Pulpectomy In Primary Teeth Introduction
The radical mode of endodontic therapy in primary teeth is indicated when coronal and radicular pulps are irreversibly inflamed or necrosed.
Table of Contents
The treatment objective is to amputate the pulp in toto or completely remove its fragments to eliminate the purulent focus.
This is achieved by pulpectomy, enlargement, and cleansing of the root canal system. Pulpectomy implies the complete removal of pulp tissue, to the clinically possible extent.
Read And Learn More: Paediatric Dentistry Notes
Removing pulp tissue from the lateral canal is not possible. A pulpectomy is followed by root canal filing with suitable materials and post-endodontic restoration.
The radicular mode of endodontic therapy in primary teeth is different from that of permanent teeth due to the anatomic variations in primary teeth.
While the technique is discussed in detail later in this chapter, the significant variations in anatomy and the corresponding modifications in the technique are as follows:
- Primary molar roots are fired out and diverged. It demands a wider access cavity preparation than that in the permanent teeth to obtain straight-line access to the root canals.
- The roots are mesiodistally flattened. This requires precision during initial endodontic instrumentation to avoid the breakage of instruments in the canal.
- The root canals are slender and tortuous and make extirpation of pulp in toto relatively difficult. This demands meticulous endodontic instrumentation.
- The apical foramen is relatively larger in diameter when compared to permanent teeth.
- The length of instrumentation is found at 1 mm short of the radiographic apex as compared to 0.5 mm in permanent teeth.
- This is to prevent instrumentation beyond the apex and expulsion of root canal-filling material across the apex.
- The number of lateral canals is more in the apical one-third in the permanent tooth. They are more at the furcation area in the primary tooth. So, dentoalveolar abscess and early periodontal bone rarefaction are observed at the furcation (inter-radicular region) in primary molars rather than at the root apices.
Pulpectomy In Primary Teeth
Pulpectomy In Primary Teeth Rationale
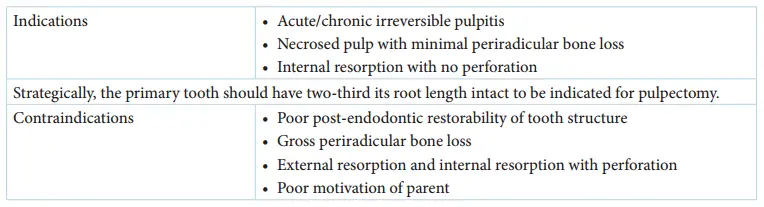
A tooth suggested for pulpectomy must have at least two-thirds of its root length intact.
A pulpectomy is indicated in the following cases:
- Chronic or acute irreversible pulpitis
- Necrosed pulp with minimal periradicular bone loss
- Internal resorption with no perforation
A pulpectomy is contraindicated in the following cases. Extraction of the involved tooth is the alternate treatment when pulpectomy is contraindicated.
- Gross tooth surface loss with poor post-endodontic storability. These include conditions such as
- Caries extending more than 2 mm beyond the gingival margin
- Caries on the pulpal floor/root dentin
- The tooth has less than two-thirds its root length
- Gross periradicular bone loss
- External resorption or internal resorption with perforation
- The poor motivation of the parent
- A pulpectomy is contraindicated in children with cardiac ailments as they are prone to subacute bacterial infective endocarditis
Subacute infective endocarditis occurs when the Streptococcus species produce vegetation in the diseased heart valves. The organism is found in abundance in the infected pulp.
There is a high risk of the disease when very minimal amounts of pulpal fragments are left behind, maybe at the apex or in lateral canals.
To eliminate the infected pulp, extraction is preferred in these cases. Uncooperative behavior of the child is not a contraindication for endodontic therapy.
The child’s behavior has to be appropriately managed to render effective dental care.
Pulpectomy In Primary Teeth Technique
Radical endodontic therapy involves three clinical steps, which are as follows:
- Establishing an access
- A pulpectomy, debridement, and enlargement of the root c ana l
- Obturation of root canal and post-endodontic restoration
Three intraoral periapical radiographs of the involved tooth are essential to achieve proper endodontic therapy. They are as follows:
Pulpectomy In Primary Teeth
1. Pre-operative baseline radiograph:
This diagnostic radiograph is required to detect the number, length, and shape of the roots of the tooth in question.
2. Length determination radiograph:
This radiograph determines the working length for appropriate instrumentation and obturation purpose.
3. Post-obturation radiograph:
This radiograph determines the quality ofobturation.
Establishing An Access
The primary objective is to establish straight-line access to the apical foramen. This has to be achieved with the removal of the least amount of non-carious tissue and the complete removal of carious dentin and enamel. A preoperative IOPA radiograph is a baseline requirement for the establishment of access.
Establishing An Access Procedure
The tooth is anesthetized and isolated with a rubber dam. There is three substeps in this step. They have accessed cavity preparation, pulp extirpation, and establishment of working length.
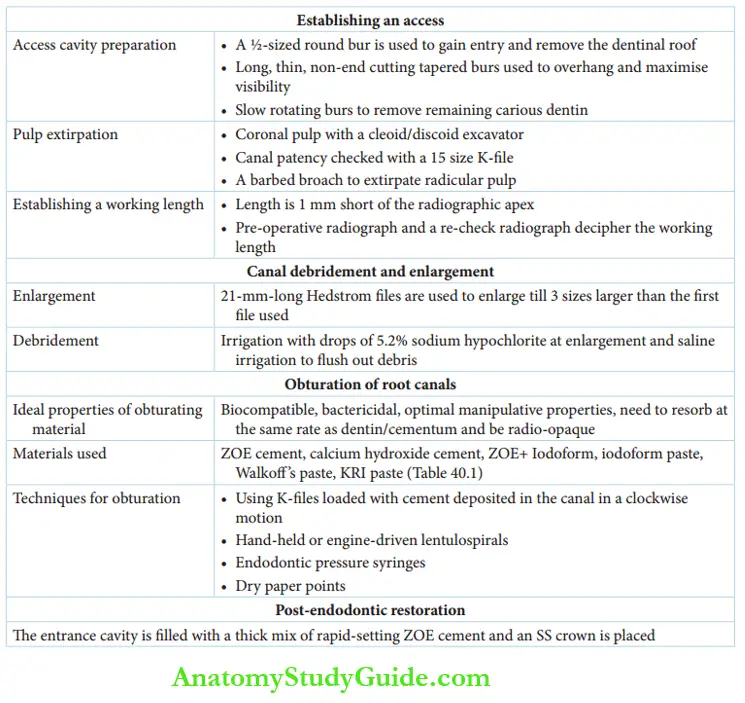
1. Access Cavity Preparation
The access cavity is prepared with a ½-sized round bur and a long, thin non-end cutting tapered fissure bur. The ½-sized bur is used to gain entry into the chamber and remove the entire dentinal roof of the chamber.
The tapered figure bur is used to remove the overhanging dentin and enamel that is overlooking the access cavity. It is rather used to refine the access cavity to maximize the visibility of the chamber.
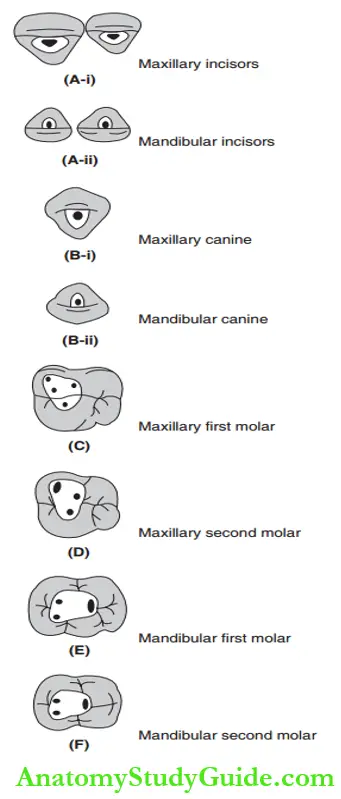
Slow-rotating round burs are used to remove the remaining carious dentin. The location and proportionate sizes of the access cavity on different teeth are depicted.
2. Pulp Extirpation
Visualization of the chamber is primary for pulp extirpation. Endodontics is never a blind procedure and one need not go into a quest searching for the canals. They have to be located with precision and confidence.
On removal of the entire roof, the coronal pulp can be visualized by controlling the bleeding. It is excavated with a cloud/discoid excavator.
This exposes the bleeding points, which indicate the orifice of the root canals. The faint black lines connecting the orifices constitute the dentinal map which also helps in locating the root canals.
The first instrument to be used in the root canal can be the endodontic explorer or a smooth broach or a 15-size K-fie.
This ensures the patency of the canal up to the apical foramen. The extirpation of the pulp is done with a barbed broach.
The size of the barbed broach should be selected in such a way that it is neither loose enough to freely rotate in the canal nor very tight to be bound to the root dentin.
The radicular pulp is best removed in toto rather than in fragments.
3. Establishment Of Working Length
The pre-operative radiograph throws light on the probable length of the root canal. The length up to which the canal has to be debrided and enlarged is called the working length.
It is fixed at 1 mm short of the radiographic apex. Instrumentation beyond the apex or expulsion of root canal filling material beyond the apex can cause periapical irritation and pathology.
Determination of the working length is done by the length determination radiograph.
A K-fie with a stopper at the tip is placed in the canal to take the length determination radiograph.
Necessary addition or reduction of the length can be identified from this radiograph to finalize the working length.
Pulpectomy In Primary Teeth
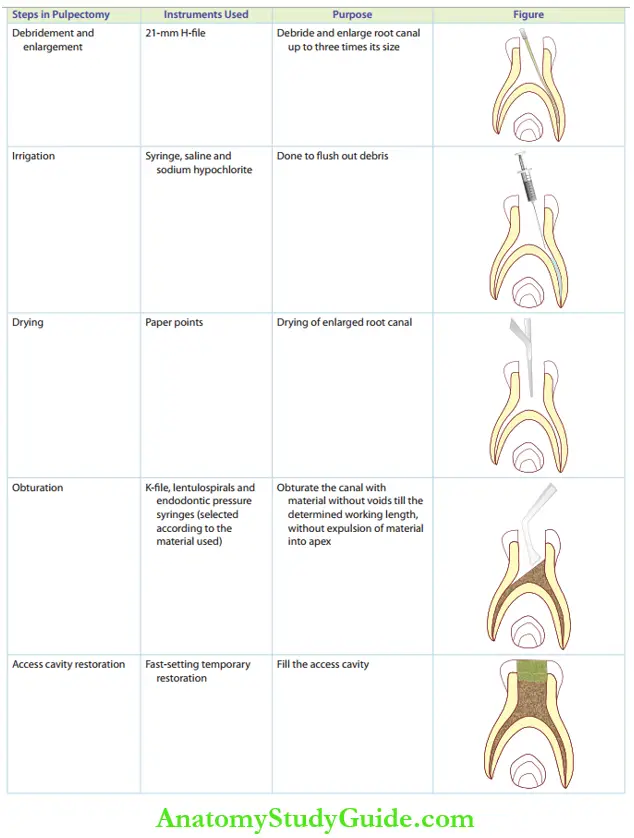
Debridement And Enlargement Of Root Canal
21-mm Hedstrom file or H-fie is the most ideal instrument for the debridement and enlargement of primary root canals. It has very good cutting efficiency but is more prone to breakage than K-fies.
A root canal is copiously irrigated with saline, an inert agent, to flesh out all the debris and dentin shavings. Enlargement is done sequentially from the determined root length to at least three sizes larger than the first H-fie used.
Enlargement is coupled with irrigation of the canal with one or two drops of 5.2% sodium hypochlorite under optimal tissue isolation.
Sodium hypochlorite is a caustic agent. Cautious usage of this root canal irrigant is highly advantageous for the following reasons:
- Bactericidal: It brings down the viable bacterial count to attain sterility of the root canal.
- Tissue sealant: It can probably dissolve the fragments in the lateral canals.
- Surfactant: It improves the efficiency of mechanical enlargement.
Debridement: It flashes out the debris.
The enlarged canal is dried with paper points. It is always tempting to use an air spray to dry root canals. But air drying of root canals can result in surgical emphysema. Soft tissues of the head and neck can tolerate only 5 c.c. of air infusion and not more.
Obturation Of Root Canal
The material used for obturation of the enlarged and cleaned root canal should fulfill the following criteria:
- It has to be biocompatible with alveolar bone and dentinal structures.
- It has to be bactericidal or at least inert.
- It has to resorb the primary dentin and cementum at the same rate.
- It should be packed into the root canal with ease.
- It must have optimal manipulative properties.
- It should be stable with no dimensional changes.
- It must be radiopaque.
The various obturating materials used are as follows:
- Zinc oxide eugenol cement (ZOE)
- Calcium hydroxide cement
- Iodoform paste
- Calcium hydroxide and iodoform paste (Metapex, Vitapex)
- Combination of calcium hydroxide, ZOE, and iodoform cement
- Zinc oxide and iodoform paste
- Camphorate monochloride phenol paste (CMCP) (Walkoffs paste)
- Iodoform and CMCP paste (KRI paste)
Gutta-percha is the obturating material in permanent teeth. It is not used in primary teeth as it does not resorb.
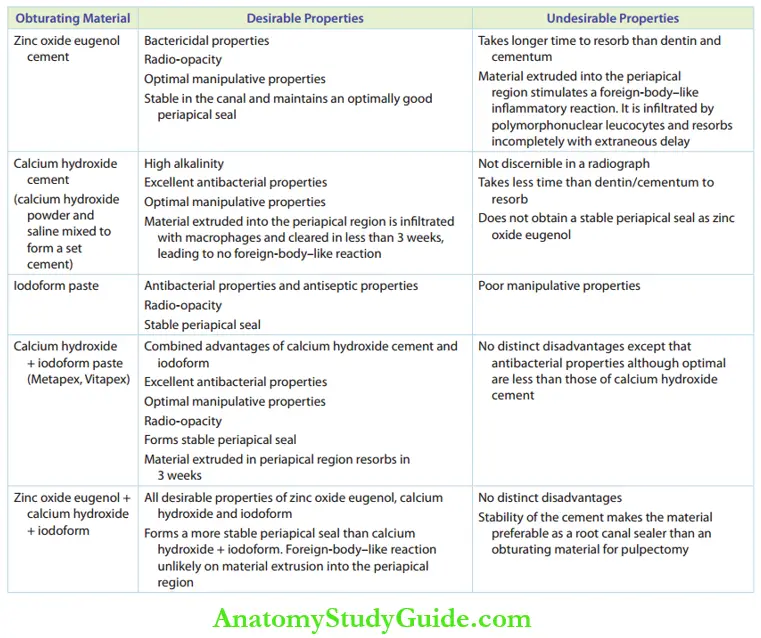
It gives a comparison between the desirable and undesirable properties of obturating materials commonly used in Indian clinical practice.
Comparison of the Properties of Obturating Materials
Obturation Of Root Canal Procedure
The techniques for obturation depend on the instrument used. They can be any of the following:
1. K-fies: They are used when the obturating material is ZOE, calcium hydroxide, or cement combinations.
The size of the K-fie should be smaller than the one used as the final size during enlargement. A thin mix of the material is carried by this small-sized K-fie and deposited into the root canal in a slow clockwise motion.
The maneuver is repeated around three to five times per canal. A thick mix of the cement is kept inside the chamber and gentle pressure is applied with a metal instrument or with a wet cotton pellet.
2. Lentulospirals: These are long, flexible instruments resembling thin coiled wires. These are either hand-held or motor driven.
Lentulospirals can be used for obturating with ZOE, calcium hydroxide, and combination cement.
A thin mix of the material is lifted with the instrument and carried inside the canal. It is rotated in a slow clockwise direction to deposit the cement.
Pulpectomy In Primary Teeth
3. Endodontic pressure syringes: Obturating pastes may be pre-loaded in pressurized syringes.
The syringe comes with a long, narrow beak that can be let in till the middle one-third of the root canal. As the paste is expressed, the syringe is retracted slowly.
Stoppers are fitted on their beaks to calibrate the length of the root canal. A post-obturation IOPA radiograph is essential to detect the quality of obturation.
Good-quality obturation expresses the following three features:
- Homogeneity – the absence of voids in between the filing
- Completeness – filing till the working length
- Appropriateness – no expulsion of material beyond the apex into the periradicular area (over obturation)
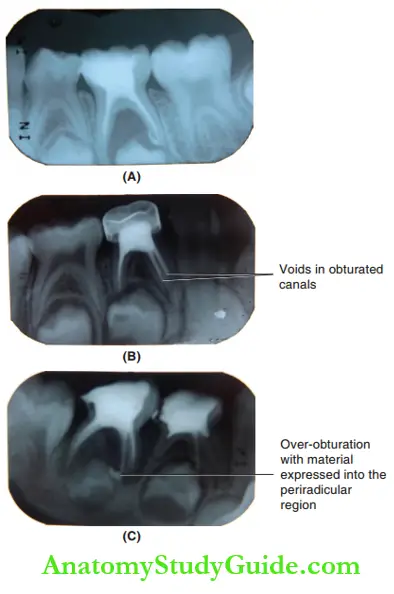
It shows examples of postoperative radiographs.
The obturation material of choice is predominantly influenced by the operator’s comfort level of manipulation of the material.
In the current-day practice, calcium hydroxide and iodoform combination (Metapex, Vitapex) is more widely used followed by zinc oxide eugenol cement.
The former is delivered through a pressure syringe and the latter by a K-fie or a leptospiral. If the child is younger than 5 years old, ZOE may be preferred owing to its better stability than the calcium hydroxide combination.
If the child is older than 7 years, then the calcium hydroxide combination may be sought.
On obturation of the root canals, a thick mix of a fast-setting temporary restoration material (thick mix of rapid-set ZOE) is used to fill the access cavity. The tooth is then rehabilitated with a stainless steel crown.
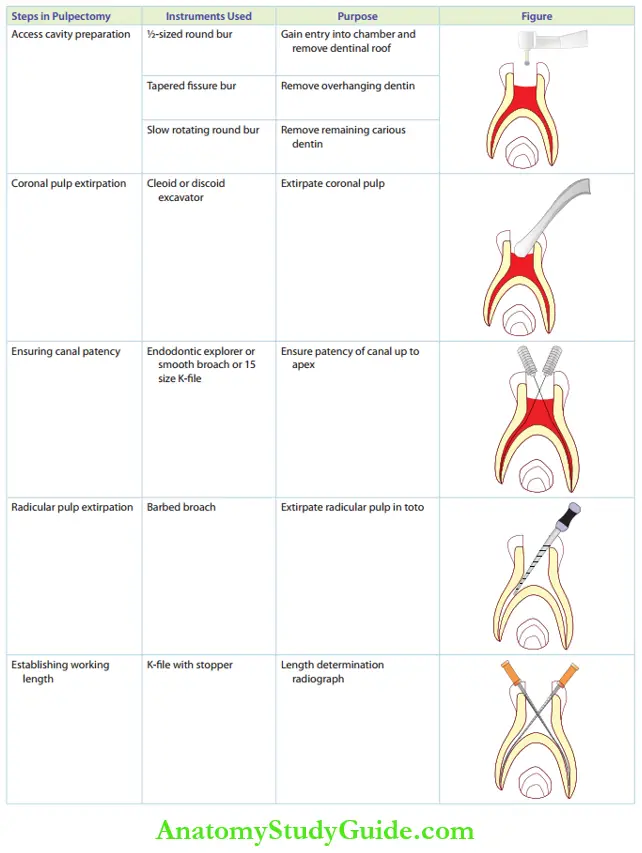
It depicts the steps involved in the pulpectomy of the primary tooth.
Steps in Pulpectomy
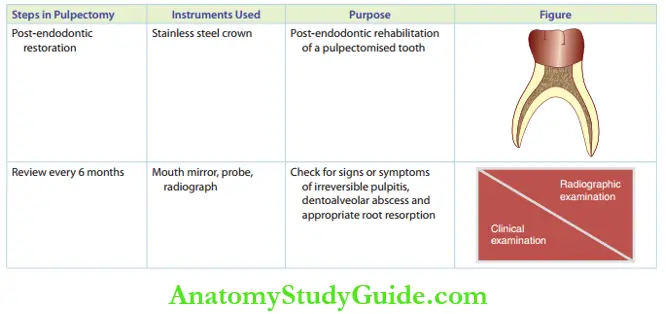
Obturation Of Root Canal Review And Outcome
A pulpectomised tooth has to be reviewed every 6 months. The success of the therapy is determined by the absence of clinical/radiographic signs/symptoms of irreversible pulpitis/dentoalveolar abscess and an appropriate root resorption pattern.
The presence of the aforementioned signs/symptoms, an exaggerated rate of resorption, or delayed exfoliation of the tooth is an undesirable consequence.
When the focal sepsis is not eliminated by pulpectomy, the signs and symptoms may occur or recur. Extraction is required in these cases and subsequent space maintenance is essential.
Pulpless or pulpectomised teeth have a limited surface area subjected to resorption than a normal tooth.
The vascular network around the root apex that induces resorption is less intense around the pulpless teeth. Hence, pulpless teeth usually resorb at a slower rate compared to their normal counterparts.
Pulpectomy In Primary Teeth
A pulpectomy is usually performed in a single visit with post-endodontic rehabilitation. It is converted into a multi-visit procedure in the following situations:
- Dentoalveolar abscess with a weeping canal
- Dentoalveolar abscess with a draining sinus
- An anxious child with a short attention span
- Inability to obtain hemostasis in any of the canals
The following treatment protocol is followed in case of a dentoalveolar abscess (first two situations mentioned in the preceding text):
1. First visit: Access opening and enlargement and debridement are completed at the first visit.
Surgical exploration of the draining sinus with a spoon excavator/curette is performed as it enhances drainage. The tooth is left open for a day.
2. Second visit: At the second visit, a closed dressing is placed.
3. Third visit: At the third appointment, obturation is done and post-endodontic restoration is placed.
In the case of an anxious child or a bleeding canal (third and fourth situations mentioned in the preceding text), pulpectomy can be performed as a two-visit procedure. There is no phase of open dressing in this protocol.
Case Description
1. Case 1
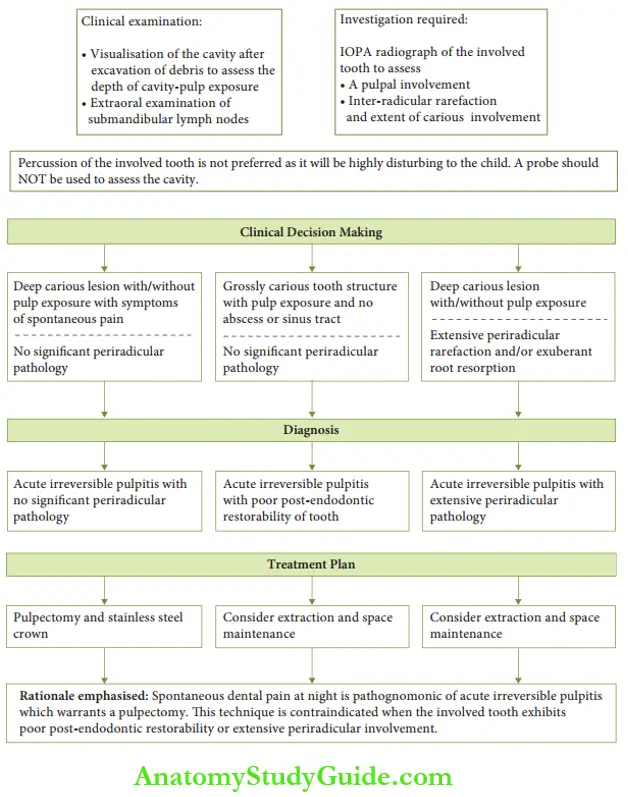
Chief complaint: A 10-year-old male child complains of a deep, wide cavity in the lower back tooth and dull pain in that region for the past few months.
Clinical scenario: A 10-year-old child, whose dental development is coherent with the chronological age, complains of a deep and wide open cavity in the mandibular second primary molar and dull pain for the past few months due to food impaction.
[Baseline data – Mandibular second premolar erupts at 11−12 years of age]
2. Case 2
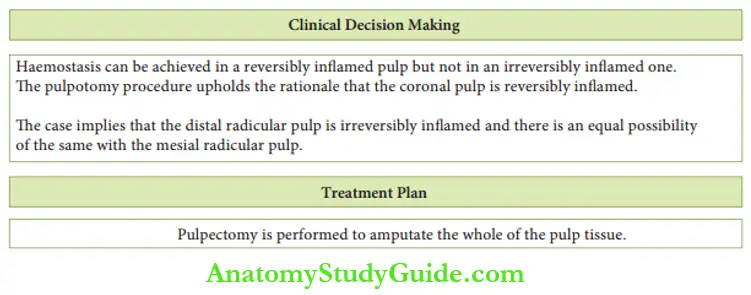
Chief complaint: Bleeding of distal radicular pulp region during pulpotomy of 75 in a 6-year-old female child.
Clinical scenario: During a pulpotomy procedure of tooth 75 in a 6-year-old, after the excision of the coronal pulp, optimal hemostasis could not be attained. the distal radicular pulp exhibits bleeding.
3. Case 3
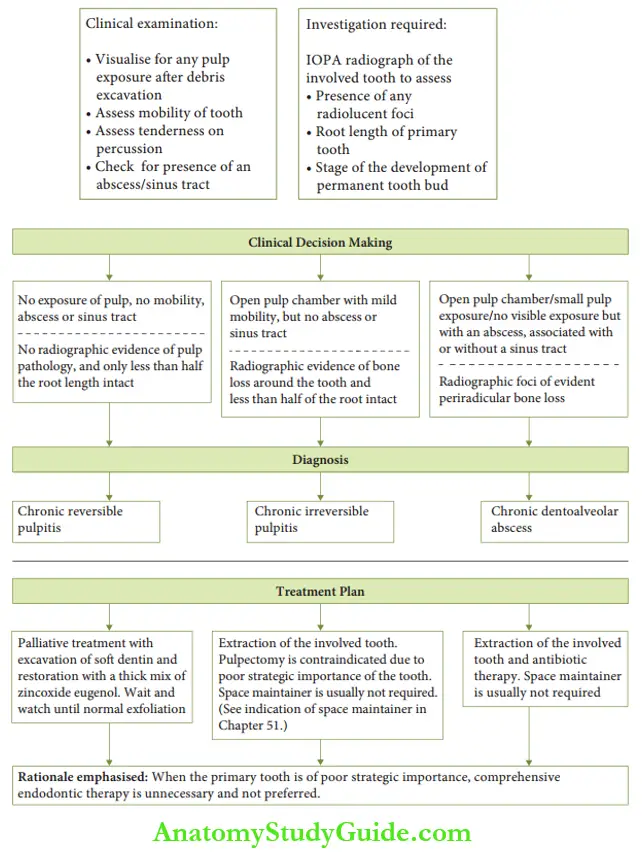
Chief complaint: The parent of a 5-year-old male child complains of disturbed sleep of the child due to pain in the right lower back tooth. The parent adds that the child chews on the le side only for the past 2 days
Clinical scenario: A 5-year-old child is brought with a parental complaint of disturbed sleep last night associated with dental pain on a carious right lower molar. The parent presents a history of the child resorting to chewing only on his le side for the past 2 days.
[Baseline data – Post-endodontic storability and periradicular involvement influence treatment plan]
Pulpectomy In Primary Teeth Summary
1. Radicular endodontic therapy implies a total pulpectomy, enlargement, and cleansing of the root canal system and root canal filling with suitable materials.
2. Rationale
3. Steps in radicular endodontic therapy
Leave a Reply