Pulp Oral Histology Notes
Pulp
Pulp is a soft connective tissue of the tooth which is mesodermal in origin, highly vascularized and innervated. It is present in the centre of the tooth surrounded by dentin on all the sides. Pulp and dentin are closely related embryologically, functionally and histologically and hence are together referred as the pulp–dentin complex.
Table of Contents
Salient Features Of The Pulp
- Pulp is a highly vascularized connective tissue.
- Coronal pulp: Pulp present in the crown of the tooth called pulp chamber.
- Radicular pulp: Pulp present in the root of the tooth.
- The shape of the pulp varies in different teeth and resembles the outer surface of the crown.
Read And Learn More: Oral Histology Notes
- Size of the pulp: Posteriors > Anteriors.
- Number of pulp organs: Deciduous – 20, Permanent – 32.
- Surfaces of the coronal pulp: Six (Occlusal, mesial, distal, buccal, lingual, floor).
- Communications with the periradicular tissues:
-
- Through apical foramen
- Through lateral/accessory openings/canals
Pulp Origin
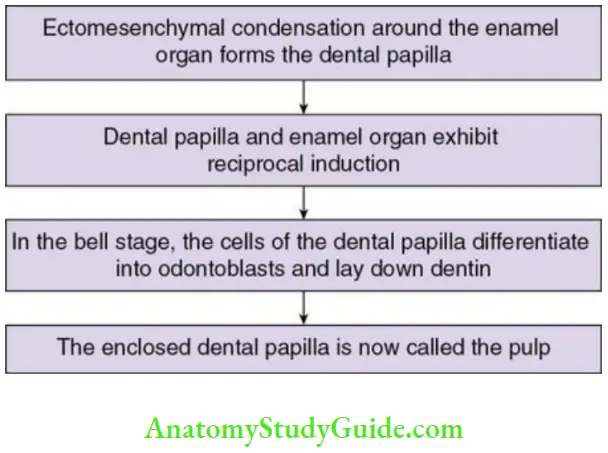
- The condensation of mesenchyme invaded by the neural crest
(ectomesenchyme) around the developing enamel organ are referred to as dental papilla. - With growth of the tooth germ, the dental papilla expands and exerts a morphogenetic effect on the enamel organ. The mesenchymal cells that surround the dental papilla comprise the dental follicle and give rise to the cementum and periodontal ligament.
- As the enamel organ enters the bell stage of tooth development, the cells of the dental papilla differentiate into outer layer of odontoblasts and inner layer of fibroblasts. Under the influence of the inner enamel epithelium, the odontoblasts lay down dentin and the dental papilla now becomes the dental pulp.
- As the pulp matures, cytoplasmic organelle appear within the cells and fibre bundles appear in the ground substance. The formation of dental pulp is considered to be complete once the entire root develops.
Parts Of The Pulp
Coronal pulp:
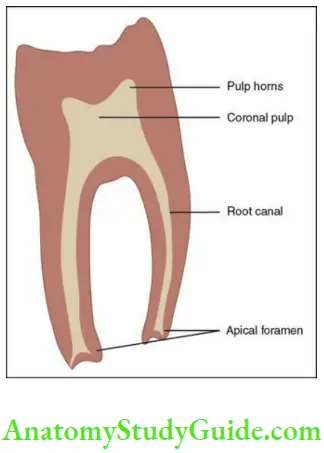
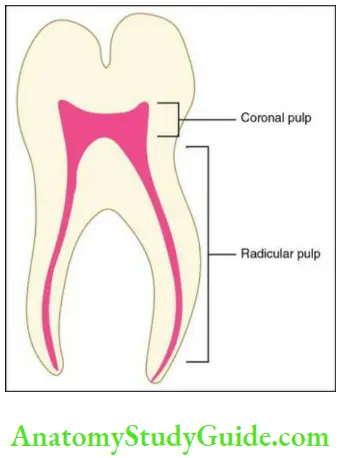
- The pulp presents in the centre of the crown of the tooth is called coronal pulp.
- It has pulp horns. Pulp horns are protrusions extending into the cusps; thus, the number of pulp horns corresponds to the number of cusps.
Coronal pulp Clinical Considerations
- The size of the coronal pulp decreases with age due to the deposition of the secondary dentin.
- The pulp horn might get exposed during cavity preparation; thus, a dentist has to be careful while preparing a cavity.
Radicular pulp:
- The pulp presents in the root canals of the teeth is called radicular pulp.
- It varies in size, shape and number in different teeth.
- It communicates with the periapical tissues via a large foramen known as the apical foramen.
Radicular pulp Clinical Consideration
The radicular pulp gradually becomes obliterated due to the deposition of secondary dentin, thus it is making root canal treatment as complicated.
Communications Of The Pulp
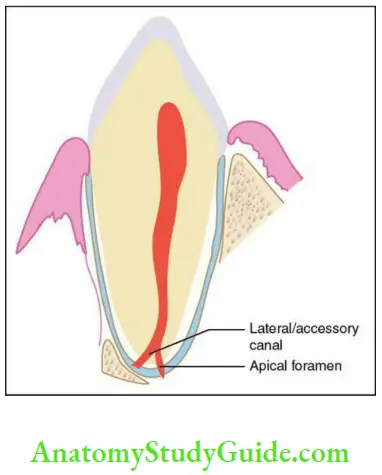
Apical foramen:
- Apical foramen is the foramen through which the pulp communicates with the periapical tissues. Blood vessels and nerves enter the tooth through this foramen.
- The location, shape, size and the number of the apical foramen is not constant.
Location: The apical foramen is generally located centrally in a developing tooth; as the development is complete, it assumes an eccentric position.
Average size: Maxillary teeth – 0.4 mm; mandibular teeth – 0.3 mm
Number: One, two or more.
Communications Of The Pulp Clinical Consideration:
With the advancement of age, the apical foramen gets obliterated due to the deposition of dentin which reduces the vitality/healing potential of the pulp.
Accessory canals or lateral canals:
- The extra canals present in the root are called accessory or lateral canals. They extend from the root canal to the periradicular or the periodontal tissues.
- They are seen most commonly in the apical third of the root and in the furcation areas of molars. They are formed due to extensive looping of the tooth root around a blood vessel or premature loss of the root sheath during root development.
Accessory canals Clinical Considerations
- Infection may spread from the pulp to the periodontal tissues or vice versa through accessory canals, which can lead to an endo-perio lesion.
- It can be one of the reasons for the failure of root canal treatment
Histology Of The Dental Pulp
There are four zones present in the dental pulp, which are as described in Table
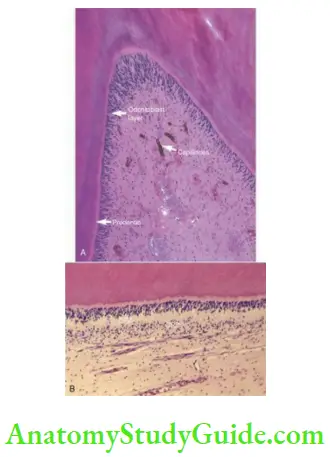
Zones of the Pulp:
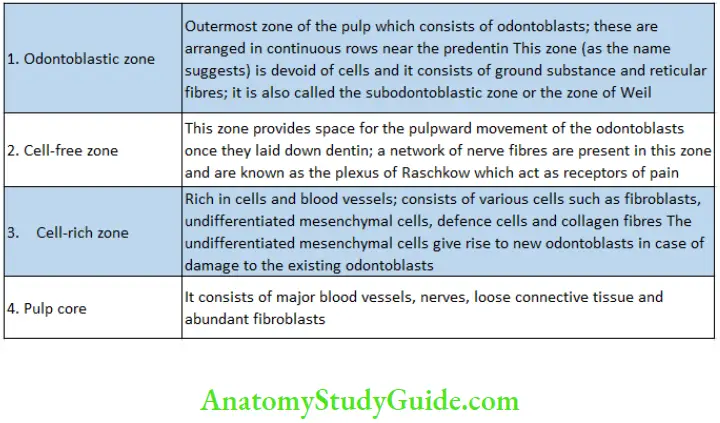
Zones Of The Pulp
Odontoblastic zone
Cell-free zone
Cell-rich zone
Pulp core
The pulp consists of the following:
- Cellular components
- Extracellular components
- Connective tissue elements
Components of the Pulp:
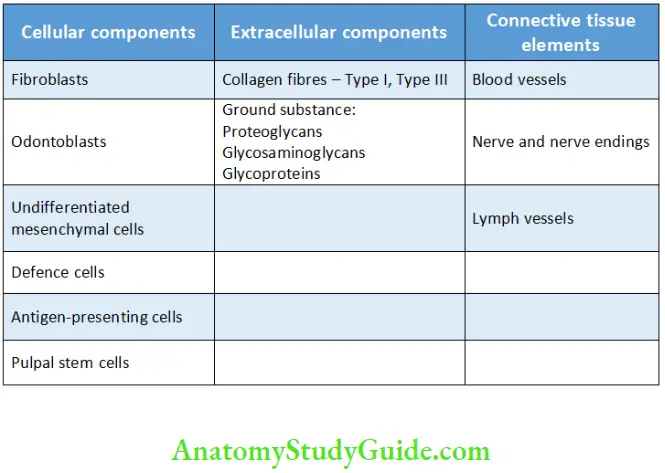
Cellular Components Of The Pulp
Fibroblasts:
- Fibroblasts are the most common cells present in the pulp.
- They play an important role in the maintenance of the matrix of the pulp. They serve the dual function of formation and degradation of the collagen matrix.
- In the young individual, the fibroblast is active and acquires a fusiform shape; with age, there is a decrease in activity and they become spindle shaped and are called fibrocytes.
- They also play a role in inflammation by the release of mediators of inflammation such as cytokines and also secrete growth factors.
Odontoblasts
- Odontoblasts are the second most abundant cells in the pulp.
- They lay down dentin and are derived from the ectomesenchyme.
Shape:
- Long and cylindrical in the crown; cuboidal in the centre of the root; spindle shaped at the apex of the tooth.
Odontoblasts Location:
- Present in the odontoblastic zone where the cell bodies are arranged in a continuous row near the pre-dentin.
Odontoblasts Number:
- Corresponds to the number of dentinal tubules. It could range from 59,000 to 76,000 per mm2. They are more in number in the crown than in the root.
The odontoblasts are further divided into three types based on the activity as follows:
- Active odontoblasts
- Intermediate odontoblasts
- Resting odontoblasts
Phases of Odontoblasts
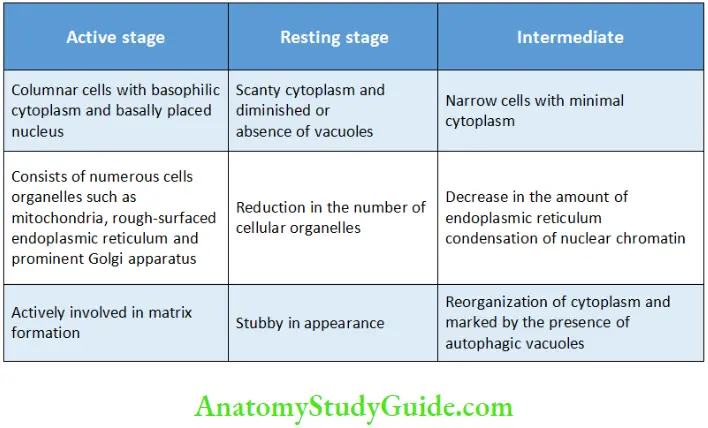
The odontoblasts are rich in cellular organelles, such as mitochondria, endoplasmic reticulum, Golgi apparatus, vesicle and granules. The cell body of the odontoblasts is columnar in shape with a basally placed oval-shaped nucleus. The cytoplasmic process extends into the dentinal tubules up to the dentinoenamel junction.
The cytoplasmic extensions do not contain cellular organelles. There are several microtubules and filaments present within the extension. Odontoblasts are end cells as they cannot undergo cell division. Their life span is believed to be equal to that of the viable tooth.
Undifferentiated mesenchymal cells:
- Undifferentiated mesenchymal cells are pluripotent cells seen in the pulp. They have the capacity to give rise to various other cells such as fibroblasts, odontoblasts or macrophages.
- They act as a reservoir of cells and give rise to other cells in cases of injury to the pulp.
- The number of these cells decreases with age.
- They are exclusively found in the cell-rich zone of the pulp.
- These cells are polyhedral in shape with an oval nucleus.
Defence cells:
The defence cells consist of
- Histiocytes: Histiocytes are also known as macrophages. They play an important role of phagocytosis. These are irregular in shape, containing granular cytoplasm, with a small round nucleus, cell organelle such as rough-surfaced endoplasmic reticulum, ribosomes, mitochondria and phagocytic vesicles known as phagosomes.
- Dendritic cells: Dendritic cells are bone marrow-derived antigen-presenting cells, which play an important role in immunosurveillance. They trap the foreign antigen and present it to the defence cells like T cells. These cells are found in close approximation with the odontoblastic layer and communicate with the adjacent odontoblasts by means of dendritic processes. The number of
these antigen-presenting cells is more in the teeth affected with caries, and attrition. - Eosinophils and lymphocytes: These are extravascular cells seen in the normal pulp. There is marked increase in the number of these cells during inflammation and damage to the pulp.
- Mast cells: They play a role in inflammation by the release of histamine. Their number increases gradually in case of inflammation.
- Plasma cells: These cells provide immunity to the pulp by the production of antibodies. There is an increase in the number of cells during inflammation and both mature and immature plasma cells may be seen during pulpal inflammation.
Pulpal stem cells:
Pulpal stem cells are a new class of stem cells, isolated from the dental pulp of deciduous and permanent teeth. These are pluripotent stem cells which have selfrenewal capacity and have high angiogenic, chondrogenic, osteogenic, adipogenic and neurogenic differentiation potential. They have been recently introduced in the area of regenerative endodontics because of their pluripotent nature. These are also known as dental pulpal stem cells.
Extracellular Components Of The Pulp
- The ground substance provides support to the cells.
It also helps in exchange of nutrients from the vascular component to the cell and various other metabolites from the cell to the vasculature. - With age, the ground substance is reduced, which causes disturbance in mineral deposition, reduced vascularity of cells and metabolic alterations.
Ground Sub Stance
Composition of ground substance
- Glycosaminoglycans
- Proteoglycans
- Water
Fibres of pulp
- Collagen – Type I and Type III
- Reticular fibres
- Elastic fibres
The collagen fibres are scattered as individual fibrils between the cells in the younger pulp and are get organized into bundles with age. The former is called diffuse collagen and the latter are called bundled collagen. Bundled collagen is more prominent in the apical region of the tooth. The number of collagen fibres also increase with age.
Blood Vessels In The Pulp
The dental pulp is a highly vascularized tissue. The pulp tissues of the upper and lower teeth are supplied by the superior and the inferior alveolar dental arteries. These blood vessels communicate with the periapical region and the periodontium through the apical foramen and the accessory or lateral canals. They form an extensive
network in the coronal pulp and during its course give lateral branches. Arteriovenous communication is also observed in the pulp.
Blood Vessels In The Pulp Course:

Lymph Vessels Of The Pulp
The dental pulp is drained by the lymph vessels which are thin-walled vessels with an irregular lumen. They are most commonly seen in the coronal region of the pulp and exit the tooth via the apical foramen. The lumen is lined by endothelial cells surrounded
by an incomplete layer of smooth muscle cells. The lymph vessels are characterized by the presence of lymphocytes in the lumen and by the absence of RBCs and discontinuity in the vessel wall and basement membrane in comparison to the venules.
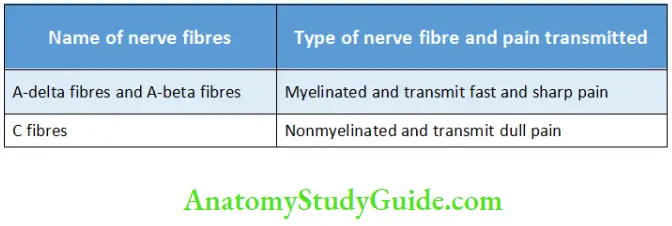
Nerve And Nerve Endings In The Pulp
The dental pulp is highly innervated. The nerve fibres enter the pulp through the apical foramen. Most of the nerve fibres are nonmyelinated. The course of the nerves run along the blood vessels. These nerve fibres arise from the trigeminal nerve.
The nerve bundles enter the coronal pulp and divide to form a network of nerve fibres in the cell-free zone of Weil known as the plexus of Raschkow. There is no corresponding plexus in the radicular pulp. They further give rise to terminal free nerve endings which act as receptors of pain.
Nerves in the Pulp
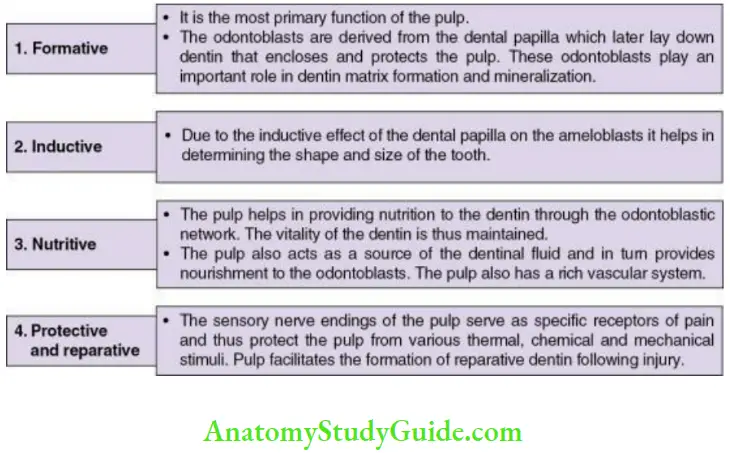
Functions Of The Pulp
Functions Of The Pulp
FINE – Mnemonic for functions of the pulp
Formative
Inductive
Nutritive
Reparative and protective
Functions Of The Pulp
Age Changes In The Pulp
- Changes in cellular components
- Changes in fibrous components
- Vascular changes Changes in innervation
- Calcification (pulp stones)
- Change in volume of the pulp
1. Changes in cellular components
- The number of cells in the pulp decreases with age. This includes the decrease in the number of fibroblasts and odontoblasts.
- There is also a reduction in the size of the cell and the cytoplasmic organelles.
- The cytoplasm is scanty in the ageing fibroblasts; they also demonstrate thin cytoplasmic processes.
2. Changes in fibrous components
- In the ageing pulp, there is an increase in the number of fibres of the ground substance.
- The size of the collagen fibre bundles increases thus making them more prominent. There is an alteration in the arrangement of the fibres; they are arranged in a longitudinal manner in the radicular pulp and in a diffused manner in the coronal pulp.
- Deposition of collagen fibres is also observed in the inner layer of blood vessels.
3. Changes in innervation
- Decreased innervation to the pulp due to loss and degeneration of the nerve fibres is seen. This results in reduced sensitivity and response of the pulp to any noxious stimuli.
- Reduced innervation may also occur due to the obliteration of the apical foramen due to the deposition of secondary dentin.
4. Vascular changes
- There is decrease in the blood flow due to the decrease in the blood vessels and the formation of atherosclerotic plaques in the lumen of the vessels.
- Calcifications may be seen in the walls of the blood vessels in the region close to the apical foramen.
5. Calcifications
These could be
- Pulp stones or denticles
- Diffuse calcifications
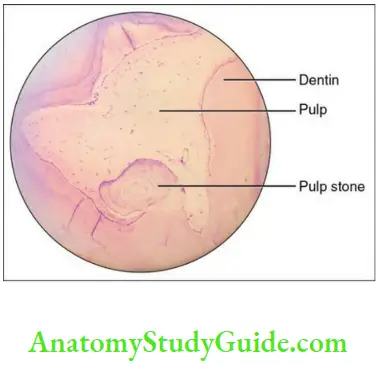
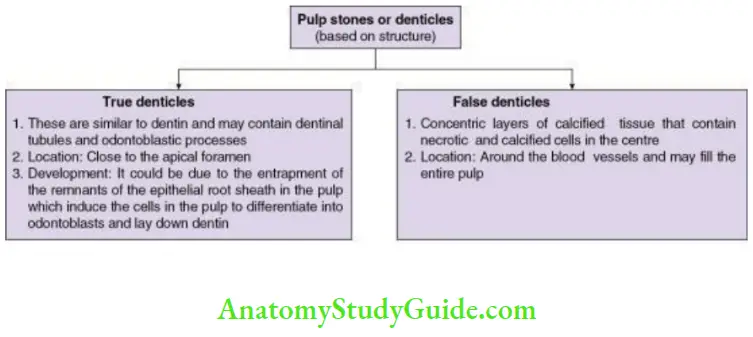
Pulp stones
Pulp stones are small nodular calcified structures
commonly present in the pulp chamber and also seen in
the radicular pulp. The reasons for the formation of the pulp stones are
- Chronic dental caries
- Advancement of age
- Inclusion of the remnants of the epithelial root sheath into the pulp
- Injury of the pulp due to trauma
- During operative and restorative procedures
- Vascular injury due to trauma
- Systemic diseases, e.g. AtherosclerosisIncidence: 60%–70% in 10–30 years of age
75%–80% in 75–80 years of age
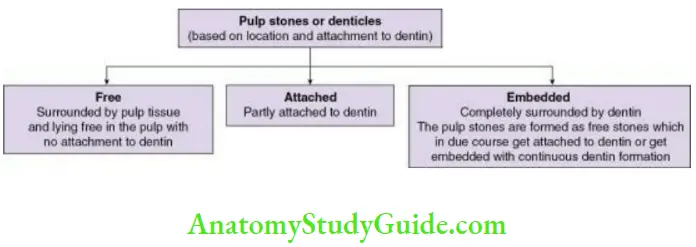
90% in above 50 years of ageRecent studies have suggested increase in the occurrence of pulp stones in patients suffering from cardiovascular disorders; further studies are required to ascertain the same. Pulp stones can be classified on the basis of location and structure and are described in Flowcharts
Diffuse calcifications:
- Irregular calcific deposits in the pulp tissue usually following the collagenous fibre bundles or blood vessels
- Sometimes develop into larger masses or persist as fine calcified spicules
- More often seen in the radicular pulp
- Dystrophic calcifications may be seen around the blood vessels
6. Change in volume of the pulp
The volume of pulp decreases with age
Clinical Considerations Of The Pulp
Shape and location of the apical foramen:
- It is important to for root canal treatment.
- The foramen is easily located if narrowed by deposition of cementum due to the resistance of the broach; but if the location is eccentric then radiographs may not reveal the right length of the root and lead to misjudgement.
Accessory canal:
- Rarely seen in radiographs; mechanically tough to reach them.
- Pulpal and periodontal disease may spread from the pulp to the periodontal ligament or vice versa.
- It can also affect the success of the root canal treatment.
Cavity preparation in a young individual:
- The pulpal horns project into the cusp tips; hence, an exposure is a possibility. Thus, a radiograph is a precautionary measure in the above-mentioned conditions.
- Deep cavity preparation could be hazardous due to a wide pulpal chamber in young patients.
Root canal in an older individual:
- The size of the pulp chamber decreases due to the deposition of secondary dentin thus it is difficult to locate the root canals.
- Pulp stones can cause difficulty in locating the root canals.
Pulpal exposure and pulp capping
- Minimally or noninfected accidental exposure of pulp can be treated by pulp capping at any age. Pulp capping can be
- Indirect pulp capping
- The deepest layer of the remaining dentin is left behind and covered by a layer of biocompatible material to prevent the exposure of the pulp and further trauma.- Aim of this procedure is to preserve the vitality of the pulp by removal of the infected dentin and then placement of the material to stimulate odontoblasts to lay down reparative dentin.
- Direct pulp capping
- Exposed pulp is covered by a protective dressing or base directly over the exposed pulp to preserve the vitality of the pulp. This is possible when the pulpal exposure is small, that is, less than 0.5 mm.
Materials that may be used1. Calcium hydroxide: It has high pH and is bactericidal; thus it promotes tertiary dentin formation. (Particles of calcium hydroxide can get into the pulp and cause pulpal inflammation.) - MTA (mineral trioxide aggregate): More effective than calcium hydroxide as the inflammation and necrosis of the pulp is less; thicker dentin bridge formation is seen.
- Bioactive materials such as BMP (bone morphogenic proteins), transforming growth factor, purified dentin protein fractions, stem cells might be used in future to produce dentin.
- Exposed pulp is covered by a protective dressing or base directly over the exposed pulp to preserve the vitality of the pulp. This is possible when the pulpal exposure is small, that is, less than 0.5 mm.
Pulpitis
- Inflammation of the pulp. This could be due to
- Response to trauma
- Bacterial infection such as caries
- Physical trauma to the tooth, operative procedures
- Chemical insult to the pulp
Pain could be the only symptom in case of pulpitis with the other cardinal signs of inflammation not seen clinically as the pulp is present within the tooth and is surrounded by dentin. Due to the presence of nerve endings, all the sensory stimuli such as pressure temperature or touch manifest in pain. Pain worsens with the severity of inflammation.
- Focal reversible pulpitis: Milder form of pulpitis which may progress if left untreated leading to an acute and chronic form.
- Chronic hyperplastic pulp or pulp polyp: A carious molar of a young adult with an open apex might exhibit a form of hyperplasia seen clinically as a protruding mass of granulation tissue, red in colour which is called a pulp polyp or chronic hyperplastic pulp. The treatment for this condition is root canal therapy or extraction of the tooth.
- Internal resorption or Pink tooth: Inflammation within the pulp causes outward resorption or the dentinal walls leading to the pink appearance of the pulpal through the translucent enamel walls. The treatment of this condition is root canal therapy.
Dehydration
Can cause damage to the pulp and such procedures causing this condition should be avoided. An appropriate cavity liner should be used before the insertion of restorative material that contains harmful chemicals.
Vitality of the pulp:
Vitalometer can be used to test the reaction of the pulp to an electrical or thermal stimuli to test the sensitivity of the pulp rather than the vitality. The vitality depends on
the blood supply and a traumatized tooth may have damaged nerve but normal blood supply. Such a tooth may not respond to an electrical or thermal stimuli but the pulp is otherwise viable.
Nonvital tooth:
A tooth is considered to be nonvital when the pulp in the tooth is necrosed. A nonvital tooth is discoloured as the RBCs in the pulp have undergone lysis and the haemosiderin pigment which is released is taken up by the dentin which in turn becomes dark. This dark coloured dentin is seen through the translucent enamel and the tooth appears brown or black.
Pulp Synopsis
- Pulp is a soft connective tissue which is mesodermal in origin. It is a highly vascularized and innervated tissue of the tooth. It is present in the centre of the tooth surrounded by dentin on all the sides.
- Coronal pulp: It is present in the centre of the tooth called the pulp chamber.
- Radicular pulp: It is present in the root of the tooth.
- Number of pulp organs: Deciduous – 20; permanent – 32
- Surfaces of the coronally pulp: Six (occlusal, mesial, distal, buccal, lingual, floor)
- Communications to the periradicular tissues:
- Through apical foramen
Through lateral/accessory openings/canals - There are four zones present in the dental pulp: Odontoblastic zone, the cell-free zone, the cell-rich zone, the pulp core. The cells in the pulp are fibroblasts, odontoblasts, undifferentiated mesenchymal cells, defence cells, antigenpresenting cells and pulpal stem cells.
- The pulp tissues of the upper and lower teeth are supplied by the superior and the inferior alveolar dental arteries.
- The dental pulp is highly innervated. The nerve fibres enter the pulp through the apical foramen. Most of the nerve fibres are nonmyelinated.
- The chief functions of pulp are formative, nutritive, inductive, protective and reparative.
- The age changes in pulp are reduction in volume and cellular components, increase in fibrous components, reduced vascularity and innervation and formation of calcifications (pulp stones).
Leave a Reply