Physical Factors In Retention Of Complete Dentures
Denture retention with a note on physical factors.
Answer:
Retention is defined as, “That quality inherent in the prosthesis which resists the force of gravity, adhesiveness of foods and the forces associated with the opening of the jaws.”–GPT It is the ability of the denture to resist displacement against its path of insertion.
Physical factors
- Adhesion.
- Cohesion.
- Interfacial surface tension.
- Capillarity or capillary attraction.
- Atmospheric pressure and peripheral seal.
Read And Learn More: Complete Dentures Question and Answers
1. Adhesion
Adhesion is defined as “The physical attraction of, unlike molecules to one another.” –GPT
Physical factors Factors Affecting Adhesion
- A thin film of saliva is essential in wetting the tissue surface of the denture and the mucosa. Thick ropy saliva displaces the denture by hydraulic pressure.
- The amount of adhesion is proportional to the denture base area coverage. Some denture base materials help in wetting and have better retention by adhesion.
2. Physical factors Factors Affecting Cohesion
Cohesion is defined as, “The physical attraction of like molecules for each other”. The factors that affect adhesion also affect cohesion. The cohesive forces act within the thin film of saliva. The greater the denture-bearing area, the more effective cohesion.
3. Physical factors Factors Affecting Interfacial surface tension
It is defined as, “The tension or resistance to separation possessed by the film of liquid between two well-adapted surfaces.” –GPT These forces are found within the thin film of saliva, separating the denture base from the tissues which in turn resists the displacing forces. This force is dependent on the presence of air at the margins of liquid and solid contact (liquid-air interface).
Physical factors Factors Affecting Interfacial Surface Tension
- Consistency of Saliva (should be thin and even).
- The perfect fit of the denture base.
- Maximum coverage of basal seat area.
- Good adhesive and cohesive forces, which aid to enhance interfacial surface tension.
4. Capillary attraction
It is defined as “That quality or state because of surface tension causes elevation or depression of the surface of a liquid that is in contact with a solid.”–GPT
Capillary attraction is a phenomenon in which a liquid tends to rise in a capillary tube by maximizing its contact along the walls of the tube at the interface between the liquid and glass.
Factors Affecting Capillary Attraction
- Good adaptation of denture base to soft tissue with maximum coverage.
- A thin film of saliva.
- When there is a close adaptation between the denture and the mucosa.
5. Atmospheric pressure and peripheral seal
- A peripheral seal is the area of contact between the peripheral borders of the denture and the resilient-limiting structures. The peripheral seal prevents air entry between the denture and the soft tissue.
- When displacing forces act on the denture, a partial vacuum (natural suction) is produced between the denture and the soft tissues, which aids in retention.
- Hence, atmospheric pressure is referred to as emergency retentive force or temporary restraining force.
Factors Affecting Atmospheric Pressure
- Good peripheral seal.
- The perfect fit of the denture.
- Maximum coverage of basal seat.
Vibrating line.
Answer:
- The vibrating line of the palate is an imaginary line drawn across the palate that marks the beginning of motion of the vibrating in the soft palate when the patient says “ah”.
- The submucosa in the region of the vibrating line on the soft palate contains glandular tissue. The submucosa of the mucous membrane contained within the hamular notch is thick and made up of loose areolar tissue.
The vibrating line is Divided as:
- Anterior vibrating line.
- Posterior vibrating line.
Vibrating line Anterior Vibrating Line
- The anterior vibrating line is an imaginary line located at the junction of the attached tissues overlying the hard palate and the movable tissues of the immediately adjacent soft palate. The anterior vibrating line is always on soft palatal tissues.
- Locating anterior vibrating line This is to have the patient do the Valsalva maneuver, in which both nostrils are held firmly while the patient blows gently through the nose. Another method is to instruct the patient to say “ah” with short vigorous bursts.
- Due to the projection of the posterior nasal spine, the anterior vibrating line is not a straight line between both hamular processes.
Vibrating line Posterior Librating Line
- The posterior vibrating line is an imaginary line at the junction of the aponeurosis of the tensor veli palatine muscle and the muscular portion of the soft palate.
- It demarcates between that part of the soft palate that has limited or shallow movement during function and the remainder of the soft palate that is displaced during functional movements.
- Locating posterior vibrating line: The posterior vibrating line is visualized by instructing the patient to say “ah” in short bursts in a normal, unexaggerated fashion. The posterior vibrating line marks the most distal extension of the denture base.
Vibrating line Extent
- It extends from one pterygomaxillary notch to the other and is about 2 mm in front of the foveae palatine. The direction of the vibrating line depends on the shape of the palate.
- In a mouth with a flat vault, the vibrating line is usually farther posterior with a gradual curvature, having a broad posterior palatal seal area.
- The distal end of the upper denture should end 1 or 2 mm posterior to the vibrating line and cover the tuberosities and extend into the hamular notches.
Vibrating line Posterior palatal seal area
The posterior palatal seal area lies between the anterior and posterior vibrating lines and is cupids bow-shaped. This area in the denture should adapt closely to the PPS for improved retention.
Fluid wax technique.
Answer:
The fluid wax technique is one of the techniques that utilize waxes that flow at mouth temperatures to record the posterior palatal seal area.
Fluid wax technique Waxes used are.
- Lowa wax ( white) was developed by Dr. Earl S. Smith
- Korecta wax No. 4 (orange) developed by Dr. O. C. Applegate
- H-L physiologic paste (yellow-white) developed by Dr. C. S. Harkins
- Adaptol (green) was developed by Nathan G. Kaye.
Fluid wax technique Procedure
- After identifying the posterior palatal seal area in the mouth, the transfer markings are copied onto the final impression.
- Any one of the four types of wax is selected depending on the dentist’s choice and is painted onto the impression surface within the outline of the seal area after melting.
- After the wax is painted in the PPS region, the tray is reseated in the mouth and held in place under gentle pressure for four to six minutes.
- A 30° flexion of the patient’s head along with the tongue that is firmly positioned against the mandibular anterior teeth (handle) helps in molding the PPS region.
- The patient is asked to periodically rotate the head so that all functional positions of the soft palate are recorded.
- The tray is removed from the mouth and if the wax has a glossy appearance the tissue contact is proper, if not, the procedure should be repeated.
- The secondary impression is reinserted and held for three to five minutes under gentle pressure, followed by two to three minutes of firm pressure applied to the mid-palatal area of the impression tray. During this time, the head and tongue positions must be maintained.
Fluid wax technique Advantages
- It is a physiologic technique displacing tissues within their physiologically acceptable limits.
- Over-compression of tissues is avoided.
- A posterior palatal seal is incorporated into the trial denture base for added retention.
- Mechanical scraping of the cast is avoided.
Fluid wax technique Disadvantages
- More time is necessary during the impression appointment.
- Difficulty in handling the materials and added care during the boxing procedure.
Fluid wax technique for adding a posterior palatal seal to an already existing denture (Moghadam and Scandrett)
- The locating, marking, and placing of the wax in the seal area are the same.
- After the wax has flown adequately, the denture is removed from the mouth and the anterior extent of the seal is marked on the denture.
- Utility wax is placed vertically across the palate, separating the posterior two-thirds from the anterior region and extending around the posterior portion of the denture.
- The dental stone is vibrated into the denture-wax surface outlined by the utility wax.
- After the stone has set, the wax is eliminated, the denture cleaned and the area distal to the anterior vibrating line is ground.
- After applying lubricant to the unground areas, including the polished surface, a separating medium is applied to the stone cast, and the denture is replaced on the stone cast and held firmly with rubber bands.
- Acrylic is added till the space between the denture and cast is filled. After waiting till the initial set has taken place, it is placed in a pressure pot with water (140°F) for 20 minutes under 30 psi pressure.
- The cast and denture are separated, the excess acrylic is trimmed, and the border is polished lightly.
- Light-cured resin can be used instead of acrylic resin.
Relevance of pps.
Answer:
The posterior palatal seal (PPS) is defined as, “The soft tissues along the junction of the hard and soft palates on which pressure within the physiologic limits of the tissues can be applied by a denture to aid in the retention of the denture.” –GPT
Relevance of pps Importance of apps
- A positive contact is established posteriorly thereby preventing the final impression material from sliding down the pharynx.
- For positioning the impression tray, accurately.
- To create slight displacement of the soft palate.
- To determine if adequate retention and seal can be achieved in the potential denture border.
- Adequate border seals resist horizontal forces and lateral torquing of the maxillary denture.
- The function of the posterior palatal seal in the completed maxillary prosthesis is to maintain
contact with the anterior portion of the soft palate during functional movements such as mastication, deglutition, and phonation. - To aid the denture to achieve better retention.
- The posterior palatal seal will reduce patient awareness of the border of the denture hence reducing the gag reflex.
Functions of bite blocks/occlusal rims.
Answer:
- Helps to orient the occlusal plane.
- Gives facial support.
- Aids inaccurate location of the midline of the arch.
- Helps in positioning the incisors and cuspids.
- Aids in locating the smile line (high lip line) and the speaking (low) lip line.
- To establish accurate maxillomandibular jaw relations.
- For arranging the artificial teeth to form the trial denture.
- Helps to determine the length and width of the artificial teeth.
Functions of bite blocks/occlusal rims Four factors in the fabrication of occlusion rims
- Relationship of the natural teeth to the alveolar bone.
- Relationship of occlusion rim to the edentulous ridge.
- Fabrication technique.
- Clinical guidelines.
Functions of bite blocks/occlusal rims Relationship of the natural teeth to the alveolar bone and occlusal rim to the ridge
- The natural maxillary anterior teeth are slightly forward of the alveolar bone and support the
upper lip. - The incisal edge of the incisor teeth approximates the lower edge of the lip.
- The mandibular incisors are inclined forward and tend to support the lower lip. The incisal edge is approximately 1 to 2 mm behind the lingual surface of the maxillary incisors.
- The maxillary posterior teeth are positioned slightly buccal to the alveolar ridge and. the maxillary buccal cusps project 2 to 3 mm beyond the buccal cusps of the mandibular teeth.
Functions of bite blocks/occlusal rims Fabrication technique
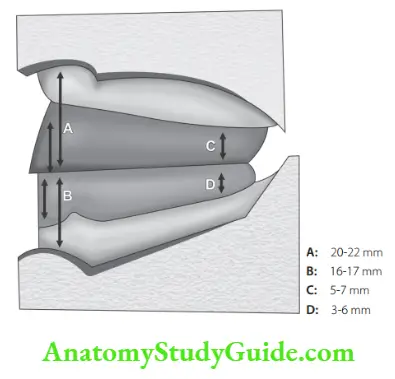
- Maxillary height anterior region: 22 mm from the sulcus depth.
- Maxillary posterior height: 18 mm (length of the first maxillary molar crown).
- Mandibular anterior height: approximately 16 to 18 mm.
- Mandibular posterior height: a point representing one-half the height of the retromolar pad.
- Width anteriorly for both rims: 3 to 5 mm wide.
- Width in the posterior region: 8 to 10 mm.
Functions of bite blocks/occlusal rims Clinical Guidelines
- Maxillary rim: Anteriorly parallel to the interpupillary line and occlusal rim should be 2 mm visible. Posteriorly the upper rim is one-quarter inch below Stensen’s duct. The plane of occlusion is made parallel to the ala-tragal line projected from the ala of the nose to the superior edge of the tragus of the ear (Camper’s line).
- Apart from the above factors as facial support, the length and width of the anterior teeth, the cuspid eminences, the smiling line, and the speaking (low) lip line.
- Mandibular rim: Anteriorly should be at the level of the lower lip and posteriorly one-half the height of the retromolar pad. From cuspid to cuspid, the rim is inclined slightly forward but remains within the border of the recording base. Posterior to the cuspid area, the rims should be located over the center of the crest of the ridge.
The final forming of the anterior portion of the maxillary occlusion rim is determined by the:
- Nasolabial sulcus
- Mentolabial sulcus
- Philtrum
- Commissure (corner) of the mouth.
Functions of bite blocks/occlusal rims Nasolabial sulcus and mento labial sulcus
- When proper lip support is not given there is a deepening of the nasolabial and mentolabial sulci with loss of definition in the philtrum and a drooping of the corners of the mouth.
- If occlusal rims are over contoured the nasolabial and mentolabial folds and philtrum become shallow producing a “stretched look”.
Occlusal plane.
Answer:
Occlusal plane Procedure in adjusting the maxillary occlusal plane
- Anteriorly the maxillary rim is reduced 1 to 2 mm below the lower edge of the lip “low lip line” and should be parallel to the interpupillary line.
- Posteriorly the height in the first molar area is reduced by about one-quarter inch below Stensen’s duct.
- The plane of occlusion is made parallel to the ala–tragal line (the ala of the nose to the superior edge of the tragus of the ear- Camper’s line). When the occlusal plane is parallel to the ala-tragus line the closing force during clenching was greater than when it was altered plus or minus 5°.
- The cuspid eminences are marked corresponding to lines placed at the corners of the mouth. These lines represent the location of the distal surface of the cuspid teeth.
- From the occlusal view, the occlusion rim is sloped slightly inward to create space, for buccal corridor, between the teeth and the cheeks.
Occlusal plane Mandibular Occlusal Plane
Occlusal plane Anteriorly
- The occlusal plane is determined by the lower anterior teeth and the commissure of the mouth.
- From cuspid to cuspid, the rim is inclined slightly forward remaining within the border of the recording base. Posterior to the cuspid area, the rims should be located over the center of the crest of the ridge.
- The occlusal rim should terminate posteriorly at the junction of the anterior one-third and posterior two-thirds of the retromolar pad. These landmarks orient the occlusal plane at the correct anteroposterior inclination which is nearly parallel to the lower foundation plane.
- The parotid papilla was on average 3.3 mm above the occlusal plane and it can be used as a guide for establishing the height of the occlusal plane.
- If it is too high, the upper and lower posterior teeth can bite the papilla during function. If the occlusal plane is too low, then the tongue can overlap the lower teeth and cause tongue biting.
Occlusal plane Buccally
The teeth should not displace the buccal mucosa but make passive contact with it so that the buccinator muscle will not forcibly move the lower denture by its action against the buccal surfaces of the teeth.
Occlusal plane Lingually
The lower posterior teeth should not crowd the tongue or interfere with its normal function. The lingual cusps of the natural molars are approximately in vertical alignment with the mylohyoid ridge.
Occlusal plane Tongue Position
- At rest, after swallowing, the tip of the tongue touches the lingual surfaces of the lower anterior teeth.
- The lateral border of the tongue will be at the level of the lingual contour of the lower natural posterior teeth.
- The dorsal surface of the tongue is nearly level with the occlusal surfaces of the posterior teeth.
Atmospheric pressure.
Answer:
Atmospheric pressure Introduction
- Stanitz (1945) states that there are differences in pressure between the atmosphere and the fluid film.
- Landa states that atmospheric pressure aids in the retention of dentures.
- Oehl and Dresen acknowledged that atmospheric pressure acts only if the peripheral seal is correctly formed.
- Snyder showed that reduced atmospheric pressure decreased denture retention in a decompression chamber.
- Skinner and co-workers (1953) say that “atmospheric pressure is an ordinary ‘suction’ and vacuum chamber does not have much influence on retention.”
- Page and Moses consider atmospheric pressure to be of no importance in retention. Only interfacial surface tension helps in retention.
Atmospheric pressure and peripheral seal
- The peripheral seal is the area of contact between the peripheral borders of the denture and the resilient-limiting structures. The peripheral seal prevents air entry between the denture and the soft tissue.
- When displacing forces act on the denture, a partial vacuum (natural suction) is produced between the denture and the soft tissues, which aids in retention.
- Hence, atmospheric pressure is referred to as emergency–retentive force or temporary restraining force.
Atmospheric pressure Factors affecting atmospheric pressure
- Good peripheral seal.
- The perfect fit of a denture.
- Maximum coverage of basal seat.
- Balanced occlusion.
- The shape of the polished surfaces.
Cast metal bases/Metal denture bases.
Answer:
Metal denture bases Requirements for Cast Metal Bases
- Metal bases should be thin but rigid.
- Dense.
- Accurate, having a positive fit on the master cast without rocking.
- Biologically acceptable alloy.
Metal denture bases Advantages of Metal Bases Over Resin Bases (By Faber)
- Prevention of acrylic warpage.
- Lack of bulk with more strength.
- Increased accuracy.
- Less tissue change under the base.
- Less porosity and therefore easier to clean and keep clean.
- Thermal conductivity.
- Less deformation in function.
Metal denture bases Disadvantages
- High cost.
- Greater weight.
- Inability to be easily rebased.
- Poor esthetic qualities.
- Time-consuming construction.
Metal denture bases Materials for Cast Metal Bases
- Gold alloys Types 3 and 4
- They contain copper, silver, palladium, platinum, and some trace elements.
- Chrome base alloys
- All the cast chrome alloys for RPD can be used, e.g. Ticonium, Vitalium, and Nobelium, etc.
- Aluminum alloys
- Pure aluminum with 29c to 4% magnesium and slight amounts of silicon is more common. The casting temperature of aluminum is between 704. 5° to 815. 5° C.
- Anodized aluminum
Metal denture bases Design Principles
A pencil drawing indicating the amount of coverage, placement of finishing lines, and type of resin retention on the master cast is used.
Metal denture bases Maxillary Bases
The appropriate design covers the complete palate and ridge crest but leaves the denture borders in resin. Covering the posterior palatal seal area in metal is also permitted and the resin periphery begins at the pterygomaxillary notch area.
Metal denture bases Mandibular Bases
The mandibular cast base covers the crest of the ridge with resin peripheries. This is preferred as easier to adjust and polish, though complete coverage of the metal base can also be done.
Metal denture bases Resin Retention
- Retention mesh,
- Non-relieved retention of beads,
- Nailheads, and
- Loops.
Metal denture bases Block out and relief
Soft-tissue undercuts under the bases need to be blocked out and the placement of arbitrary relief areas is to be given. This block-out reduces the number of sharp metal projections on the tissue surface to be removed during finishing.
Metal denture bases Casting Procedure
- Vitalium and Nobelium need higher temperature burnout, 982° to 1093°C. Cast all chrome base alloys in automatic induction casting machines.
- For Aluminum 343.5 °C place the aluminum ingots in the induction crucible of the Electromatic Casting Machine. Use this crucible for aluminum only. Turn on the melt switch and probe the ingots with a quartz rod as they melt. When it is possible to push the top ingots into the mass, turn off the melt switch and allow the metal to cool.
- Remove the mold from the furnace and place it in the cradle. Turn on the melt switch and watch the metal until it takes on the orange color of a harvest moon. At that point, throw the automatic cast switch and complete the casting. Keep the arm rotating for a full 3 minutes.
- Remove the cast and allow it to bench cool for 10 minutes before quenching it in running water. Remove the bulk of the refractory material with a wax spatula or a similar hand
instrument under running water. Do the final cleansing of the refractory cast by blasting it carefully with walnut-shell abrasives. Do not use a sandblaster because it will pit and dull the aluminum alloy. - As the aluminum alloy is soft, considerable care in fitting and finishing the casting is needed. The rest of the finishing is done with a slow-speed lathe or with a laboratory handpiece, finishing stones, and burs.
Face-bow uses and types.
Answer:
The face-bow is a caliper-like device used to record the relationship of the maxillae to the temporomandibular joints and to orient the maxillary cast to the articulator in the same relationship that exists between the maxillae and the opening and closing axis in the temporomandibular joints.
Face-bow uses and types Uses of face-bow
- It supports the casts while they are attached to the articulator.
- When cusp-form teeth are used.
- When balanced occlusion in the eccentric positions is desired.
- When a definite cusp fossa or cusp tip-to-cusp incline relation is needed.
- Interocclusal check records after face-bow transfer aid in verifying of jaw positions.
- If the occlusal vertical dimension is changed and the alterations of tooth occlusal surfaces are necessary to accommodate the change.
Face-bow uses and types Types of Face-bow
Face-bow uses and types Arbitrary: Has two types: Earpiece face-bow and Facia type of face-bow. Kinematic or hinge-bow.
Face-bow uses and types Arbitrary
- The arbitrary face-bow is placed on the face with the condyle rods located approximately over the condyles.
- Used in complete denture patients.
- The condyle rods are positioned on a line extending from the outer canthus to the top of the tragus and 13 mm in front of the external auditory meatus locating the rods within 5 mm of the true center of the opening axis of the jaws. (Facia type) Hanau Model C. Without clamping the condyle rods, the dentist centers the device so equal readings are obtained on both sidebands, and the wing nut of the clamp is tightened to hold the face-bow in place on the occlusal fork.
- The rods of another are designed to fit into the external auditory meatuses. (Earpiece type, Whip Mix).
- The fork of the arbitrary face-bow is attached to the maxillary occlusion rim. The transverse axis of the articulator is 5/8 inch (15 mm anterior to the position of the ends of the face-bow).
- This distance compensates for the distance between the external auditory meatus and the condyle.
Face-bow uses and types Kinematic face-bow
- The kinematic face-bow is so designed that the opening axis of the mandible can be located more accurately.
- The fork of kinematic face-bows is attached to the mandibular occlusion rim.
- As the patient protrudes the mandible and opens and closes the jaws, the movement of the points of the condyle rods is observed.
- As the condyle rods of kinematic face-bows have sharp points, their motion can be observed more accurately.
- When the points rotate only and do not translate, they are on the opening axis of the jaw.
- At this position, the mandible is in centric relation to the occlusal vertical dimension that has been established. After the hinge axis center is located it is marked on the face with an indelible pencil.
- The face-bow is removed from the face-bow fork and the condyle rods are straightened and made parallel. The face bow is now used in a regular manner by being fastened into place over the previously determined rotational points.
- This type of transfer will be exact in the positional relation of the cast and will permit a recording medium such as wax, zinc oxide-eugenol, or plaster for interocclusal records without usual inaccuracy being produced. This is important when the interarch distance is to be increased or decreased.
- Kinematic face-bow can aid in recording centric relations. The difficulty of attaching the lower occlusion rim to an edentulous mandible and movement of the recording base on the jaw makes determining the exact center of the opening axis difficult hence preventing its use for edentulous patients.
- Aids in finding the appropriate vertical dimension clinically and does not change in the articulator.
Interocclusal distance (freeway space).
Answer:
Interocclusal distance Definition
The interocclusal distance (formerly referred to as the “free way space”) is the distance or gap existing between the occluding surfaces of maxillary and mandibular teeth when the mandible is in the physiologic rest position.
- The difference between the occlusal vertical dimension and the rest vertical dimension is the interocclusal distance.
The interocclusal distance is 2 to 4 mm when observed at the position of the first premolars. - It was observed that the clinically recorded rest position and the electromyographically determined one have a range of 10 mm.
Interocclusal distance Significance
- In natural dentition, it is essential to maintain the health of the periodontal tissues.
- In complete denture patients failure to provide interocclusal distance will cause “clicking” of the dentures during speech, soreness of the tissues of the basal seat, and rapid destruction of the residual alveolar ridges.
- Interocclusal distance is important to record the correct vertical dimension of occlusion.
Interocclusal Distance Problems with reduced Interocclusal space
- Esthetics: The chin appears too close to the nose and too far forward. The lips lose their fullness and the vermilion borders are reduced to approximate a line. The corners of the mouth turn down.
- Muscular action: Decreases the action of the muscles, with a resultant loss of muscle tone.
- Causes a crease to form at the corners of the mouth associated with angular cheilitis.
- Leads to a loss of the cubicle space of the oral cavity.
- Pushes the tongue toward the throat. Displacing and encroaching adjacent tissues causes obstruction to the opening of the eustachian tubes interfering with ear function.
- Trauma in the region of the TMJ fossa as obscure pain, discomfort, clicking sounds, headaches, and neuralgia.
- Excessive bone resorption: If adequate interocclusal distance is not provided it produces excessive interarch distance when the teeth are in occlusion. Hence the muscles will continue to exert force to overcome this obstacle and as a result, the supporting tissues will be resorbed until the proper distance is returned.
- Clicking of dentures: The premature contact of the teeth results in a clicking noise.
- Function: Proper functioning with the denture as chewing, Phonetics, and swallowing are difficult.
Interocclusal distance Methods of establishing Interocclusal space
- Facial measurements
- Instruct the patient to stand or sit comfortably upright with the eyes looking straight ahead. Insert the maxillary record base with the attached contoured occlusion rim.
- With either an indelible marker or a triangle of adhesive tape, place a point of reference on the end of the patient’s nose and another on the point of the chin. Instruct the patient to wipe the lips with the tongue to swallow and to drop the shoulders.
- When the mandible drops to rest position and then measure between the points with a millimeter ruler. Repeat the procedure until the measurements are consistent.
- Tactile sense
- Then ask them to close slowly until the jaws reach a comfortable, relaxed position. The distance is measured between the points of reference and compared with the measurements made after swallowing.
- Phonetics
- Have patients repeat “M” until they are aware of the contact of the lips as “M” is pronounced. Repeat this procedure and ask that they stop all jaw movement when the lips touch.
- At this time measure between two points of reference. An adequate interocclusal distance is needed for the proper functioning of the denture as well as the preservation of supporting tissues and the health of the patient.
Enumerate and describe various physical factors of retention in complete denture prostheses.
Factors That Enhance The Retention, Stability, And Support Of A Denture:
- Maximum coverage of the basal seat within the limits of the health and functions of the supporting and limiting tissues.
- Borders that are in harmony with the anatomic and physiologic limitations of the oral structures.
- A physiologic type of border-molding procedure.
- Proper space is ensured in the tray for final impression material.
- Selective pressure technique for the final impression.
- Ideal impression material to be used depending on the clinical situation.
- A guiding mechanism for correct positioning of the impression tray in the mouth.
- The tray and final impression should be of dimensionally stable materials.
- The completed final impression form is similar to the external form of the completed denture.
- Accurately fitting final impression tray.
Factors Affecting Retention Of Dentures:
Retention is defined as, “That quality inherent in the prosthesis which resists the force of gravity, adhesiveness of foods and the forces associated with the opening of the jaws”–GPT. Retention is the ability of the denture to withstand displacement against its path of insertion.
Factors that affect retention can be classified as:
- Anatomical factors.
- Physiological factors.
- Physical factors
- Mechanical factors.
- Surgical factors.
- Psychologic factors.
Anatomical Factors:
- Maximum coverage of the basal seat area.
- Quality of denture bearing area, if the ridges are parallel and well formed better the retention.
- Oral facial musculature.
- Neuromuscular control.
Oral and Facial Musculature:
- The oral and facial musculature can supply supplementary retention provided
- If the teeth are positioned in the neutral zone.
- If the polished surfaces of the dentures are properly shaped.
- The buccal flanges of the maxillary denture slope up and out from the occlusal surfaces of the teeth and the buccal flanges of the mandibular denture slope down and out from the occlusal plane.
- The lingual surfaces of the lingual flanges should slope toward the center of the mouth so the tongue can fit against them. The “S” shaped area in the impression copied on to denture also perfects the seal in the posterior lingual aspect.
- The denture bases must cover the maximum area without interfering with health and function.
- The occlusal plane should be at the proper level.
Physiological Factors
Saliva: The viscosity of saliva determines retention. Thick and ropy saliva leads to loss of retention. Thin and watery saliva also leads to compromised retention.
In ptyalism, the patient suffers from a gagging sensation, and in xerostomia, dentures can produce soreness and irritation.
Physiological Factors Physical Factors:
- Adhesion.
- Cohesion.
- Interfacial surface tension.
- Capillarity or capillary attraction.
- Atmospheric pressure and peripheral seal.
- Gravity.
Physiological Factors Adhesion:
- Adhesion is defined as, “The physical attraction of unlike molecules to one another.” –GPT. Saliva is very important for adhesion.
- A thin film of saliva aids in wetting the tissue surface of the denture and the mucosa. The amount of adhesion present is proportional to the denture base area.
- Denture base materials that help in wetting have better retention by adhesion than materials that cause drops of water to form over their surfaces. Thick ropy saliva is formed by palatal glands and tends to displace dentures by hydraulic pressure.
Physiological Factors Cohesion:
Cohesion is defined as, “The physical attraction of like molecules for each other”. The cohesive forces act within the thin film of saliva. The greater the denture-bearing area, the more effective cohesion. A thin film of saliva is more cohesive than thick mucus saliva.
Physiological Factors Interfacial Surface Tension:
- Interfacial surface tension is defined as, “ The tension or resistance to separation possessed by the film of liquid between two well-adapted surfaces.” GPT.
- These forces are found within the thin film of saliva separating the denture base from the tissues which in turn resist the displacing forces. It plays a major role in the retention of a maxillary denture. This force is dependent on the presence of air at the margins of liquid and solid contact (liquid-air interface).
Factors affecting interfacial surface tension:
- Consistency of Saliva. (Should be thin and even).
- The perfect fit of the denture base.
- Maximum coverage of basal seat area.
- Good adhesive and cohesive forces, which aid to enhance interfacial surface tension.
Capillary Attraction:
- Capillarity or capillary attraction is defined as “That quality or state because of surface tension causes elevation or depression of the surface of a liquid that is in contact with a solid.
- GPT Capillary attraction is a phenomenon in which a liquid tends to rise in a capillary tube by maximizing its contact along the walls of the tube at the interface between the liquid and glass.
- When there is a close adaptation between the denture and the mucosa, a thin film of saliva tends to flow and increase its surface contact thereby increasing the retention.
Factors that aid to improve capillary attraction:
- Good adaptation of denture base to soft tissue.
- The greater surface of the denture-bearing area.
- A thin film of saliva.
Atmospheric Pressure and Peripheral Seal:
- Peripheral seal is the area of contact between the peripheral borders of the denture and the resilient-limiting structures which prevents air entry between the denture and the soft tissue.
- A good peripheral seal will have the denture borders resting on soft and resilient tissues. When displacing forces act on the denture, a partial vacuum (natural suction) is produced between the denture and the soft tissues, which aids in retention.
- Hence, atmospheric pressure is referred to as emergency-retentive force or temporary restraining force.
Factors affecting atmospheric pressure:
- Good peripheral seal.
- The perfect fit of denture.
- Maximum coverage of basal seat.
Mechanical Factors:
- Undercuts
- Balanced occlusion
- Springs
- Magnets
- Denture adhesives
- Suction chambers and suction discs
- Gum Tragacanth.
Undercuts: Unilateral undercuts aid in retention while bilateral undercuts will interfere with denture insertion and require surgical correction.
Magnetic forces: Intramucosal magnets aid in increasing the retention of highly resorbed ridges.
Denture adhesives: They are available as creams or gels or powders. They should be coated on the tissue surface before wearing the denture.
Suction chambers and suction discs: The suction chamber creates an area of negative pressure, which increases retention. But can also cause palatal hyperplasia.
Surgical factors: Vestibuloplasty, Zygomaticoplasty, Tuberoplasty, Ridge augmentation procedures, and implants.
Psychologic factors: as Patient tolerance and patient education.
Leave a Reply