Nonfermenters
Nonfermenters utilize the sugars oxidatively. Important members are Pseudomonas, Burkholderia, and Acinetobacter.
Table of Contents
Pseudomonas
Virulence Factors and Pathogenesis
- Colonization: To colonize the host surface by pili or fimbria (the organ of attachment)
- Toxin-mediated immune evasion and Tissue Injury:
- Nondiffusible toxins (e.g. exotoxins S, U, T, and Y)
- Diffusible toxins (e.g. exotoxin A, proteases, phospholipases, hemolysins, elastases, pyocyanin, etc.)
- Exotoxin A is the most important virulence factor. It inhibits protein synthesis by inhibiting EF-2 (mechanism of action is similar to diphtheria toxin).
- Host’s inflammatory response: Against lipid A of LPS and flagellin
- Pigment production:
- Pyocyanin (a blue-green pigment, produced only by P. aeruginosa)
- Fluorescein (or pyoverdin): Gives greenish-yellow color, produced by all species
- Pyorubin (imparts red color)
- Pyomelanin (imparts brown black color).
- Alginate coat: Mucoid strains of Pseudomonas have a slime layer or alginate layer which facilitates biofilm formation, thus helps in adhesion to purulent mucus.
- Such strains can cause infections in patients with cystic fibrosis.
- Capsular polysaccharide prevents the bacteria from phagocytosis.
- Multi-drug resistance and Multi-disinfectant resistance.
- Wide temperature range (5–45 °C).
Read And Learn More: Micro Biology And Immunology Notes
Clinical Manifestations
- Most of the infections are encountered in hospitalized patients.
- Pneumonia: (VAP or Ventilator-Associated Pneumonia).
- Chronic respiratory tract infections: Occurs in patients with cystic fibrosis (in Caucasian populations), bronchiectasis or chronic panbronchiolitis (in Japan):
- The mucoid strains (possessing alginate layer) of Pseudomonas commonly cause such infections.
- Structural abnormalities of the airways result in mucus stasis.
- Ear infections: Swimmer’s ear (among children) and malignant otitis externa (in elderly diabetic patients).
- Eye infections such as corneal ulcers (in contact lens wearers) and endophthalmitis.
- Shanghai fever: A mild febrile illness resembling typhoid fever.
- Skin and soft tissue infections:
- Burns patients: Pseudomonas is the most common organism to infect the burn wounds.
- Ecthyma gangrenosum (is an acute necrotizing condition results from bacteremia), occurs more commonly in patients with febrile neutropenia and AIDS.
- Pseudomonas dermatitis: Cause outbreaks in spas, and swimming pools.
- Toe-web infections (in the tropics).
- Green nail syndrome: It is a ‘paronychia’ results from prolonged submersion of the hands in water.
- Other infections:
- Cellulitis (characterized by blue green pus)
- Bone and joint infections such as osteomyelitis and septic arthritis
- Meningitis (in postoperative or post-traumatic patients)
- UTI (urinary tract infection) in catheterized patients.
Laboratory Diagnosis
Pseudomonas is nonfastidious, obligate aerobe and is motile with single polar flagellum:
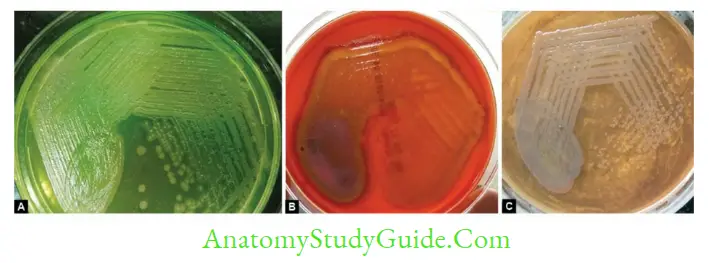
- It produces large, opaque, irregular colonies with a metallic sheen (iridescence)
- Diffusible pigments: Blue green (pyocyanin) or yellow green (pyoverdin) pigmentation
- Pigment production can be enhanced in special media such as King’s media
- Most colonies have a characteristic sweet ether or alcohol-like fruity odor
- Blood agar: It produces β hemolytic colonies on blood agar
- MacConkey agar: Produce pale nonlactose fermenting colonies
- Selective media-cetrimide agar
- Oxidase and catalase positive
- Nonfermenter: It does not ferment any sugars, but utilizes sugars oxidatively.
- OF test (Hugh and Leifson oxidative fermentative test) shows oxidative pattern.
Treatment
Pseudomonas species are inherently resistant to most of the antibiotics. Only limited antipseudomonials are available:
- Penicillins: Piperacillin, mezlocillin, ticarcillin
- Cephalosporins: Ceftazidime, cefoperazone, and cefepime
- Carbapenems: Imipenem, meropenem
- Monobactam: Aztreonam
- Aminoglycoside: Tobramycin, gentamicin, amikacin
- Quinolones: Ciprofloxacin, levofloxacin
- Polymyxins: Polymyxin B, colistin.
Drug Resistance
- Pseudomonas possesses a number of drug resistant plasmids which confer multiple drug resistance.
- Many strains are producers of β lactmases such as ESBL (extended spectrum β lactamases), carbapenemases, and AmpC β lactamases.
- Many strains are resistant to aminoglycosides and quinolones.
Burkholderia
Burkholderia species are also oxidase positive nonfermenters; however they differ from
- Pseudomonas in being:
- Bipolar stained (safety pin appearance)
- Resistant to polymyxin B.
Burkholderia Pseudomallei (Melioidosis)
- B. pseudomallei is the causative agent of melioidosis.
- Habitat: B. pseudomallei is a saprophyte of soil and water and have large number of animal reservoirs.
- Mode of transmission: by inoculation, inhalation, aspiration or ingestion. Man to man transmission is very rare.
- Virulence factors:
- Polysaccharide capsule, type III secretion system,
- LPS, toxins, enzymes and proteins (such as hemolysin, lipases and proteases),
- Quorum sensing, type IV pili and siderophore for iron acquisition.
- Risk factors: Diabetes, renal failure and traumatic inolcutaion in children, weather (rainy season) and occupation (rice farmers).
- Incubation period: 2 days to many years. Has long latency; presented long time after the exposure; hence also known as ‘Vietnam time-bomb disease’.
- Clinical feature: Can present with an array of manifestations (hence called as ‘great mimicker’)
- Acute, localized infection: Nodule, fever, general muscle aches
- Sub-acute (Pulmonary) infection: bronchitis to severe tuberculosis-like pneumonia with cellulitis and lymphangitis
- Acute bloodstream infection: Seen in patients with HIV, renal failure and diabetes and presents as septicemia
- Chronic suppurative infection forming abscesses: Involves various organs such as joints, viscera, lymph nodes, skin, brain, liver, lung, bones, and spleen.
- Geographical distribution: 1.65 lakh new cases of melioidosis occur worldwide every year with mortality as high as 50%.
- World: Endemic in Thailand, Australia, Singapore, Indian subcontinent and other Southeast Asian countries.
- India: It has been reported mainly from South India such as Tamil Nadu, Karnataka, Puducherry and Kerala.
- Ashdown’s medium is used as a selective medium, where it produces wrinkled purple colonies.
- Cultures can be confirmed by latex agglutination test using specific antisera.
- Treatment of melioidosis consists of:
- Intensive phase (2 weeks): Ceftazidime or a carbapenem is given
- Maintenance phase (12 weeks): Oral cotrimoxazole is given to eradicate the bacilli and to prevent relapse.
- Doxycycline or amoxicillin-clavulanate are the alternatives.

Burkholderia Mallei
- B. mallei is a pathogen of horses; causes glanders (nasal discharge and ulcers in the nasal septum) and farcy (skin lesions and lymph node involvement).
- Human infection is characterized by:
- Local skin nodules and lymphadenitis (if transmitted by inoculation)
- Pneumonia, ulceration of the trachea and sepsis (if transmitted by inhalation)
- B. mallei differs from B. pseudomallei in being:
- Nonmotile and Oxidase negative
- Inability to grow on MacConkey agar
- Inoculation into Guinea pigs can cause testicular swelling (Strauss reaction).
Burkholderia Cepacia
- B. cepacia is currently the most commonly encountered Burkholderia species:
B. cepacia inhabits moist environments, detergents and IV fluids. - LPS of B. cepacia is among the most potent of all gram-negative bacteria.
- Cepacia syndrome characterized by a rapidly fatal respiratory infection and septicemia in cystic fibrosis patients.
Nosocomial pathogen in ICU patients because as it is resistant to multiple antibiotics.
Acinetobacter
- Acinetobacter are saprophytic bacilli. However, it is recognized as a nosocomial pathogen:
- It can cause ventilator associated pneumonia, Central line associated bloodstream infection, Catheter associated UTI.
- Wound and soft tissue infections and infections in burn patients.
- A. baumannii is nonfermenter, but differs from Pseudomonas being Oxidase negative and Nonmotile.
Haemophilus
- Haemophilus species are oxidase positive, capsulated pleomorphic gram-negative bacilli. It
- (Pfeiffer’s bacillus) is blood loving organism; requires two accessory growth factors present in blood.
- Factor X- hemin present freely in blood Factor V is an NAD (present in side RBC)
- Virulence Factors and Typing
- Capsule-Based on Capsular polysaccharide, H. influenzae is typed into six serotypes (a to f):
- H. influenzae serotype b (Hib) is the most virulent and accounts for most of the invasive infections.
- Hib capsule has unique chemical structure, made up of polyribosylribitol phosphate (PRP) antigen.
- It is strongly immunogenic, hence used for vaccination.
- Next to Hib, nontypeable strains are commonly isolated clinically. Other capsular serotypes are very rarely isolated.
- H. influenzae was the first free-living organism whose entire genome was sequenced.
Clinical Manifestations
- H. influenzae type b (Hib) is the most common and most invasive serotype.
- Central nervous system infections:
- Pyogenic meningitis in < 2 years of age
- Subdural effusion, MC CNS complication
- Epiglottitis: Seen in older children (2-7 years), absence among Navajo Indians and Alaskan Eskimos.
- Lobar Pneumonia in infants
- Less common invasive conditions seen in children include:
- Cellulitis of neck and head region
- Osteomyelitis, septic arthritis
- Orbital cellulitis, endophthalmitis
- Next to Hib, non-typeable strains are the commonest group clinically.
- They are noninvasive, spread by contagious spread and usually affect adults.
- Their clinical manifestations include:
- Childhood otitis media
- Exacerbations of COPD: They are the MC bacterial cause for this condition.
- Pneumonia in adults among patients with COPD or AIDS
- Puerperal sepsis and neonatal bacteremia- by strains of biotype IV.
- Sinusitis in adults and children.
Laboratory Diagnosis
- Specimen collection and transport:
- CSF, blood, sputum, pus, aspirates from joints, middle ears or sinuses.
- As it is highly sensitive to low temperature, the specimens should never be refrigerated.
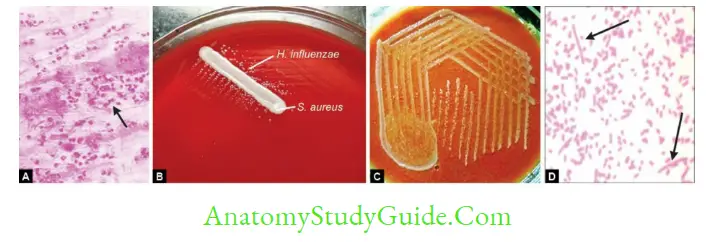
- Gram staining of CSF and other specimen shows pleomorphic gram-negative coccobacilli
- Capsule detection: By Quellung reaction or Latex aggl. test
- Culture: H. influenzae is largely aerobic, growth is enhanced by 5–10% CO2.
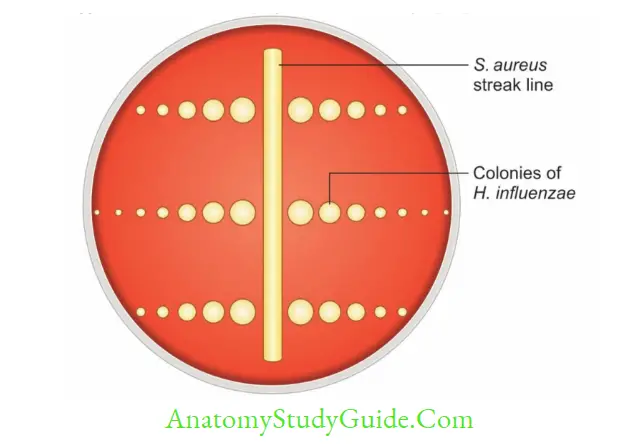
- Blood agar with S. aureus streak line: Colonies of H. influenzae grow adjacent to S. aureus streak line (this property is called as satellitism).
- This is due to release of V factor by lysis of RBCs mediated by S.aureus.
- Chocolate agar: It grows well on chocolate agar but sparsely on blood agar.
- Fildes agar and Levinthal’s agar.
- Disk test for X and V requirement:
- Biotyping: It is done by IOU tests (indole, urease test and ornithine decarboxylase test).
Slide agglutination test: Serotyping is carried out using type-specific antisera.
Treatment
- Invasive infection due to Hib: Cephalosporins are the drugs of choice.
- Nontypeable strains of H. influenzae are often resistant to β lactams [due to β-lactamase production (20–35% of strains) or rarely altered penicillin binding protein-3]. DOC is quinolones
- (levofloxacin) or macrolides (azithromycin).
- Chemoprophylaxis: Oral rifampin is indicated to household contacts or healthcare staff (if two or more cases occur within 60 days).
Hib Conjugate Vaccine
- The PRP capsular antigen of H. influenzae type b is used as vaccine.
- As capsular antigens are poorly immunogenic to children, they are conjugated with adjuvants such as diphtheria toxoid, tetanus toxoid.
- It also reduces the rates of pharyngeal colonization with Hib.
- Conjugate vaccines has dramatically reduced the incidence of Hib disease.
H. aegyptius
- Koch’s –Week’s bacillus
- Pink eye syndrome (Egyptian ophthalmia)
- Brazilian purpuric fever.
- H. ducreyi
- Causes Chancroid/soft sore: Characterized by painful lymph node, tender non-indurated and bleeding genital ulcer
- Chancroid increases both transmission and the degree of susceptibility to HIV infection
- In direct smear: Pleomorphic gram-negative coccobacilli that: Show bipolar staining
- Occurs in parallel chains called in ‘School of fish’ or ‘rail road track’ appearance
- Antigenically homogenous
- Culture Medium used:
- Rabbit blood agar or Chocolate agar with 1% isovitalex, Vancomycin
- Chorioallantoic membrane (CAM)
- Drug of choice: Azithromycin (1 g oral; single dose), treatment of all sexual partners.
- Haemophilus aegyptius
- It is also called as Koch-Weeks bacillus; closely resembles H. influenzae biotype III.
- It causes:
- Brazilian purpuric fever: A fulminant condition, characterized by fever, purpura, hypotension and shock
- Purulent contagious conjunctivitis (Egyptian ophthalmia).
HACEK Group
- HACEK organisms are a group of highly fastidious, gram-negative bacteria, normally residing in the oral cavity as commensal, but occasionally have been associated with local infections in the mouth and systemic infections, such as bacterial endocarditis:
- Haemophilus species: H. aphrophilus, H. paraphrophilus and H. parainfluenzae
- Aggregatibacter (formerly Actinobacillus) actinomycetemcomitans: Most common member
Cardiobacterium hominis - Eikenella corrodens: Produces twitching or jerky motility and pitting or corroded colonies on blood agar Kingella kingae
Treatment: Ceftriaxone (2 g/day) is the DOC except for Eikenella corrodens where ampicillin is indicated.
Bordetella
Bordetella is described first by Bordet and Gengou, causes a violent paroxysmal productive cough in children called as whooping cough or 100 days fever.
Virulence Factors
Toxins:
- Pertussis toxin (PT) expressed only by B.pertussis, similar to cholera toxin in its structure and function (↑ cAMP)
- Other toxins: Tracheal cytotoxin, adenylate cyclase toxin, dermonecrotic toxin and Endotoxin
- Adhesins: They play a role in bacterial attachment:
- Filamentous hemagglutinin (FHA)
- Pertactin, an outer-membrane protein
- Fimbriae or pili or agglutinogens.
Clinical Manifestations
Whooping cough (or pertussis) passes through three stages following an IP of 7–10 days.
1. Catarrhal phase: It lasts for 1–2 weeks, is characterized by common cold like nonspecific
- symptoms. It is highly infectious stage and smear and cultures are likely to be positive.
2. Paroxysmal phase: It is characterized by specific symptoms such as:
- Whooping cough, post tussive vomiting
- In this stage, patient is less infectious; smear and culture become negative.
3. Convalescent stage: Severity decreases. Antibodies appear in serum.
Epidemiology
- Whooping cough is exclusively human disease. There is no animal reservoir:
- Mode of transmission is via inhalation of droplets or rarely through direct contact.
- Recent outbreaks: Washington epidemic in 2012 and California epidemic in 2014 Worldwide, the incidence of pertussis is declining.
- WHO estimated around 1,39,535 cases of pertussis in 2016 and 1,42,512 in 2015 with 89,000 deaths; (Mainly in unvaccinated children).
- WHO reported an estimated global vaccine coverage of 86% in 2016.
- There is no cross protection to B. parapertussis infection.
Laboratory Diagnosis
- Best Specimen: Nasopharyngeal secretions, obtained by nasopharyngeal aspiration (best method) or pernasal swab
- Type of swabs used: Alginate swabs are the best followed by dacron swabs for culture.
- However, for PCR, only dacron or rayon swabs are recommended.
- If delay is expected, then suitable charcoal-based transport medium (Amies or Stuart’s) can be used.
- Cough plate method and postnasal swabs used before are no longer recommended.
- Antigen detection: Direct fluorescent antibody tests of nasopharyngeal secretions
- Culture: Nasopharyngeal aspirate culture is the Gold standard method
- Media: Regan and Lowe medium, Bordet-Gengou glycerine-potato-blood agar
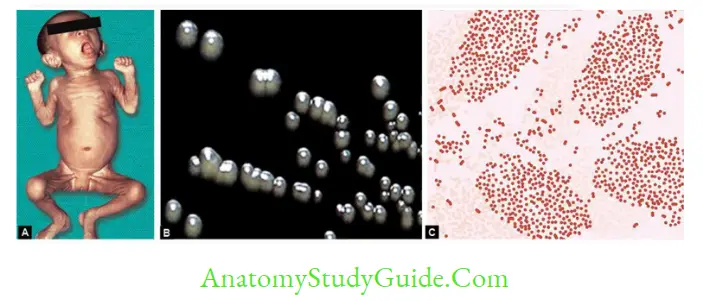
- Colonies: Mercury drops or bisected pearls appearance.
- Culture smear: Reveals small, ovoid coccobacilli arranged in thumb print appearance.
- Capsules and bipolar metachromatic granules may be seen occasionally.
- PCR: Most sensitive, gives quicker results, but yet to be standardized properly.
- The most common targeted genes are IS481 and the PT promoter region genes.
- Antibody detection: Enzyme immunoassays detecting IgA and IgG to pertussis toxin, filamentous hemagglutinin.
Treatment
- Antibiotics eliminates the bacteria from nasopharynx, but less useful for treatment as pertussis is toxin mediated.
- Macrolides are the drugs of choice (e.g. erythromycin for 7–14 days)
- Cotrimoxazole is recommended as an alternative in macrolide resistance.
- Chemoprophylaxis: Erythromycin is DOC.
Vaccine
- Whole-Cell Pertussis Vaccines
- It is prepared by heating followed by chemical inactivation and purification of whole B.pertussis bacilli.
- It is given along with DPT to children < 5 years age
- Efficacy is good, average being 85%. Adverse effects
- Common: Fever, injection-site pain, erythema, swelling, and irritability.
- Rare: Neurological complications and hypotonic hyporesponsive syndrome
- WC vaccine is contraindicated in: Children > 5–6 years age
- Associated progressive neurological conditions or family history of epilepsy
- Hypersensitivity to previous dose.
- Acellular Pertussis Vaccine
- It is composed of pertussis toxoid and ≥ 2 other bacterial components such as FHA, pertactin or fimbriae.
- Though the efficacy is same as WC vaccine, it is associated with fewer side effects and safely given after 5–6 years.
Brucella
- Brucellosisis (also called undulant fever) primarily a zoonotic disease acquired from animals such as sheep, goat, or cattle.
- Nomen System of Classification
- DNA hybridization reveals that Brucella are very closely related and probably represent variants of a single species.
- However for the sake of convenience, these have been classified into nomen species.
- Nomen species: Six nomen species identified so far, further classified into several biovars
Pathogenesis
- B.melitensis is most pathogenic followed by B. abortus andB. suis. Human infection with other species is extremely rare.
- Transmission—is usually from infected animals to man. There is no evidence of man to man transmission.
- Direct contact (MC mode) with the infected animal tissue > Ingestion of raw milk or dairy products > Air borne
- Organs affected: Brucellae are facultative intracellular pathogens, primarily infecting organs of reticuloendothelial system.
- Incubation period varies from 1 week to several months and the onset is often insidious.
Clinical Manifestations
- Classic triad: Fever with night sweats; arthralgia/arthritis and hepatosplenomegaly
- Typhoid-like illness: Overall, brucellosis resembles typhoid like illness except that,
- it is less acute, less severe with undulating pattern of fever (or Malta fever or Mediterranean fever) and more musculoskeletal symptoms.
- CNS (Depression and lethargy with meningitis or lymphocytic meningoencephalitis), CVS (Endocarditis rarely, affecting the aortic valve)
- Genitourinary manifestations (acute epididymo-orchitis, prostatitis, salpingitis and pyelonephritis) may also be seen.
Epidemiology
- Endemic area:
- Human brucellosis is endemic in countries of Mediterranean zone,
- Eastern Europe, Central Asia, Mexico and
- South America and rare in most European countries, Australia and North America.
- Sources of infection:
- Infected animals excreting the organisms in urine, milk, placenta or vaginal discharge and Contaminated animal food products (soft cheeses, milk, icecream)
- People at higher risk are farmers, shepherds, goatherds, butchers and abattoir workers in endemic areas (occupationally exposed to infection).
Laboratory Diagnosis
- Culture and Identification
- Sample: Blood, bone marrow, CSF, joint fluid or other tissues.
- Cultural media: Biphasic blood culture bottles media (Castaneda’s) made up of Brain heart infusion (BHI) broth/agar
- Erythritol: Improves growth Automated techniques such as BACTEC and BacT/Alert systems.
Antibody Detection by Standard Agglutination Test (SAT)
- It remains the gold standard test serological test:
- It is a tube agglutination test detecting antibodies in serum by using standard strain of B.
- SAT detects IgM antibodies against antigens of smooth LPS: Hence useful for acute brucellosis
Other Tests
- Serological tests to detect IgG antibody—2ME (2-mercaptoethanol) test, CFT, ELISA.
- PCR using primers for rrs-rrl gene, Omp2 gene and IS711 insertion sequence.
- Brucellin skin test
- Guinea pig inoculation
- Tbilisi phage typing is done
- Diagnosis of brucellosis in animals
- Isolation of brucellae from milk and dairy products.
- Antibody detection in milk: By Milk ring test, Rose Bengal card test, and whey agglutination test.
Treatment
- Gold standard regimen in adults: Streptomycin plus doxycycline
- WHO regimen in adults: Rifampin plus doxycycline
- Relapse or treatment failure occurs in 5–10% of cases.
- For CNS involvement: Ceftriaxone is added to the regimen and treatment is prolonged for 3–6 months.
Leave a Reply