the duration and severity of diarrhoea.
- Antimotility and antisecretory agents
- Codeine: It is a natural opium alkaloid. It reduces GI motility and produces constipation. It has abuse potential.
- Diphenoxylate: It is related to pethidine. In high doses, it has abuse liability, hence is usually available in combination with a small dose of atropine to discourage abuse or overdosage. The side effects are constipation, paralytic ileus and drug addiction. This drug has been banned in many countries.
- Loperamide: It is an opiate analogue and has a more potent antidiarrhoeal effect than morphine. By interacting with µ-opioid receptors in the gut, loperamide reduces GI motility, decreases intestinal secretion and increases the anal sphincter tone. It is orally effective and has a rapid onset of action. It poorly penetrates BBB and has no abuse potential. It has been used in both acute and chronic diarrhoea. It can also be used in travellers’ diarrhoea. The toxic effects are skin rashes, headache and paralytic ileus. It should not be used in children less than 4 years of age.
- Octreotide: It is an analogue of somatostatin which is useful in secretory diarrhoea due to hormone-secreting tumours of GIT and pancreas. It can be used to treat diarrhoea in patients with AIDS.
- Racecadotril: Racecadotril (prodrug) → active metabolite → enkephalinase inhibitor → inhibits degradation of enkephalins in intestinal mucosa → increases the concentration of enkephalins in intestinal mucosa → decreases intestinal secretion. It is used in acute secretory diarrhoea. It can be used in children. Side effects are nausea, vomiting and drowsiness.
- Antimotility drugs produce only symptomatic relief in diarrhoea and should be avoided in acute infectious diarrhoeas. These drugs also increase intraluminal pressure, hence they should be avoided in inflammatory bowel disease (IBD).
- Probiotics They consist of either bacteria or yeast-like Lactobacillus, Bifidobacterium and Saccharomyces boulardii. They may produce beneficial effects by competing with pathogens in the gut.
- Antimicrobials Irrational use of antimicrobials should be avoided. They are indicated in acute bloody diarrhoea. They are also useful in cholera, pseudomembranous enterocolitis and amoebic dysentery. Commonly used chemotherapeutic agents for the treatment of infectious diarrhoea are ciprofloxacin, doxycycline, cotrimoxazole, metronidazole, vancomycin and tinidazole.
Laxatives (Purgatives, Cathartics)
Laxatives are drugs that facilitate the evacuation of formed stools from the bowel.
Purgatives cause evacuation of watery stools. The terms laxatives, purgatives and cathartics are often used interchangeably.
Classification (according to the mechanism of action)
- Bulk laxatives
- Dietary fibre – Bran, methylcellulose, ispaghula (isabgol)
- Stimulant or irritant laxatives
- Bisacodyl, sodium picosulfate, senna, cascara sagrada, castor oil, prucalopride
- Osmotic laxatives
- Magnesium sulfate, magnesium hydroxide, sodium phosphate, sodium sulfate, lactulose
- Stool softeners (emollient laxatives)
- Docusates, liquid paraffin.
Bulk-forming Laxatives
They are indigestible, hydrophilic substances like bran, methylcellulose, agar and paghula, which absorb water, swell up and increase the bulk of stools. They cause mechanical distension, so stimulate peristalsis and promote defecation. It takes 1–3 days for the evacuation of formed stools.
Ispaghula is obtained from the seed of Plantago ovata. Large amounts of water should be taken with bulk purgatives to avoid intestinal obstruction. A fibre diet should be encouraged in patients with irritable bowel syndrome but should be avoided in those with megacolon or megarectum. The side effects include abdominal discomfort and flatus
Stool Softeners (Emollient Laxatives)
- Docusate The common docusate salt used is dioctyl sodium sulfosuccinate (DOSS). Docusates are anionic detergents. They lower the surface tension of stool, thereby causing accumulation of fluid and fatty substance, thus softening the stools. These agents act within 1–3 days. They are administered orally or as a retention enema. Docusates increase the absorption of liquid paraffin, hence should not be given together.
- Liquid paraffin Liquid paraffin is mineral oil and is administered orally. It softens stools. It also has a Lubricant effect, and thus helps in smooth defecation. It is useful in patients with cardiac disease because it prevents straining during defecation.
- Adverse effects of liquid paraffin
- Lipid pneumonia may occur due to the entry of the drug into the lungs, hence liquid paraffin should not be given at bedtime and in a lying down position.
- Long-term use may cause malabsorption of vitamins A, D, E and K (fat-soluble vitamins).
- Leakage of faecal matter through the anal sphincter may lead to the soiling of clothes.
- Adverse effects of liquid paraffin
Stimulant (Irritant) Laxatives
These agents have direct action on enteric neurons and GI mucosa. They increase prostaglandin (PG) and cyclic adenosine monophosphate (cAMP) levels, but inhibit Na+, K+–ATPase activity in the intestinal mucosa.
This causes an increased secretion of water and electrolytes by the mucosa thus stimulating peristalsis. They cause evacuation of semifluid stools. Chronic use of stimulant laxatives may cause an atonic colon. Large doses may cause loss of fluid and electrolytes. They are contraindicated in pregnancy, as they cause reflex stimulation of the uterus.
- Bisacodyl The major site of action is the colon. It is available as an enteric-coated oral tablet and also as a rectal suppository. It is poorly absorbed after oral administration and undergoes activation by esterases in the bowel. Hence, the effect is seen only after 6–8 hours of oral administration. Therefore, it is usually given at bedtime. Rectal suppositories act more rapidly within an hour by irritation of rectal mucosa. Bisacodyl is used in constipation and to empty the bowel before endoscopy, surgery and radiological investigations. The side effects are local irritation and inflammation.
- Sodium picosulfate is a stimulant purgative given orally at bedtime. It can be used to evacuate the bowel before surgery or colonoscopy.
- Prucalopride Prucalopride, a prokinetic drug, is a 5-HT4 agonist. It is useful in chronic constipation not responding to laxatives. It increases colonic motility.
- Anthraquinone derivatives The popular anthracene purgatives are senna and cascara. They take 6–8 h to act, hence they are usually administered at bedtime to produce their effect in the morning. They are poorly absorbed in the small intestine. The unabsorbed portion reaches the colon, where it is reduced by bacteria to control that acts locally and induces purgation.
- They should not be prescribed to lactating mothers, as they are secreted in milk. The side effects are skin rashes, black pigmentation of the colonic mucosa and discolouration of urine. Prolonged use can cause colonic atony.
Osmotic Laxatives
They are salts of magnesium, sodium or potassium. Those having magnesium or phosphate are known as saline laxatives. In addition, magnesium salts cause the release of cholecystokinin. To mask the bitter taste, they are often administered with fruit juice.
The important osmotic laxatives are magnesium sulfate (Epsom salt), magnesium hydroxide (milk of magnesia), sodium phosphate, lactulose, etc. They should be avoided in young children and patients with renal failure, as they may cause CNS or cardiac depression.
Sodium phosphate is commonly used orally for colon preparation before surgery or colonoscopy. It can also be used as an enema. Sodium salts should be avoided in cardiac patients.
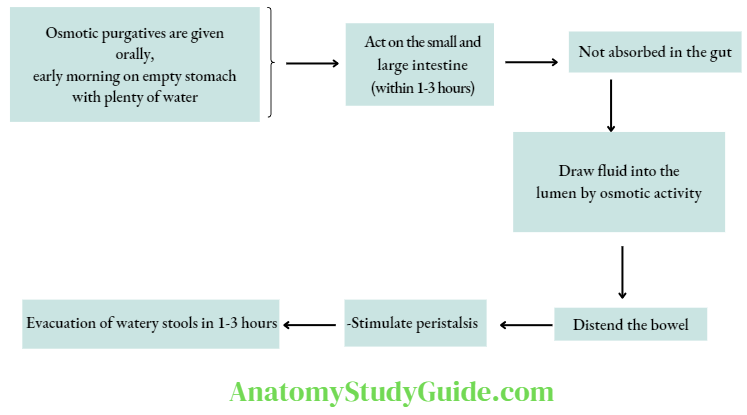
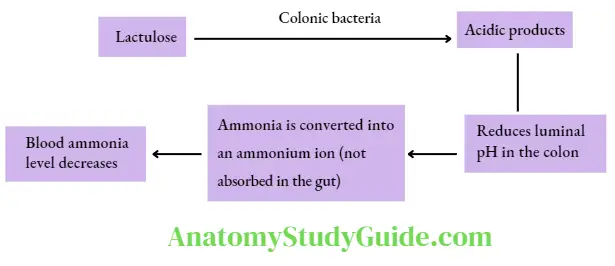
- Lactulose is a disaccharide of fructose and galactose. Lactulose is available as liquid and powder. On oral administration, it is not absorbed through GI mucosa. Colonic bacteria convert it into acidic products, which exert an osmotic effect – draw fluid into the lumen and distend it; thus useful in constipation. It produces soft-to-loose stools. It can be used to treat constipation in children and pregnant women. Lactulose is used in hepatic coma to reduce blood ammonia levels. The side effects include abdominal discomfort and flatulence.
Uses Of Laxatives With The Preparation Of Choice
- Acute functional constipation (atonic or spastic) – bulk laxatives.
- To avoid straining during defecation in patients with cardiovascular disease, eye surgery, hernia, etc. – docusate or bulk laxatives.
- In patients with hepatic coma reduce the blood ammonia level – lactulose.
- Preoperatively in bowel surgery, colonoscopy and abdominal X-ray – osmotic laxatives or bisacodyl.
- Following anthelmintics (example for Taenia solium) – saline laxatives to expel the worm segments.
- In drug poisoning to wash out the poisonous material from the gut – saline laxatives.
- To treat constipation in children and pregnant women – lactulose.
Treatment Of Opioid-Induced Constipation
Laxatives are the preferred drugs. If the patient does not respond to laxatives, opioid antagonists like methylnaltrexone (s.c.) and naloxegol (oral) can be used.
Pharmacotherapy Of Peptic Ulcer And Gastroesophageal Reflux Disease
- Physiology of gastric secretion The stomach secretes roughly about 2–3 L of gastric juice per day. The chief or peptic cells secrete pepsinogen, which is converted to pepsin by gastric acid. Parietal or oxyntic cells secrete acid and intrinsic factor (IF). Superficial epithelial cells secrete alkaline mucus and bicarbonate ions.
- Regulation of gastric acid secretion The secretion of gastric acid by parietal cells is regulated by ACh, histamine, gastrin and prostaglandin E2 (PGE2). Binding of histamine, ACh and gastrin to their specific receptors on the parietal cell results in increased secretion of gastric acid. In contrast, the binding of PGE2 to its receptor decreases gastric acid secretion. There are various phases of gastric acid secretion – basal, cephalic and hormonal. A membrane-bound proton pump H+,K+– ATPase plays an important role in the final step of gastric acid secretion.
- Damage to the mucosa and deeper tissue exposed to acid and pepsin is known as peptic ulcer. The exact cause of peptic ulcer is not clear. In most cases, peptic ulcers are caused by Helicobacter pylori infection or the use of nonsteroidal anti-inflammatory drugs (NSAIDs).
- Classification of drugs used in peptic ulcer
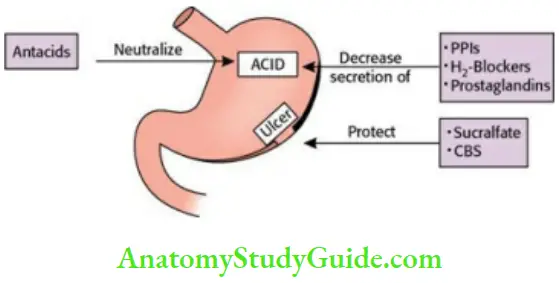
- Drugs that inhibit gastric acid secretion
- Proton-pump inhibitors (PPIs): Omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole.
- H2-receptor antagonists (H2-blockers): Cimetidine, ranitidine, famotidine, roxatidine, nizatidine.
- Antimuscarinic agents (anticholinergic agents): Pirenzepine, telenzepine.
- Prostaglandin analogues: Misoprostol.
- Ulcer protectives
- Sucralfate, colloidal bismuth subcitrate (CBS).
- Drugs that neutralize gastric acid (antacids)
- Nonsystemic antacids: Magnesium hydroxide, magnesium trisilicate, aluminium hydroxide, calcium carbonate.
- Systemic antacids: Sodium bicarbonate, sodium citrate.
- Anti–H. pylori agents Amoxicillin, tetracycline, clarithromycin, metronidazole, tinidazole, bismuth subcitrate, H2-antagonists and proton pump inhibitors.
- Drugs that inhibit gastric acid secretion
Drugs That Inhibit Gastric Acid Secretion
- Proton pump inhibitors (PPIs)
- Mechanism of action of proton pump inhibitors.
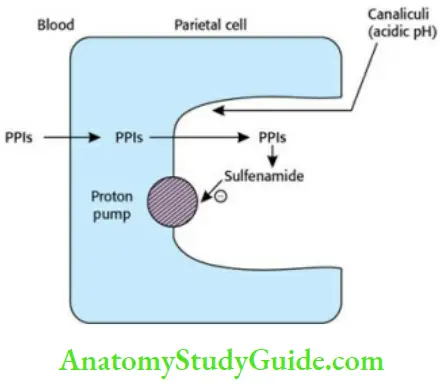
- Proton pumps H+, K+-ATPase is a membrane-bound enzyme that plays an important role in the final step of gastric acid secretion (basal and stimulated; Omeprazole is the prototype drug. The other PPIs are lansoprazole, pantoprazole and rabeprazole.
- PPIs (prodrugs) → absorbed in small intestine → blood → diffuse into parietal cells → canaliculi of the cell (acidic pH) → converted to sulfenamide (active, charged form). The activated form (sulfenamide) binds covalently with the SH group of the proton pump and irreversibly inactivates it. PPIs are the most powerful inhibitors of gastric acid secretion.
- They inhibit both fasting and stimulated acid secretion. As PPIs act in the final step of acid secretion, they are effective in inhibiting acid production following any stimulation. PPIs are administered orally about 30 min before food because food stimulates the secretion of acid (in the canaliculi of the parietal cell), which is necessary for the activation of PPIs. Food decreases the absorption of PPIs. Though the half-life of PPIs is short (~1.5 h), acid secretion is suppressed for up to 24 h as they cause irreversible inhibition of proton pumps.
- In the commonly used doses, PPIs suppress acid production by about 80%–98%. PPIs are available as enteric-coated form or as powder-containing sodium bicarbonate to prevent their activation by acid in the stomach.
- Esomeprazole, pantoprazole and lansoprazole have higher oral bioavailability than omeprazole. Parenteral (i.v.) formulations are available for esomeprazole, lansoprazole, pantoprazole and rabeprazole. They are highly bound to plasma proteins; extensively metabolized in the liver and their metabolites are excreted in the urine.
- Therapeutic uses
- Peptic ulcer: PPIs are the most powerful acid-suppressive agents. They inhibit all phases of gastric acid secretion. PPIs are superior to H2-blockers, as their onset of action is rapid and causes faster ulcer healing. The standard dose of omeprazole is 20 mg, lansoprazole is 30 mg and pantoprazole is 40 mg once daily. Duodenal ulcers require 4-week therapy and gastric ulcers require 6- to 8-week therapy for healing.
- In acute bleeding ulcers, intravenous PPIs are preferred. By suppressing acid secretion, they promote the healing of ulcers.
- H. pylori-associated ulcers: Combination therapy of two or three antimicrobials and a PPI is the most effective regimen for these ulcers.
- Stress ulcers: Prophylactic use of intravenous PPIs reduces the incidence of stress ulcers in critically ill patients.
- NSAID-induced ulcers: PPIs are more effective than H2-blockers for the prevention and treatment of NSAID-induced ulcers.
- PPIs can be used preoperatively to reduce the risk of aspiration pneumonia.
- Gastroesophageal reflux disease GERD: In GERD, the goal of therapy is to produce symptom relief, heal erosive oesophagitis and prevent complications.
- PPIs are the preferred agents for the treatment of GERD and are usually given once daily. They are more effective than H2-blockers. Patients with erosive oesophagitis or peptic ulcer with stricture need prolonged maintenance therapy with PPIs.
- Zollinger–Ellison syndrome (Z–E syndrome): Z–E syndrome is characterized by hypergastrinaemia with multiple peptic ulcers. PPIs are the preferred agents for Z–E syndrome. Higher doses of PPIs are needed for healing of ulcers. Surgery is the definitive treatment. In inoperable cases, prolonged therapy with PPIs has been recommended.
- Peptic ulcer: PPIs are the most powerful acid-suppressive agents. They inhibit all phases of gastric acid secretion. PPIs are superior to H2-blockers, as their onset of action is rapid and causes faster ulcer healing. The standard dose of omeprazole is 20 mg, lansoprazole is 30 mg and pantoprazole is 40 mg once daily. Duodenal ulcers require 4-week therapy and gastric ulcers require 6- to 8-week therapy for healing.
- Adverse effects of PPIs are generally well tolerated. The side effects are headache, nausea, diarrhoea and abdominal pain. Skin rashes and arthralgia can rarely occur. Long-term use of PPIs can decrease vitamin B12 absorption, increase the risk of infections (for example hospital-acquired pneumonia) and osteoporosis. Chronic use also results in hypergastrinaemia which may predispose to gastric tumours.
- Drug interactions
- Omeprazole can inhibit the metabolism of drugs like phenytoin, warfarin and diazepam.
- PPIs decrease the bioavailability of itraconazole, iron salts, etc. Drug interactions are minimal with pantoprazole.
- Mechanism of action of proton pump inhibitors.
- H2-receptor antagonists (H2-blockers)
- Mechanism of action H2-receptor antagonists competitively block H2-receptors on parietal cells and inhibit gastric acid production. They suppress all phases (basal, cephalic and gastric) of acid secretion. They are mainly effective in suppressing nocturnal acid secretion. H2-blockers also reduce acid secretion stimulated by ACh, gastrin, food, etc. They are less potent than PPIs – 24 h acid secretion is suppressed by 60%–70%. Cimetidine is the prototype drug and was the first H2-blocker to be used in clinical practice. It is seldom used now because of its adverse effects.
- Comparison of Cimetidine and Ranitidine
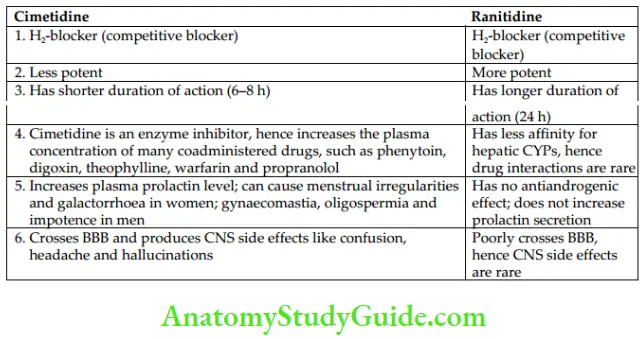 H2-blockers is usually administered orally and are well absorbed; metabolized in the liver and the metabolites are excreted in the urine. Cimetidine, ranitidine and famotidine are also available for intravenous administration.
H2-blockers is usually administered orally and are well absorbed; metabolized in the liver and the metabolites are excreted in the urine. Cimetidine, ranitidine and famotidine are also available for intravenous administration. - Famotidine: Most of the features are similar to ranitidine. It is more potent and longer-acting than ranitidine. It has no antiandrogenic effect. Drug interactions with famotidine are negligible.
- Comparison of Cimetidine and Ranitidine
- Therapeutic uses
- Peptic ulcer: H2-blockers are one of the most commonly used drugs in peptic ulcers. H2-blockers produce symptomatic relief within days and ulcer healing within weeks. The duration of treatment for duodenal ulcers is 4–6 weeks. Gastric ulcer requires prolonged therapy for 6–8 weeks. However, PPIs are more frequently used because they have higher efficacy and are well tolerated.
- H. pylori-associated ulcers: H2-blockers can be used along with antimicrobial agents to treat H. pylori infection.
- Stress ulcers are commonly seen in critically ill patients with severe medical or surgical illness. They may be associated with upper gastrointestinal bleeding. Intravenous H2-blockers are used to prevent and treat stress-related ulcers and bleeding.
- NSAID-induced ulcers: H2-blockers can be used for healing NSAID-induced ulcers, but they are less effective than PPIs.
- Z–E syndrome: In Z–E syndrome, surgery is the definitive therapy. PPIs or H2– blockers are used to control the hypersecretion of acid. PPIs are the preferred agents in Z–E syndrome.
- GERD: In GERD, H2-blockers are effective and produce symptomatic relief. PPIs are more effective than H2-blockers.
- H2-blockers are used preoperatively to reduce the risk of aspiration pneumonia.
- Peptic ulcer: H2-blockers are one of the most commonly used drugs in peptic ulcers. H2-blockers produce symptomatic relief within days and ulcer healing within weeks. The duration of treatment for duodenal ulcers is 4–6 weeks. Gastric ulcer requires prolonged therapy for 6–8 weeks. However, PPIs are more frequently used because they have higher efficacy and are well tolerated.
- Mechanism of action H2-receptor antagonists competitively block H2-receptors on parietal cells and inhibit gastric acid production. They suppress all phases (basal, cephalic and gastric) of acid secretion. They are mainly effective in suppressing nocturnal acid secretion. H2-blockers also reduce acid secretion stimulated by ACh, gastrin, food, etc. They are less potent than PPIs – 24 h acid secretion is suppressed by 60%–70%. Cimetidine is the prototype drug and was the first H2-blocker to be used in clinical practice. It is seldom used now because of its adverse effects.
- Anticholinergic agents Pirenzepine and telenzepine, selective M1-receptor blockers, inhibit acid secretion. They are not commonly used because of their low efficacy and anticholinergic side effects.
- Prostaglandin analogues Misoprostol, a synthetic PG analogue (PGE1), is effective orally for the prevention and treatment of NSAID-induced gastric and duodenal ulcers. Prostaglandins inhibit gastric acid secretion, and increase mucus and bicarbonate secretion; they also increase mucosal blood flow (cytoprotective effect). The common side effects are diarrhoea and abdominal cramps. Misoprostol is contraindicated in pregnancy, as it may cause uterine contractions. Because of its adverse effects and need for frequent dosing, it is rarely used.
Ulcer protectives
- Sucralfate is a complex of aluminium hydroxide and sulfated sucrose. In the acidic environment of the stomach (pH <4), sucralfate undergoes polymerization to form a sticky gel that adheres to the ulcer base and protects it.
- It also precipitates proteins at the ulcer base – and forms a barrier against acid, and pepsin. It stimulates the release of PGs and epidermal growth factor locally, thus producing a cytoprotective effect. It also increases mucus and bicarbonate secretion – and enhances mucosal defence and repair.
- Sucralfate is given orally on an empty stomach at least 1 h before meals. It reduces the absorption of drugs such as digoxin, tetracyclines, ketoconazole and fluoroquinolones. Since it requires pH <4 for activation, concurrent administration of antacids, H2-blockers or PPIs should be avoided. Constipation is a common side effect. Nausea may occur.
- Aluminium toxicity can occur in patients with renal failure. After the introduction of PPIs, sucralfate is seldom used in peptic ulcers. Sucralfate is effective for the prevention of bleeding from stress ulcers and to reduce the risk of aspiration pneumonia. It is also useful in GERD with oesophagitis, as it is a mucosal protector. Other uses are oral mucositis, radiation proctitis, rectal ulcers, burns, bed sores, etc.
- Bismuth-containing preparations Colloidal bismuth subcitrate (CBS) is an oral bismuth preparation. The mode of action is not clear. It probably:
- Reacts with protein in the base of the ulcer and protects it from peptic digestion.
- Stimulates the secretion of PGE2, mucus and bicarbonate.
- Has antimicrobial effect against H. pylori.
It is one of the components in certain anti–H. pylori regimens. The side effects are blackening of the tongue and stools.
Drugs That Neutralize Gastric Acid (Antacids)
Antacids are weak bases that neutralize gastric acid and thus raise the gastric pH. They do not affect acid production. Acid neutralizing capacity reflects the potency of an antacid.
- An ideal antacid:
- should be insoluble and capable of neutralizing acid.
- should not liberate CO2.
- should be nonabsorbable.
- should not disturb the acid-base balance of the body.
- Types of antacids
- Nonsystemic: Magnesium hydroxide, magnesium trisilicate, aluminium hydroxide gel and calcium carbonate.
- Systemic: Sodium bicarbonate and sodium citrate.
- Nonsystemic antacids Magnesium hydroxide, magnesium trisilicate, aluminium hydroxide, calcium carbonate, etc. form respective chloride salts in the stomach. When this reaches the intestine, the chloride salt reacts with bicarbonate, so HCO3– is not available for absorption, hence there is no systemic alkalosis. The combination of antacids produces various beneficial effects. They are:
- Aluminium salts cause constipation and magnesium salts cause diarrhoea; so the combination of these two can counteract the adverse effects of each other.
- Magnesium hydroxide has a rapid onset of action, but aluminium hydroxide acts slowly – the combined product produces a rapid and sustained effect.
- The dose of individual antacids is reduced, hence systemic toxicity is minimized. Calcium may be absorbed from its salts resulting in hypercalcaemia and hypercalciuria.
- Systemic antacids
- Sodium bicarbonate (NaHCO3): It rapidly neutralizes gastric acid, but the duration of action is short. The disadvantages of NaHCO3 are that:
- it is highly water soluble and rapidly absorbed from the gut;
- it releases CO2 that can cause abdominal distension and belching;
- it may cause metabolic alkalosis; and
- it produces rebound acidity.
- Sodium bicarbonate is also used to alkalinize urine and to treat acidosis. It should be avoided in patients with hypertension and congestive cardiac failure, as it causes sodium retention.
- Formulations: Antacids are available as suspension, tablet and powder. Tablet should be chewed and swallowed for better effect. Suspensions have better neutralizing capacity than other formulations.
- Adverse effects of antacids
- Sodium bicarbonate can cause systemic alkalosis and sodium overload.
- Magnesium hydroxide may produce diarrhoea.
- Aluminium hydroxide may produce constipation and phosphate depletion.
- Calcium carbonate may produce hypercalcaemia and hypercalciuria.
- Acid rebound can occur.
- Drug interactions All antacids increase the pH of the stomach and form insoluble and nonabsorbable complexes with many drugs – iron, tetracyclines, fluoroquinolones, ketoconazole, etc., thus, antacids reduce the absorption of these drugs. There should be a gap of 2 hours between the administration of these drugs and antacids.
- Sodium bicarbonate (NaHCO3): It rapidly neutralizes gastric acid, but the duration of action is short. The disadvantages of NaHCO3 are that:
Antifoaming Agents
- Methylpolysiloxane (simethicone and dimethicone): They are antifoaming agents, usually present in some antacid preparations. They decrease foaming and relieve flatulence.
- Oxethazaine: It is a topical anaesthetic and is used to anaesthetize gastric mucosa. It produces symptomatic relief in gastritis and GERD. It is available in combination with antacids.
- Sodium alginate: It forms froth on the contents in the stomach – and prevents the effects of gastroesophageal reflux.
Anti–H. Pylori Agents
Helicobacter pylori, a gram-negative, rod-shaped bacteria, is associated with gastritis, duodenal ulcer, gastric ulcer and gastric carcinoma.
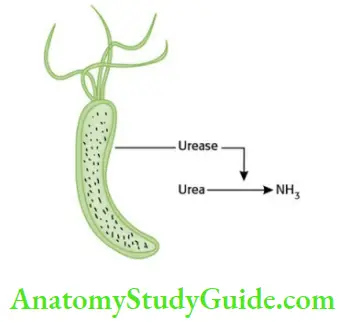
The mechanism by which H. pylori causes mucosal inflammation and damage is not clear. The ammonia produced by urease activity may directly damage the cells.
Many regimens are available for the eradication of H. pylori. Combination therapy (triple/quadruple) is always recommended. The objectives of combination therapy are:
- To prevent or delay the development of resistant organisms.
- To prevent relapse.
- To promote rapid ulcer healing.
- To eradicate H. pylori infection.
The duration of treatment could be for 1 or 2 weeks, of which 2-week therapy is more effective.
The antimicrobials used in H. pylori infection are amoxicillin, tetracycline, clarithromycin, metronidazole and tinidazole. Resistance develops rapidly to metronidazole and clarithromycin, but not to amoxicillin. Amoxicillin should be avoided in patients with a history of penicillin allergy.
Other anti–H. pylori drugs are PPIs, H2-blockers and CBS. A combination of three drugs (triple therapy) or four drugs (quadruple therapy) can be used. A commonly used triple-therapy regimen is as follows:
- Triple therapy × 1 4 days (2 weeks)
-
- Lansoprazole 30 mg BD +
- Clarithromycin 500 mg BD +
- Amoxicillin 1 g BD
After completion of the above regimen, PPI should be continued for 6 more weeks to enhance ulcer healing.
- Drugs useful in gastroesophageal reflux disease (GERD)
-
- PPIs and H2 receptor blockers – they decrease acid secretion → pH of gastric contents rise → Relief of symptoms and healing of oesophageal lesions. PPIs are more effective than H2– blockers. They do not affect LES tone.
- Antacids are used occasionally in GERD. They are rapid-acting.
- Prokinetic drugs, for example, metoclopramide, cisapride, and mosapride increase the tone of LES, and enhance gastric emptying but do not affect acid secretion.
Leave a Reply