Acute Infections Sinuses Fistula And Surgical Site Infection
Define and describe the aetiology and pathogenesis of surgical infections.
Table of Contents
The aetiology and pathogenesis of surgical infections Introduction
- Ever since surgery evolved as a speciality, infection and haemorrhage have been two well-known enemies of surgeons. Although many newer antibiotics have come into existence, infection still dominates and is a major cause of morbidity and mortality in patients with ‘benign disease.’
Read And Learn More: General Surgery Notes
- This is the sad outcome of disease complications. Hence, it is important to effectively diagnose and treat infections as early as possible. Common surgical infections and their details are given below.
Cellulitis
- Cellulitis is a spreading subcutaneous inflammation caused by haemolytic Streptococci that produce hyaluronidase and streptokinase. This leads to the spreading of inflammatory exudates in the subcutaneous and fascial planes, resulting in a gross swelling of the affected part.
- Cellulitis spreads quickly in areas of loose subcutaneous tissue, such as the scrotum, or in areas of loose connective and interstitial tissue, such as the face and forearm.
Cellulitis Sources of Infection
- Injury—minor or major
- Graze or scratch or abrasion
- Snakebite, scorpion bite, etc
Cellulitis Precipitating Factors
- Diabetes
- The low resistance of an individual
Cellulitis Common Sites
- Lower limbs
- Face and neck
- Scrotum
Cellulitis Clinical Features
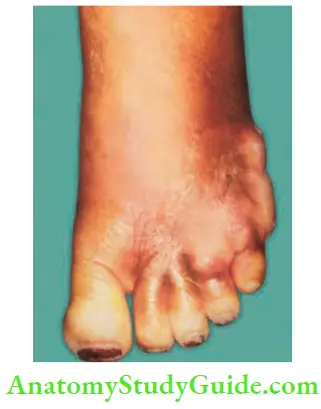
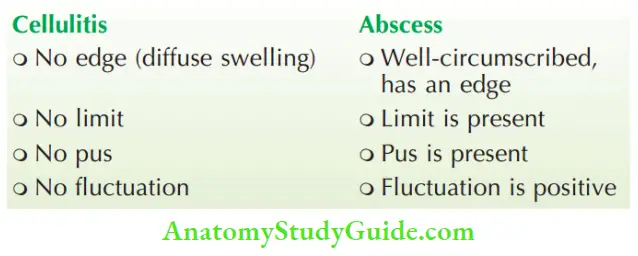
The affected part shows evidence of inflammation such as redness, itching, and diffuse swelling. Skin is stretched and shiny. Pain, fever, and toxaemia follow later. It is differentiated from an abscess by the features mentioned. In untreated cases, suppuration, sloughing, and gangrene may occur.
Cellulitis Treatment
- Bed rest with legs elevated to reduce oedema of legs.
- Glycerine MgSO4 dressing—reduces oedema of the part by osmotic effect.
- Diabetes mellitus, if present, is treated with an injection of insulin given subcutaneously.
- Appropriate antibiotics such as injection cephalosporins have to be given.
- Amoxycillin clavulanate potassium 25–40 mg or kg or day every 12 hours for 5–7 days depending on the severity of the condition.
- Antisnake venom is given in cases of snakebite.
Cellulitis Complications
- Cellulitis may turn into an abscess which needs to be drained.
- Necrotising fasciitis: Certain highly invasive strains of Streptococcus pyogenes may cause extensive necrosis of the skin and subcutaneous tissues, resulting in necrotising fasciitis. This is treated by debridement and skin grafting.
- Toxaemia and septicaemia: Streptococcal toxic shock syndrome may result if exotoxins are produced by the organisms.
- Cellulitis may precipitate ketoacidosis in patients with diabetes mellitus.
Ludwigs Angina
It refers to cellulitis of the submental and submandibular regions combined with inflammatory oedema of the mouth. Virulent streptococcal organisms are responsible for infection surrounding the submandibular region. Anaerobes also play a major role.
Ludwigs Angina Precipitating Factors
- Caries tooth
- Cancer of the oral cavity
- Calculi in the submandibular gland
- Chemotherapy
- Cachexia
- Chronic disease—diabetes Observe 6 Cs
Ludwigs Angina Clinical Features
- Elderly patients presenting with diffuse swelling in the submandibular and submental regions (brawny oedema).
- Oedema of the floor of the mouth, which pushes the tongue upwards and results in difficulty swallowing.
- High-grade fever with toxicity.
- Putrid halitosis is characteristic of this condition.
Ludwigs Angina Treatment
- Rest and hospitalisation.
- Appropriate antibiotics.
- Intravenous fluids (to correct dehydration) and Ryle’s tube feeding.
- If it does not respond to conservative treatment, surgical intervention is recommended.
Ludwigs Angina Surgery (Decompression)
- Under general anaesthesia, a 5–6 cm curved incision is made below the mandible in the submandibular region over the most prominent part of the swelling. The submandibular gland is mobilised, the mylohyoid muscle is divided, and the pus is drained.
- Even if pus is not found, the oedematous fluid comes out, which greatly improves the condition of the patient. The wound is closed with loose sutures after irrigating the cavity with antiseptic agents, and a drainage tube is kept in place.
Ludwigs Angina Complications
- Mediastinitis and septicaemia
- Swelling of the tissues in the floor of the mouth results in elevation of the tongue, as the infection is contained by the mylohyoid. This leads to upper airway obstruction and oedema of the glottis, resulting in stridor.
Lymphangitis
- It is also a nonsuppurative, poorly localised infection caused by streptococci, staphylococci, or clostridia.
- It presents as red painful streaks over the affected lymphatics.
- Filarial infection is a common cause of lymphangitis in coastal India.
- High-grade fever, chills and rigours, and features of systemic inflammatory response syndrome (SIRS) are common.
- Tender, painful lymph nodes in the groin are characteristic of lower limb lymphangitis.
Lymphangitis Treatment
- Rest, elevation, MgSO4, local dressing, antibiotics, and anti-inflammatory drugs.
- Anti-filarial treatment in appropriate cases.
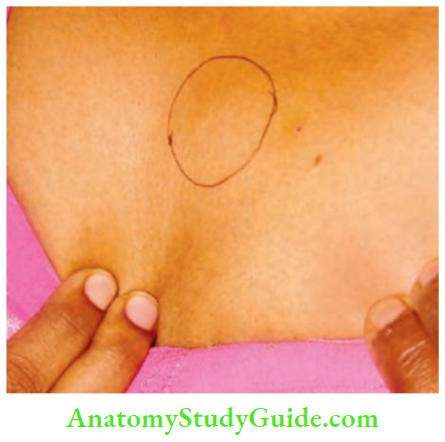
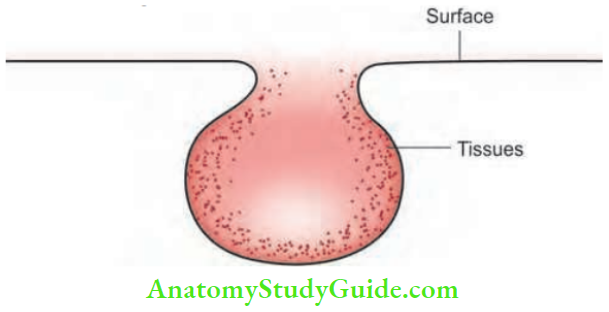
Abscess
An abscess is a localised collection of pus (dead, dying neutrophils and proteinaceous exudate).
Abscess Classification
- Pyogenic abscess: It is the commonest form of an abscess. It can be subcutaneous, deep, or can occur within viscera such as the liver or kidney. In this chapter, pyogenic abscess refers to soft tissue abscess.
- Pyaemic abscess: Occurs due to circulation of pyaemic emboli in the blood (pyaemia).
- Cold abscess: Usually refers to tubercular abscess due to the involvement of either lymph nodes or the spine.
Pyogenic Abscess
It is usually produced by staphylococcal infections. The organisms enter the soft tissue through an external wound (minor or major). It can also be due to cellulitis or haematogenous spread from a distant focus such as tonsillitis or caries tooth.
Pyogenic Abscess Pathophysiology
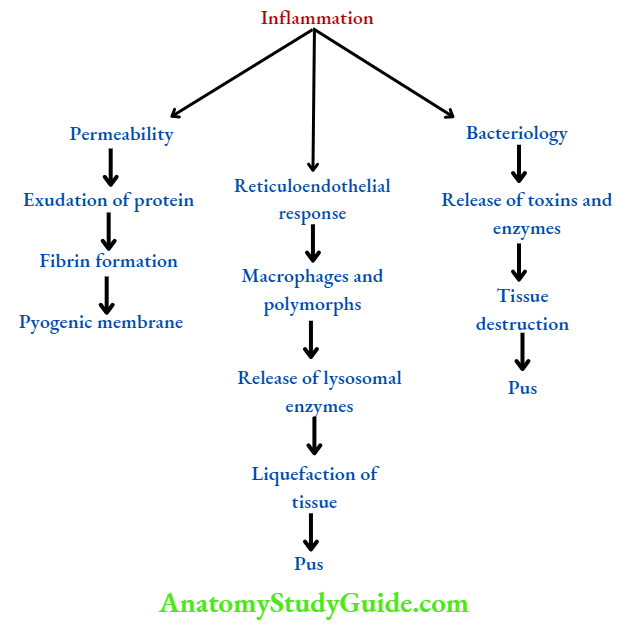
- Following injury, there is inflammation of the part brought about by the organism such as Staphylococcus.
- Pathological events are summarised.
- The end result is the production of pus composed of dead leukocytes, bacteria, and necrotic tissue. The area around the abscess is encircled by fibrin products and it is infiltrated with leukocytes and bacteria. It is called a pyogenic membrane.
Pyogenic Abscess Symptoms
The patient feels ill and complains of throbbing pain at the site, which occurs due to pressure of the pus on the nerve endings. Fever, with or without chills and rigours, may be present.
Pyogenic Abscess Signs
- Calor–heat: The affected part is warmer due to the local rise in temperature.
- Rubor–redness: It is due to inflammation resulting in hyperaemia.
- Dolour–pain: An abscess is extremely tender.
- Tumour–swelling: It consists of pus. It is tensely cystic with surrounding brawny oedema.
- Loss of function: The function of the part is impaired, due to pain.
- Fluctuation: It may be elicited. However, in a deep-seated abscess (for example. breast abscess), it may be negative.
-
- Untreated abscess tends to point spontaneously along the area of least resistance to the nearest epithelial surface, for example. skin, gut, oral cavity.
- However, deep-seated abscesses such as breast abscesses may cause much tissue destruction before pointing.
Pyogenic Abscess Treatment
Incision and drainage (I and D) under general anaesthesia. General anaesthesia is preferred because in the presence of infection, local anaesthesia may not act and it would be difficult to break all the loculi of an abscess without causing pain.
Pyogenic Abscess Procedure
- A stab incision is made over the most prominent (pointing) part of the abscess. The pus which comes out is collected and sent for culture and sensitivity.
- A sinus forceps or a finger is introduced within the abscess cavity and all the loculi are broken down.
- Fresh oozing of the pus is an indication that the procedure is complete. The abscess cavity is irrigated with saline or a mild antiseptic agent like iodine solution.
- The cavity, if large, may need to be packed with roller gauze dipped in an iodine solution, which is removed 1–2 days later. Roller gauze packing prevents premature closure of the skin.
- Thereby facilitating healing from the depth of the cavity through granulation tissue formation. With appropriate antibiotics and proper dressings, the wound heals within 5–7 days.
- The antibiotic of choice is cloxacillin for staphylococcal abscesses. Dosage: 500 mg 6th hourly for 5–7 days.
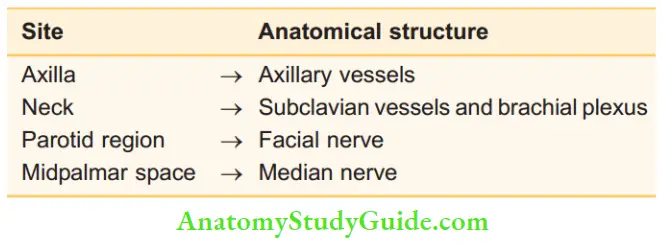
- Modified Hilton’s method for I and D. This method is followed if the abscess is situated in the vicinity of important anatomical structures like vessels or nerves.
- The skin and superficial fascia are incised (instead of a stab incision), and the abscess is opened by sinus forceps to avoid damage to vital structures.
Pyogenic Abscess Differential Diagnosis
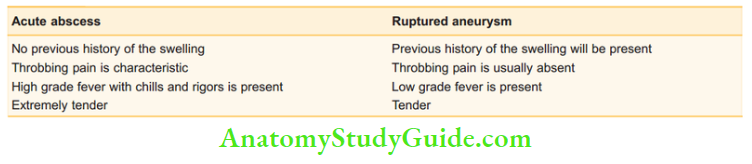
1. A ruptured aneurysm may present as a subcutaneous abscess with pain, redness, local rise of temperature, and sometimes even leukocytosis.
- A ruptured vertebral artery aneurysm in the posterior triangle and a popliteal artery aneurysm in the popliteal fossa have been incised, mistaking them for an abscess.
- Caution: When in doubt, aspirate with a wide bore needle before incising an abscess.
2. Soft tissue sarcoma in the thigh may be confused for a deep-seated abscess. However, throbbing pain, high-grade fever with chills and rigours, and short duration of the swelling clinch the diagnosis of an abscess.
Pyogenic Abscess Antibiotic
- It is an antibiotic-induced swelling (oma). Once an abscess is formed, antibiotics seldom affect a cure but partially sterilise the pus. Antibiotics also produce fibrosis, resulting in thickening of the abscess wall.
- Clinically, this may result in a hard lump. Common sites of antibioma are the breast, thigh, and ischiorectal fossa. Antibiotics in the breast may mimic carcinoma of the breast.
Pyaemic Abscess
This is due to pus-producing organisms in the circulation (pyaemia). It is the systemic effect of sepsis. It commonly occurs in diabetics and in patients receiving chemotherapy and or radiotherapy.
Pyaemic abscess is characterised by the following features:
- They are multiple
- They are deep-seated
- There is minimal tenderness
- There is no local rise in temperature
Hence, it is called a nonreactive abscess to differentiate it from a pyogenic abscess. This is treated by multiple incisions over the abscess site and drainage (like a pyogenic abscess) with antibiotic cover.
- Leptospirosis is a zoonosis caused by infected urine of cattle, dogs or rats. It causes severe myalgia/myositis of thigh muscles and thus can be confused for pyaemic abscesses. High-grade fever is also a feature.
- When in doubt ask for an ultrasound. A severe form of leptospirosis is called Weil’s disease. It can cause multiorgan failure and death.
Cold Abscess
Even though this is a chronic abscess due to a chronic disease (tuberculosis), for the completeness of the chapter on abscess and for the convenience of reading, it is discussed here.
- Cold abscess refers to an abscess that has no signs of inflammation. Usually, it is due to tuberculosis, for example., following tubercular lymphadenitis or due to tuberculosis of the spine.
- However, other chronic diseases like leprosy, actinomycosis, and Madura’s foot also produce abscesses that are ‘cold’ in nature. In this chapter, cold abscess due to cervical tubercular lymphadenitis is discussed.
Cold Abscess—Causes
- Tuberculosis (main cause)
- Actinomycosis
- Leprosy
- Madura’s foot
Cervical Tuberculous Lymphadenitis
It is the most common form of extrapulmonary tuberculosis.
- Tuberculous infections of the cervical lymph nodes—often termed scrofula and king’s evil—are typically caused by tuberculous mycobacteria, but may also be caused by non-tuberculous mycobacteria.
- It is seen in endemic areas and in immunocompromised individuals.
- Lymph node tuberculosis constitutes 20–40% of extrapulmonary tuberculosis. It is more common in children and women and in Asians and Pacific Islanders.
- The disease may be caused by Mycobacterium tuberculosis, atypical mycobacteria, or Mycobacterium bovis.
Cervical Tuberculous Lymphadenitis Aetiopathogenesis
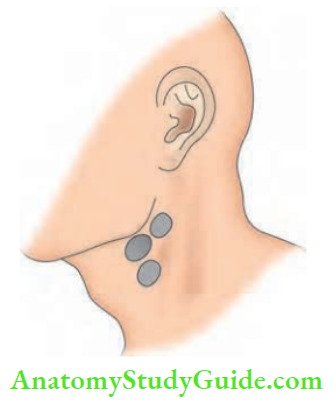
In 80% of the cases, mycobacteria pass through tonsillar crypts and affect the tonsillar node or jugulodigastric group of nodes in the anterior triangle of the neck.
- In 20% of the cases, lymph nodes in the posterior triangle are affected due to adenoid involvement.
- Rarely, infection can spread from tuberculosis at the apex of the lung. Organisms directly penetrate Sibson’s fascia (suprapleural membrane) and may cause enlargement of the supraclavicular node.
- Other lymph nodes in the neck, such as the preauricular and submandibular nodes, may also be affected.
- Tuberculous bacilli survive within macrophages and release a toxin called tuberculosis necrotising toxin (TNT), which causes host cell death.
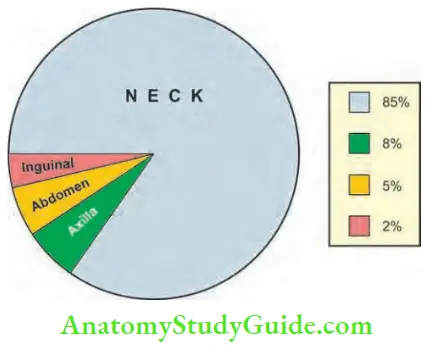
- In general, the incidences of lymphadenopathy at various sites are shown.
Cervical Tuberculous Lymphadenitis Pathological Types
- Caseating type: The most common type seen in young adults.
- Hyperplastic type: Lymph nodes show a marked degree of lymphoid hyperplasia. Least caseation is seen in patients with good body resistance.
- Atrophic type: Seen in elderly patients. Lymphoid tissue undergoes degeneration. Glands are small with early caseation. A few lymph nodes may show scattered calcifications.
Cervical Tuberculous Lymphadenitis Clinical Features
Common in the age group of 11–30 years.
- HIV-immunocompromised disease is a strong risk factor for developing tuberculous infections.
- Tuberculous lymphadenitis presents as a gradually increasing painless swelling of one or more lymph nodes and lasts from a few weeks to a few months. Multiple sites may be involved.
- Systemic symptoms such as chills, fever, weight loss, fatigue, and night sweats are common, especially in those with extensive disease. Seen in about 40% of patients.
- In tuberculosis, interleukin-1(IL-1) and interleukin-6 (IL-6) are released, resulting in high-grade fever. However, this effect is somewhat counteracted by cortisol levels (which are also increased), resulting in low-grade fever.
Stages of Tuberculous (TB) Lymphadenitis
1. Stage of Lymphadenitis
- Common in young adults between 20 and 30 years of age.
- Upper anterior deep cervical nodes are enlarged.
- Nontender, discrete, mobile, firm lymph nodes are palpable.
2. Stage of Periadenitis or Stage of Matting
- Results due to capsular involvement
- Nodes move together—matting
- Firm, non-tender
- Matting is pathognomonic of tuberculosis
- Other rare causes of matting are chronic lymphadenitis and anaplastic variety of lymphoma.
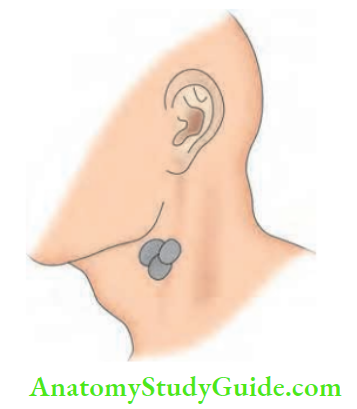
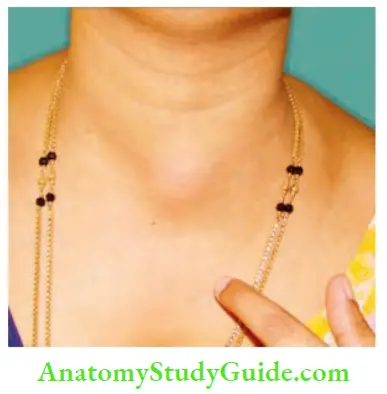
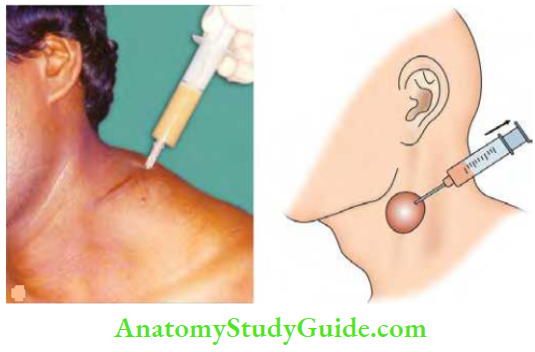
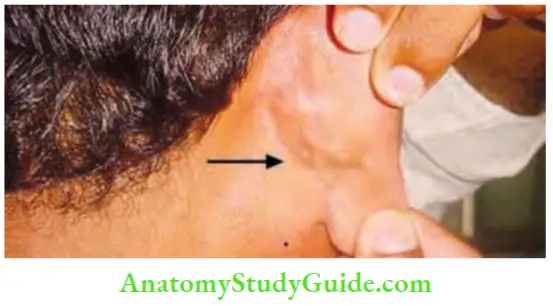
3. Stage of Cold Abscess
- It occurs due to caseating necrosis of the lymph nodes, which results in a fluctuant swelling in the neck. Clinical features of a cold abscess in the neck are:
- No local rise in temperature, tenderness, or redness
- Soft, cystic, fluctuant, transillumination—negative swelling.
- It becomes less prominent on the sternocleidomastoid contraction test, indicating that it is deep to the fascia.


Tuberculous (TB) Lymphadenitis Differential Diagnosis
Branchial cysts may be confused for cold abscess in the anterior triangle. Cold abscess is of a shorter duration and may present with other lymph nodes in the neck. Branchial cyst, being a congenital swelling, is of a longer duration.
Tuberculous (TB) Lymphadenitis Treatment of Cold Abscess
- Nondependent aspiration using a wide bore needle to avoid a persistent sinus.
- A wide bore needle is preferred because the caseous material is thick.
- Incision and drainage should not be done as they cause persistent tuberculous sinus.
- Antituberculous treatment is administered.
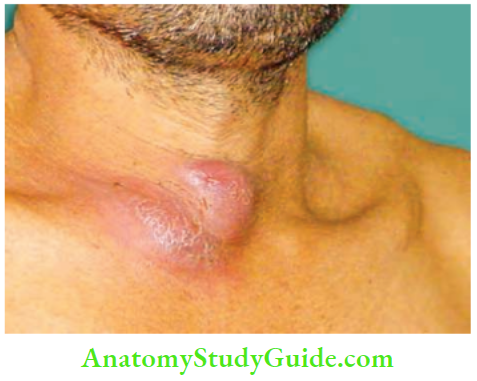
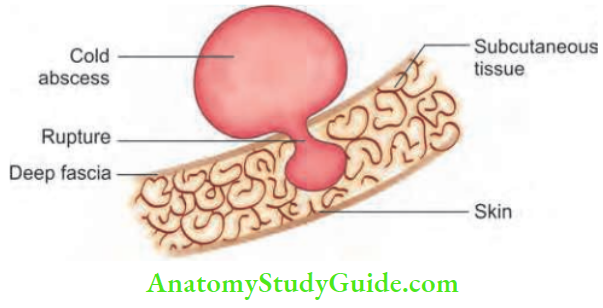
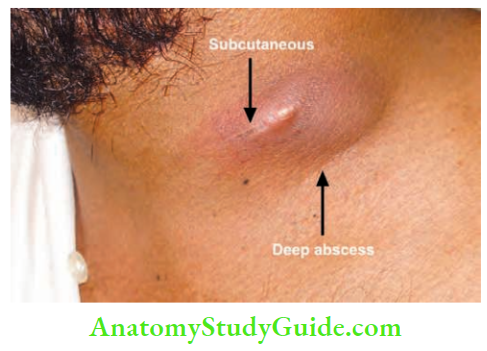
4. Stage of Collar Stud Abscess
It results when a cold abscess deep to the deep fascia ruptures through the deep fascia and forms another swelling, which is fluctuant, in the subcutaneous plane.
Cross fluctuation test may be positive. It is treated like a cold abscess.
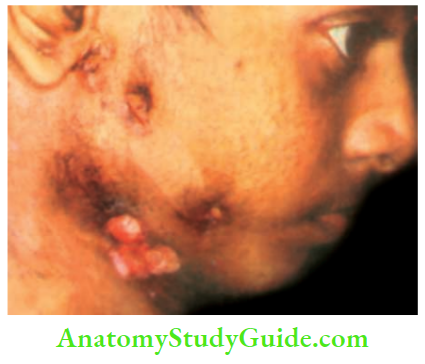
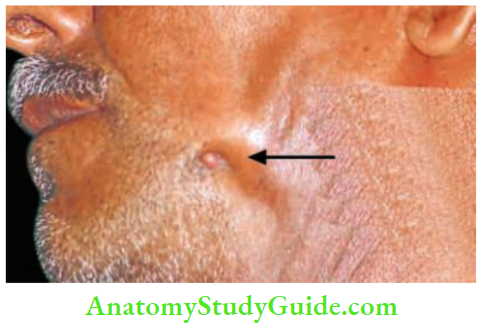
5. Stage of Sinus
- A sinus is a blind tract leading from the surface down into the tissues.
- It occurs when a collar stud abscess ruptures through the skin.
- In India, the tubercular sinus is the most common sinus in the neck.
- It is common in young females. There may be multiple sinuses.
- Tubercular sinuses have a wide opening.
- The sinus resembles an ulcer with an undermined edge.
- There is no induration.
- Surrounding skin is hyperpigmented and sometimes bluish in colour.
- A group of lymph nodes is usually palpable underneath the sinus.
Tuberculous (TB) Lymphadenitis Tuberculosis Of Intrathoracic Nodes
- Occurs in about 25% of all TB lymphadenitis cases.
- Pressure on the bronchus gives rise to atelectasis and lung infection.
- Pressure on the oesophagus causes dysphagia and oesophagotracheal fistula.
- Retroperitoneal nodes may give rise to chylous ascites and chyluria.
- HIV infection and lymph node TB.
HIV Infection and Lymph Node Tuberculosis
- It is more common than lymphoma and sarcoma
- Patients are male and older
- Multiple sites are more commonly affected
- Disseminated disease (virulent) may be seen
- Nodes can be tender
- Weight loss is more common
TB-IRIS: Tuberculosis-associated Immune Reconstitution Inflammatory Syndrome. This is seen in patients with tubercular lymphadenitis on retroviral therapy.
- It manifests as deterioration of a treated infection or as a new presentation of a previously subclinical infection. Thus, lymph nodes may persist or may become bigger.
- It occurs due to an antigenic response caused by the bactericidal action of antitubercular drugs.
- It needs only reassurance and anti-inflammatory drugs.
- A short course of steroids may be needed if pressure symptoms are present.
- However, if lymph nodes do not respond and are increasing, a biopsy should be done to rule out lymphoma.
Tuberculous (TB) Lymphadenitis Investigations
TB lymphadenitis is most commonly diagnosed by histopathology. Other investigations used for diagnosis are acid-fast bacilli (AFB) smear or Ziehl-Neelsen (ZN) staining and culture of lymph node material. Collection of samples or material for examination may be done by either:
- Fine needle aspiration, or
- Excisional lymph node biopsy.
1. Fine needle aspiration (FNA): It is considered as the first line of evaluation of suspected tuberculous lymphadenopathy. FNA had good sensitivity and specificity (77% and 93%, respectively). Materials
Obtained should be tested for:
- AFB smear microscopy (ZN staining or fluorescence microscopy)
- Mycobacterial culture with drug susceptibility testing
- Cytology
- Nucleic acid amplification testing (Xpert MTB/RIF) and line probe assays.
2. Excisional biopsy: This allows for a larger sample to be collected and has a higher diagnostic yield than FNA. Because a sinus tract may form if an incisional biopsy is performed, an excisional biopsy is preferred. Materials obtained should be tested for:
- AFB smear microscopy (ZN staining or fluorescence microscopy)
- Mycobacterial culture with drug susceptibility testing
- Histology: TB may be confirmed if epithelioid cell granulomas and caseation are seen. The chance of diagnosing TB is increased if multinucleated cells are present.
- In patients living with HIV, these typical granulomas are usually not found, as T cells (which are essential for their formation) are affected.
- Nucleic acid amplification testing (Xpert MTB/RIF) and line probe assays.
- Histopathology findings of caseating granulomas, Langhans giant cells and foreign body giant cells are suggestive of TB.
- Nucleic acid amplification testing (NAAT)—CBNAAT (cartridge-based NAAT) or Xpert MTB or RIF helps in both the diagnosis of TB and in the detection of rifampicin resistance.
- NAAT identifies the complex nucleic acid of Mycobacterium tuberculosis but cannot assess the viability of the bacteria.
- It cannot be used for monitoring the response to the treatment as it identifies the complex nucleic acid of dead Mycobacterium tuberculosis bacilli as well.
- Line probe assays are molecular tests which make use of PCR to evaluate drug susceptibility to isoniazid, rifampicin, aminoglycosides, and fluoroquinolones.
- Mycobacterial culture is the gold standard for diagnosis. It also helps in performing drug susceptibility testing (DST) on MTB complex growth, which may be used for decision-making by the treating physician or surgeon.
- Tuberculin skin test (Mantoux test) is a delayed-type hypersensitivity reaction to antigens of Mycobacterium tuberculosis. The reagent used is protein purified derivative (PPD) which is injected intradermally.
- The induration is measured between 48 and 72 hours. An induration >10 mm is considered to be reactive and is suggestive of M. tuberculosis infection. However, it does not indicate active disease.
- A 5–9 mm induration is an intermediate response and may be attributed to BCG vaccination, M. tuberculosis, or atypical mycobacterial infections. An induration <4 mm is considered negative.
- Interferon-gamma release assays (IGRAs) may be used in place of the Mantoux test for diagnosing TB infection.
- Imaging:
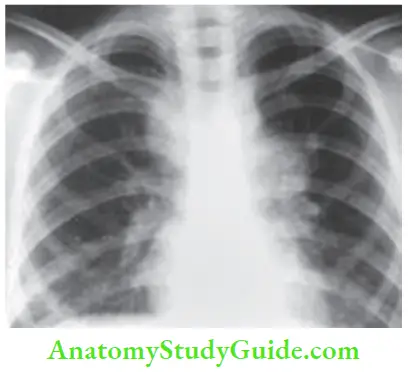
- Chest X-ray should be done in all patients suspected of lymph node tuberculosis, as the lungs are the portal of entry for bacilli.
- It may show features suggestive of active pulmonary tuberculosis or apical fibrosis suggesting previous exposure to tuberculosis. Positive chest radiograph abnormalities are more commonly seen in patients living with HIV.
- HRCT scan of the thorax or abdomen may be done if mediastinal or abdominal lymphadenopathy is suspected.
- Ultrasound scanning of the suspected anatomical site may be done to confirm the lymph node swelling, and abscess and also helps in guided FNA.
- EBUS (endobronchial ultrasound) helps in localising the mediastinal lymph node and in guiding transbronchial needle aspiration (FNA) of mediastinal lymph nodes (mediastinoscopy or CT-guided FNA/biopsy are preferred if mediastinal lymph nodes are not accessible through EBUS).
Definitions of Diagnosis (INDEX TB Guidelines)
- Bacteriologically Confirmed LNTB Cases (Lymph Node TB)
- A patient with symptoms and signs of LNTB who has at least one of the following:
- Positive microscopy for AFB on examination of lymph node fluid or tissue
- Positive culture of Mycobacterium tuberculosis from lymph node fluid or tissue
- Positive validated PCR-based test (such as Xpert MTB/RIF)
Clinically Diagnosed LNTB Case
A presumptive LNTB patient who undergoes diagnostic testing and has all of the following:
- Negative microscopy, negative culture, and negative PCR-based tests
- No other diagnosis to explain the clinical features
- Strongly suggestive evidence of LNTB by radiological findings, histopathological findings, or clinical course
Clinically Diagnosed LNTB Case Treatment
Antitubercular drugs are the cornerstone of treatment for LNTB. Isoniazid (H), rifampicin (R), pyrazinamide (Z), ethambutol (E) and streptomycin (S) are the 1st line antitubercular drugs and are very important in treating drug-sensitive tuberculosis.
Clinically Diagnosed LNTB Case Regimen
IP (intensive phase) of 2 months of HRZE followed by CP (continuation phase) of 4 months of HRE in new cases (patients without a history of previous exposure to ATT).
Treatment Of Drug-Resistant Cases
MDR-resistance to Rifampicin and Isoniazid
- IP (intensive phase): 6–9 months of kanamycin, levofloxacin, pyrazinamide (Z), ethambutol (E), cycloserine, and ethionamide.
- CP (continuation phase): 18 months of levofloxacin, ethambutol (E), cycloserine, and ethionamide.
- If sensitive to isoniazid and resistant to rifampicin, isoniazid can be added to the above regimen in both phases.
- If resistant to isoniazid and sensitive to rifampicin (isoniazid monoresistance), treat with:
- IP: 3–6 months of kanamycin, levofloxacin, rifampicin (R), pyrazinamide (Z), and ethambutol (E).
- CP: 6 months of levofloxacin, rifampicin (R), pyrazinamide (Z), and ethambutol (E).
- Individual monoresistance should be treated according to drug sensitivity testing results.
HIV Co-Infection
In India, the most common opportunistic infection related to HIV is tuberculosis. Patients with latent tuberculosis are more prone to develop tuberculosis in their lifetime if they become infected with HIV.
- Extrapulmonary tuberculosis is more common in patients living with HIV (PLHIV) than in non-HIV-infected patients. HIV has been accepted by the WHO as the defining criteria for clinical stage 4 disease diagnosis. Tuberculous lymphadenopathy often suggests disseminated tuberculosis in PLHIV.
- In PLHIV, lymph node enlargement is usually symmetrical and multiple. Significant mycobacterial load is often reported in PLHIV. Chest X-ray findings of pulmonary tuberculosis are a common association with tuberculous lymphadenitis in PLHIV.
- Response to treatment with antitubercular treatment is similar to HIV-negative patients; however, recurrence and death are higher in PLHIV.
HIV Coinfection Incidence Of Different Lymph Node Sites Involved
The cervical group of lymph nodes is the most common group of lymph nodes involved (63.3%), followed by the mediastinal lymph nodes (26.7%) and the axillary lymph nodes (8.3%).
- Cervical and mediastinal lymph nodes together constitute around 70% of the cases of TBLN. Axillary, mesenteric, hepatic, periportal, and inguinal lymph nodes constitute the rest.
- In descending order, the incidence of involvement of lymph nodes is cervical (64.9%), axillary (27%), and mediastinal (8%) nodes.
- TBLN may involve single or multiple sites. When all TB lymphadenopathies are analysed, the incidence is as follows: Only cervical nodes (63.6%), and cervical + axillary + inguinal nodes (15.1%).
- Only hilar nodes (6%), only inguinal nodes (3%), axillary + inguinal nodes (3%) and axillary + abdominal + hilar lymph nodes (3%).
HIV CoInfection Role Of Surgery In Tuberculous Lymphadenitis
- Biopsy: Lymph node biopsy, wedge biopsy from the edge of the sinus.
- Aspiration: Non-dependent aspiration of cold abscess and pus should be sent for AFB staining and Ziehl-Neelsen (ZN) staining.
- Excision of lymph nodes if they persist in spite of antitubercular treatment.
- Excision of sinus wall along with the tract.
Other Special Types Of Pyogenic Infections
Boil
- This is also called a furuncle. It is a hair follicle infection caused by Staphylococcus aureus or a secondary infection of a sebaceous cyst.
- It starts with a painful indurated swelling with surrounding oedema. After about 1–2 days, softening occurs in the centre and a pustule develops which bursts spontaneously and discharges pus.
- Necrosis of subcutaneous tissues produces a greenish slough. The skin overlying the boil also undergoes necrosis. Hence, the boil is included under acute infective gangrene.
- Furuncle of the external auditory meatus is a very painful condition because of the rich nerve supply of the skin. Pain is also due to the dense adherence of the skin to the perichondrium (there is no subcutaneous tissue).
Treatment Of Boil
Incision and drainage with excision of the slough. Antibiotic cloxacillin is given. Diabetes, if present, is treated.
Complications of Boil
- Necrosis of the skin.
- Pyaemic abscess and septicaemia.
- Cavernous sinus thrombosis due to a boil on the face or a stye on the eyelid.
Carbuncle
The name is derived from Latin: Carbunculus, a small coal.
- This is an infective gangrene of the subcutaneous tissue caused by Staphylococcus aureus. It commonly occurs in diabetic patients Patients with poor immunity or those undergoing radiotherapy may also develop carbuncle.
- Sites: Nape of the neck is the most common site, followed by the back and shoulder region. The skin of these sites is coarse and has poor vascularity.
- Carbuncle can also occur in kidneys.
Carbuncle Staphylococcal Infections of Surgical Importance
- Boil
- Carbuncle
- Breast abscess
- Parotitis
- Osteomyelitis
Carbuncle Pathology
- The initial lesion is similar to a boil in the form of a hair follicle infection with perifolliculitis. Since the majority of patients are diabetic, the infection takes a virulent course and results in subcutaneous fat necrosis, giving rise to multiple abscesses.
- These abscesses are intercommunicating and open to the exterior by multiple sieve-like openings. This appearance is described as cribriform appearance which is the pathognomonic of a carbuncle.
Carbuncle Clinical Features
- Typically, the patient is a diabetic.
- Severe pain and swelling in the nape of the neck.
- Constitutional symptoms, such as fever with chills and rigours, are severe.
- The surface is red and angry-looking like red hot coal.
- The surrounding area is indurated.
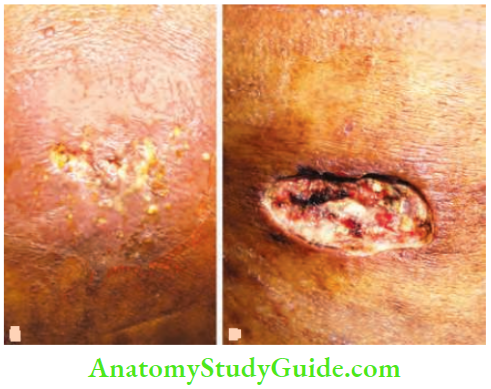
- Later, skin over the centre of the carbuncle softens and peripheral satellite vesicles appear, which rupture and discharge pus, giving rise to a cribriform appearance.
- The end result is the development of a large crateriform ulcer with a central slough.
Carbuncle Complications
- Worsening of diabetic status, resulting in diabetic ketoacidosis.
- Extensive necrosis of the skin overlying the carbuncle. Hence, it is included under acute infective gangrene.
- Septicaemia, toxaemia.
Carbuncle Treatment Summary of Carbuncle
- Caused by Cocci
- Abscesses Communicating
- Red hot like Coal
- Appearance Cribriform, Crateriform ulcer
- Gangrene Cutaneous (subcutaneous)
- Drug of choice Cloxacillin
- Diabetes Control
- Incision Cruciate
Control diabetes, preferably with injectable insulin.
- Appropriate parenteral antibiotics are given till complete resolution occurs. Most strains of Staphylococcus aureus are sensitive to cloxacillin, flucloxacillin, erythromycin, and some cephalosporins.
- However, methicillin-resistant Staphylococcus aureus (MRSA) bacteria are resistant to these drugs. They are sensitive only to the expensive drug vancomycin, which has to be given intravenously.
- Improve the general health of the patient.
- If the carbuncle does not show any softening or shows evidence of healing, it is not incised and may be left open to the exterior. Alternatively, saline dressings may be applied to reduce oedema. Complete resolution may take place within 10–15 days.
- Surgery is required when there is pus. A cruciate incision is preferred because of the multiple abscesses and extensive subcutaneous necrosis.
- Edges of the skin flap are excised, the pus is drained, loculi are broken down, the slough is excised, and the cavity is irrigated with antiseptic agents. Like a pyogenic abscess, a wound heals with granulation tissue from the depth.

Erysipelas
- It is an acute inflammation of the skin and subcutaneous tissue associated with severe lymphangitis. The causative organism is Streptococcus pyogenes. The precipitating factors are malnourishment, chronic diseases, etc. Thus, children and old people are commonly affected.
- Infection sets in after a small scratch or abrasion and spreads very rapidly, resulting in toxaemia. Sites: Face, eyelids, scrotum, and in infants, the umbilicus.
Erysipelas Clinical Features
- Rose-pink rash with a raised edge (on palpation) and a buttonhole consistency.
- Vesicles appear later and rarely become pustular.
- Oedema of the eyelids or scrotum, depending on the site.
- Features of toxaemia
- When it occurs over the face, it involves the pinna because the erysipelas is basically a cuticular lymphangitis. This is described as Milian’s ear sign positive, which is used to differentiate cellulitis of the face from facial erysipelas.
- In cellulitis of the face, the pinna does not get involved because of the close adherence of the skin and cartilage.
Erysipelas Complications
- Toxaemia and septicaemia
- Gangrene of the skin and subcutaneous tissue
- Lymphoedema of the face and eyelids due to lymphatic obstruction and fibrosis
Erysipelas Treatment
Injection crystalline penicillin 10 lakh units 6th hourly IM/IV for 5–10 days.
Chronic Abscess
It occurs when the initial infective process or cause is not fully identified and properly treated.
Chronic Abscess Sites
Foot, hand, thigh, etc.
Chronic Abscess Causes
1. Foreign bodies: These are the most common causes of a chronic abscess. There is a typical history of recurrent swelling discharging pus. Wooden pieces impacted in the thigh or in the foot are common. Infection of the synthetic mesh used in hernial repair is another example.
2. Dead tissue: As it occurs in diabetic patients.
3. Pilonidal sinus: This condition gives rise to recurrent abscesses. There is a typical history of pain and swelling that ruptures and is followed by spontaneous recovery. However, the sinus persists.
4. Chronic disease: Tuberculosis is one of the causes. All features of a cold abscess may be present but in an unusual location.
Chronic Abscess Clinical Notes
- A 40-year-old female presented with swelling of the left thigh of 8 months duration. There were no signs of inflammation. FNAC was inconclusive. During surgery, a localised abscess with a thick wall and fleshy tissue was removed. The final report was a tubercular abscess.
- There was no evidence of tuberculosis anywhere in the body. Tuberculosis may present in different forms, as seen in this case. Detailed investigations were unable to reveal any evidence of pulmonary tuberculosis.
Necrotising Fasciitis
It is a spreading, destructive, invasive infection of the skin and soft tissues, which includes the deep fascia, but relatively spares muscle. Risk factors are given
Necrotising Fasciitis—Risk Factors
- Diabetes mellitus, malnutrition
- Obesity, corticosteroids
- Immune deficiency
Necrotising Fasciitis Common Sites
It is common in the lower extremities. Other sites are the genitalia, groin, and lower abdomen. In these places, it is comparable or similar to gangrene and is called Meleney’s gangrene.
Necrotising Fasciitis Types and Microorganisms
- Type 1 necrotising fasciitis : Polymicrobial: It is due to a synergistic combination of anaerobes and coliforms or nongroup A streptococci— Very often, there is no history of injury when it occurs in the lower limbs.
- Type 2 necrotising fasciitis : Monomicrobial: It is due to group A β-haemolytic streptococci. This has been referred to as a flesh-eating disease.
- Specific Features of Type 2 Necrotising Fasciitis
- Caused by Streptococcus pyogenes
- Occur in young healthy people
- Minor abrasions, lacerations may be a precipitating factor
- Severe systemic illness with multiorgan failure streptococcal toxic shock syndrome
- Specific Features of Type 2 Necrotising Fasciitis
- Type 3 necrotising fasciitis: Gas gangrene due to clostridium.
- Type 4 necrotising fasciitis (others): Fungal (candida) and vibrio species-marine organisms.
Necrotising Fasciitis Pathogenesis:
- Numerous cytokines, such as IL-1, IL-6, and TNF-α, are released due to inflammation caused by M proteins, which are produced by Streptococci.
- Streptococci also produce exotoxins, which destroy neutrophils. This results in the growth of bacteria, which in turn destroy the tissues.
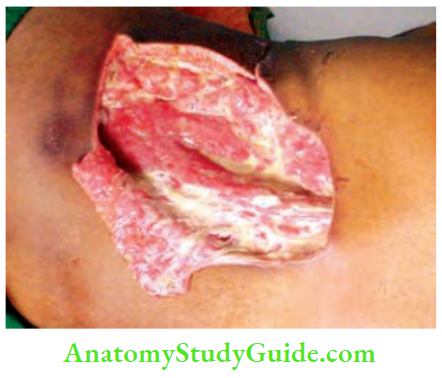
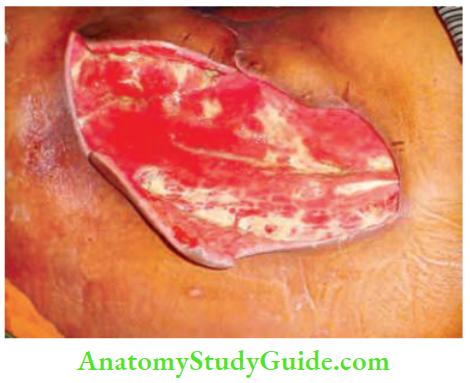
Necrotising Fasciitis Clinical Features
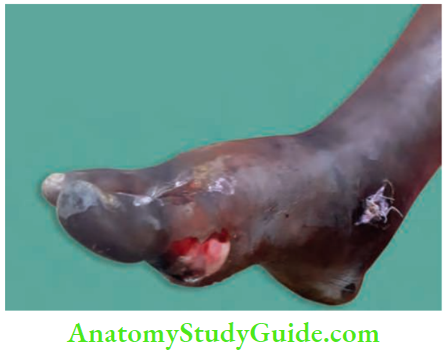
Sudden pain in the affected area with gross swelling of the limbs.



The part is swollen, red, erythematous, and oedematous with skip lesions of skin necrosis and ulceration.
- Skin changes: Bronze hue, brawny induration, blebs, or crepitus are other important features. Very soon, skin patches and a dusky blue colour, followed by blebs and bullae appear.
- Thrombosis of the nutrient artery results in gangrene. Interestingly, muscles are spared.
- High-degree fever, jaundice, and renal failure may occur soon in untreated cases.
Necrotising Fasciitis Diagnosis
- Early diagnosis may be made by a scoring system proposed by Wong et al., which considers white cell count, CRP (C-reactive protein), haemoglobin, sodium, creatinine, and glucose levels. This system is called the Laboratory Risk Indicator of Necrotising Fasciitis—LRINEC.
- Full thickness biopsy taken at bedside may give the full diagnosis. Watery pus (dishwater liquid) is also characteristic.
- A high index of suspicion is required to diagnose necrotising fasciitis. When in doubt, one can do exploratory fasciotomy. Lack of resistance between normally adherent fascia to blunt dissection is diagnostic of necrotising fasciitis.
- The finger test is a bedside procedure done under local anaesthesia. A 2-cm incision is made and deepened to the deep fascia, at which level gentle probing with the index finger is applied. The presence of dishwater liquid and a lack of resistance are characteristic of necrotising fasciitis.
Diagnosis Treatment
Early, aggressive management with supportive and surgical treatment.
- Supportive treatment includes hospitalisation, adequate hydration, treatment of hypotension and broad-spectrum antibiotics.
- First and second-generation cephalosporins are used to treat Staphylococcus aureus. However, in cases of resistant cases due to MRSA (methicillin-resistant Staphylococcus aureus) vancomycin with carbapenem may be urgently required. Surgery should be performed as early as possible.
- Severe pain, colour changes in the skin, and drowsiness are indicators of sepsis. In such cases, do not wait for all reports and perform debridement on an emergency basis. This involves wide excision and generous debridement, followed by skin grafting after a few days or weeks.
- Debridement may have to be repeated till healthy tissue is encountered. Do not hesitate to amputate if the patient’s life is in danger, because in a few patients, that is the only life-saving measure.
- Type 2 cases (streptococcal): High-dose penicillins with clindamycin are the treatment of choice. Clindamycin has a special effect as it is a potent suppressor of bacterial toxin synthesis.
- Intravenous immunoglobulin (IVIG) has recently been described as a reasonable and desirable option for neutralizing streptococcal toxins.
Acute Pyomyositis
Acute Pyomyositis Definition
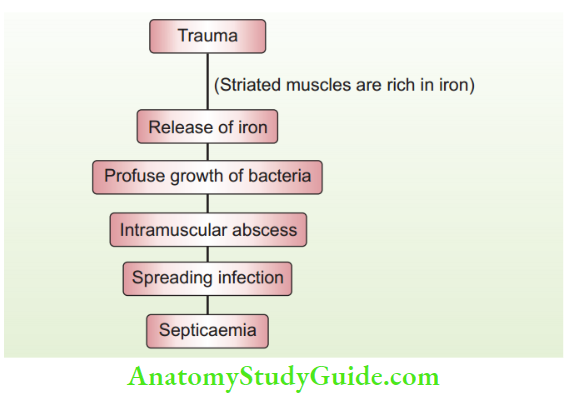
Pyomyositis refers to a localised area of suppuration within the striated muscle. It occurs after trauma.
Pathogenesis of acute pyomyositis
Acute Pyomyositis Clinical Features
Classically, the quadriceps, gluteus, and shoulder and upper arm muscles are affected. Pain over the part, oedema, fever, and jaundice are common. Tenderness, induration, and muscle spasms are characteristic.
Renal failure follows soon.
Acute Pyomyositis Investigations
- Sonographic-guided aspiration of pus followed by culture
- CT and MRI are ideal to determine the spread of the infection.
- Creatine kinase may go up to 50,000–2,00,000 units/L during the acute phase because of rhabdomyolysis.
Acute Pyomyositis Treatment
- Early diagnosis and early aggressive treatment
- Antibiotics
- Exploration—for diagnosis and treatment
- Wide excision of muscles and compartmental excision until viable tissues become visible.
Summary Pyomyositis
- Trauma
- Transient bacteraemia
- Tropical countries
- Thigh muscles are affected
- Tender intramuscular abscess
- Tenderness, temperature, toxicity
- Total renal failure—rhabdomyolysis
- Treatment—early aggressive exploration and excision
- Observe 8 Ts
Nosocomial Infections
An acquired infection from the hospital is known as a nosocomial infection.
- Infection may occur from the patient’s own organisms (self-infection) or from external organisms.
- Surgical site infections (SSIs) are the third most frequently reported nosocomial infection, after pneumonia and catheter-related infections (including urinary tract infections).
Surgical Site Infections (Ssis)
Surgical Site Infections Definition
- SSIs refer to infections of the tissues, organs, or spaces that have been exposed during invasive surgical procedures. They may be superficial, such as redness of a postoperative wound or a swollen local part.
- When associated with systemic inflammatory response syndrome (SIRS), it is called sepsis, and if it is associated with organ failure and requires inotropes, it is called severe sepsis. More details are given under septic shock.
When to Suspect SSIs?
- A postoperative patient with elevated temperature, tachycardia, tachypnoea, and an elevated white blood cell (WBC) count.
- The wound shows signs of inflammation such as rubor, colour, dolour, and tumour (swelling). These are part of SIRS (systemic inflammatory response syndrome).
- The wound is tender with discharge.
- Microorganisms are identified in blood, pus, or urine.
- SIRS may be caused by a variety of diseases, such as pancreatitis, polytrauma, malignancies, transfusion reactions, as well as infection.
- SIRS caused by an infection is known as sepsis. SIRS is mediated by the production of proinflammatory mediators, such as lipopolysaccharides (endotoxin) derived from gram-negative organisms and peptidoglycans from gram-positive organisms.
PIRO Classification Scheme
Predisposition: Advancing age or immunosuppression that may affect survival.
Insult (infection): It depends on the infecting organism or location of the disease.
Response: It refers to the development of SIRS, shock, elevated C-reactive protein, etc.
Organ dysfunction: Failure or dysfunction of organ(s).
PIRO Classification Scheme Clinical Features
- Superficial SSI: The wound is tender, erythematous, and oedematous.
- Deep incisional SSI: Tenderness extends, and crepitus, vesicles, and/or bullae may be present.
- Intra-cavitary SSI: This depends on the system involved. A classical example is paralytic ileus continuing in abdominal infections.
Common Sources of Infections
Major surgical site infections present with systemic manifestations, whereas minor surgical site infections present with suture site discharge only. In surgical wards, discharging wounds, infected urine, faeces, and sputum are sources of nosocomial infections.
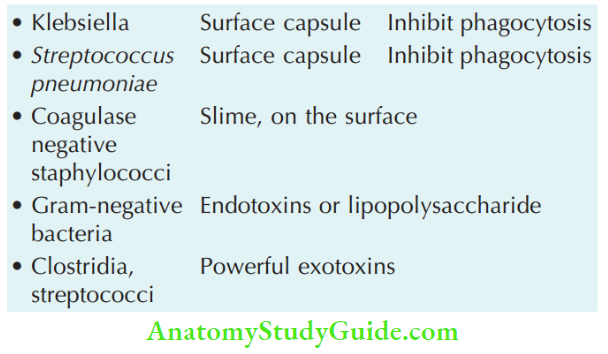
PIRO Classification Scheme Organisms
Staphylococcus aureus remains the most common SSI pathogen, followed by coagulase-negative staphylococci, enterococci and Escherichia coli. Risk factors for the development of SSIs are presented.
Risk Factors for the Development of Surgical Site Infections
- Patient-related (Remember as PATIENT)
- Peripheral vascular disease and smoking
- Anaemia
- Trauma
- Immunosuppression including diabetes
- Elderly (old age)
- Nutritional: Malnutrition
- Too much obesity
- Local features (Remember as LOCAL)
- Long (prolonged) surgical procedure
- Oxygenation is poor (hypoxia)
- Contamination of instruments and skin (poor skin preparation)
- Antibiotic prophylaxis is inadequate
- Local tissue necrosis and low temperature (hypothermia)
Principles of Treatment of Established Surgical Site Infections
- Antibiotics: Empirical broad-spectrum antibiotics that cover all likely organisms must be started, and later switched to the appropriate antibiotic(s) as per the culture-sensitivity report.
- Care of the wound: Wound dressings
- Exploration of wound or peritoneal cavity, removal of the source of sepsis, draining abscess cavity.
What is the decisive period? It takes about 4 hours after surgery for the mobilisation of inflammatory, humoral, and cellular defences. This is the time when invading bacteria get established. Hence, prophylactic antibiotics should be given during this period.
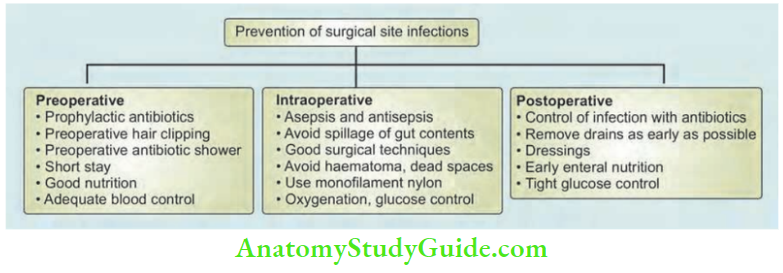
PIRO Classification Scheme Preventing Sources of SSIs
Surgical site infections may be largely prevented or reduced by an approach called the surgical care bundle approach. A bundle refers to a structured process of care that improves patient outcomes. Surgeons may develop their own surgical care bundle for SSIs. This approach may be summarised by 6 Ss.
1. Standardised antibiotic prophylaxis: Antibiotics should be administered ideally 1 hour before the skin incision. It should be repeated every 3 hours if the surgery is prolonged.
2. Skin is prepared by iodophors (povidone iodine 10%) or chlorhexidine gluconate 4% in alcohol. Povidone iodine is safe, fast-acting, and has broad-spectrum (with some sporicidal) activity. Preoperative hair removal (clipping) should be done immediately before any operation.
3. Sterile dressings and proper wound care help protect the incision.
4. Safe operating room: Environmental cleaning and disinfection of the operating room (OR), maintenance of the ventilation system (the bacterial threshold limit for an empty OR is 35 CFU/m3), and minimizing the OR traffic with continuous monitoring.
- SSI may be prevented by maintaining positive pressure in the operating rooms, mechanical ventilation, air conditioning providing filtered air, maintaining temperature, etc.
- The surgeon and team should scrub for at least 3–5 minutes with 4% chlorhexidine gluconate. However, chlorhexidine alcohol-based ‘fast rub’ is more popular now.
- OT attire and drapes: Scrub suits, caps, masks, double gloves, and dedicated footwear are used as barriers. The life of a sterile glove is 3 hours. It should be changed if the surgery lasts > 3 hours.
5. Showers and decolonization with chlorhexidine gluconate 4% during the hospital stay.
6. Screening for colonization of the surgical site.
PIRO Classification Scheme Bacterial factors
Thus, good surgical technique, gentle tissue handling, perfect haemostasis, removal of dead tissues, and appropriate use of sutures, drains, and antibiotics play a major role in preventing SSI.
A summary of the prevention of SSIs is given.
PIRO Classification Scheme Prevention of Hospital Infection
- Avoid unnecessary antibiotics to prevent the development of resistant organisms
- Autoclaving and sterilisation should be done optimally
- Proper ventilation of the wards
- Proper scrubbing before any procedure
- Proper disposal of urine, faeces, sputum
- Use of disinfectants
- Antibiotic prophylaxis
Antimicrobial Prophylaxis Operation Likely pathogens
- Breast – S. aureus, coagulase-negative, staphylococci
- Appendicectomy – Gram-negative bacilli, anaerobes
- Biliary tract – Gram-negative bacilli, anaerobes
- Upper GI – Gram-negative bacilli, streptococci, oropharyngeal anaerobes (peptostreptococci)
- Cefazolin is generally accepted as the antimicrobial agent of choice for clean-contaminated operations.
- Dose: 1–2 g/adult dose.
- Timing: No more than 30 minutes before skin is incised.
Prophylactic regimens
- Vascular: 3 doses of flucloxacillin with or without gentamicin, vancomycin.
- Oesophagogastric: 1 dose of 2nd generation cephalosporin and metronidazole.
- Biliary: One dose of 2nd generation of cephalosporin.
- Small bowel: 1 dose of 2nd generation of cephalosporin with metronidazole.
- Appendix or colorectal: 1 dose of 2nd generation of cephalosporin with metronidazole.
Points in SSI
- SSI within 24 hours is caused by clostridia and streptococci
- SSI after 48 hours (5 days) is caused by gram-negative and other bacteria.
- Nasal carriers of Staph. aureus have ↑ risk of SSI.
- Prevention of SSI is by aseptic and antiseptic techniques in OT as introduced by Lister, the use of prophylactic antibiotics and the patient’s own ability to prevent infection.
- Skin is to be prepared by germicidal antibiotics such as tincture of iodine, povidone iodine or chlorhexidine.
- The first dose of prophylactic antibiotics is given intravenously at the induction of anaesthesia.
- Monofilament sutures are better to decrease the SSI.
Asepsis And Antisepsis
Strictly speaking, they are equivalent and there is not much of a difference between them.
- Asepsis refers to precautions taken before any surgical procedure to prevent the development of infection. Some examples are: wearing gloves, cleaning the patient’s abdomen with iodine and spirit, sterilisation of instruments, and autoclaving.
- Antisepsis: It is defined as the practice of using antiseptics to eliminate disease-causing microorganisms. All surgical procedures today are performed only after taking aseptic precautions.
- Dressing of an already contaminated wound using carbolic acid, and iodine.
- Broad-spectrum antibiotics are used in the presence of infection.
- Wearing a mask and cap in the operation theatre.
Transmissible Viral Infections Hepatitis B
It is a viral infection caused by hepatitis B virus (HBV). It injures the liver. It can result in both acute and chronic disease. It is a major global health problem. Chronic disease results in death from cirrhosis and hepatocellular carcinoma.
- Method of transmission: Contact with blood or other body fluids, including sexual intercourse with an infected partner, injections-drug use that involves sharing needles, and syringes. It can also occur with needle sticks or exposure to sharp instruments. It can also occur from tattooing, or piercing.
- Hepatitis B can be prevented by vaccines that are safe, available and effective.
- Symptoms: There can be febrile illness. It may last from a few days to several weeks. Jaundice, yellow urine, weakness, nausea, and vomiting are other features. Abdominal pain is due to an enlarged liver. A few patients with acute hepatitis can develop acute liver failure, which can lead to death.
- Diagnosis: It is done by detection of the hepatitis B surface antigen HBsAg.
- Methods of prevention: Prophylaxis by taking a vaccine. In the hospitals, all blood donations should be tested for hepatitis B virus infections. Thus to avoid accidental transmission to people who receive blood products.
- This can happen more so in patients who require massive blood transfusions, urgent transfusions and multiple transfusions such as in haemophilia cases, etc.
- All healthcare workers should not only wear double gloves but to avoid accidental pricks during the suturing of tissues, or splashing of fluids during dental extractions etc.
- Treatment: Acute illness requires treatment with paracetamol if fever is present. Otherwise, no specific drugs are used. Tenofovir or entecavir—are the drugs to suppress the hepatitis B virus.
Hepatitis C
Hepatitis C is caused by hepatitis C virus which belongs to RNA virus. There are many forms of hepatitis C—the most common being type 1.
- The incubation period is an average of 45 days—however, it can be anywhere between 2 weeks and 12 weeks.
- Method of transmission: Almost similar in the lines of hepatitis B infections such as body fluids, injection drugs and needles, etc. Transmission does not occur via breast milk, kissing or coughing, sneezing, touching, etc.
- Initial presentation after exposure to the virus is an acute illness that lasts for the first 6 months and can be in the form of fever, clay stools, high-coloured urine, loss of appetite, etc.
- Some of these cases may be completely free by 6 months of time. However, in the majority of patients, the viral infection progresses to chronic hepatitis stage.
- Complications: Cirrhosis and liver cancer: Both these can occur in hepatitis B infections also but in cases of hepatitis C virus infections, these complications can occur early. Very advanced patients can have multiple organ involvement resulting in renal failure, cerebral dysfunction ascites, etc. Intractable itching is also a feature.
- Diagnosis is established by demonstrating AntiHepatitis C Virus (HCV) antibodies. Like many other viral infections, they are demonstrated after about 12 weeks.
- Treatment: No specific treatment or drugs for this condition but symptomatic treatment is given. A few drugs have been used—they are interferon and ribavirin.
- Prophylaxis: There is a vaccine for hepatitis C. The best way is to use universal precautions such as using double gloves, avoiding prick injuries, avoiding needle sharing, avoiding direct exposure to blood and blood products and practising safe sex.
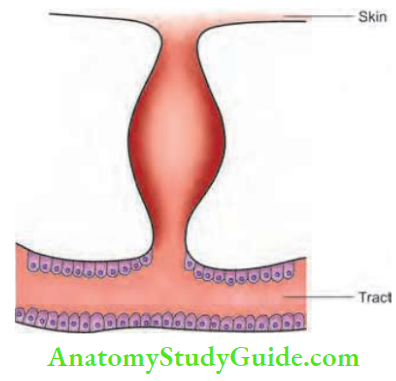
Sinuses And Fistulas
Sinus
It is a blind track from the surface down into the tissues. It is lined by granulation tissue.
A few examples are listed below:
1. Congenital sinus: Pre-auricular sinus, post-auricular sinus.
2. Acquired sinus:
- Median mental sinus: Results from a tooth abscess.
- Pilonidal sinus: Occurs in the midline of the anal region

Osteomyelitis: Gives rise to a sinus that discharges pus ± bony spicules.
The most common sinus in the neck is due to tubercular lymphadenitis. It discharges cheesy material. The skin surrounding the sinus shows bluish discolouration.

Fistula
It is an abnormal communication between the lumen of one viscus and the lumen of another (internal fistula) or a communication between a hollow viscus and the exterior, i.e. body surface (external fistula).
Examples of Internal Fistulas
- Trachea-oesophageal fistula
- Colovesical fistula
Examples of External Fistulas
- Orocutaneous fistula due to carcinoma of the oral cavity infiltrating the skin
- Branchial fistula
- Thyroglossal fistula
- Enterocutaneous fistula
Causes of Persistence of a Sinus or Fistula
- Presence of foreign body
- Persistent infection
- Distal obstruction
- Absence of rest
- Epithelialisation of the track
- Malignancy
- Nondependent drainage, inadequate drainage
- Dense fibrosis
- Irradiation
- Specific causes—tuberculosis, actinomycosis
Please refer to the Manipal Manual of Clinical Methods, 1st edition, for clinical examination of a sinus or fistula.
Sinuses And Fistulas Investigations
Complete blood picture (CBP)—haemoglobin, total and differential count, erythrocyte sedimentation rate (ESR): ESR may be increased in tuberculosis.
- Urine sugar, fasting blood sugar (FBS) and postprandial blood sugar (PPBS) to rule out diabetes.
- X-ray of the part: To look for osteomyelitis of the mandible, toe, and any foreign body.
X-ray kidney, ureter, bladder region (KUB), ultrasound abdomen: Staghorn calculi in lumbar urinary fistula.
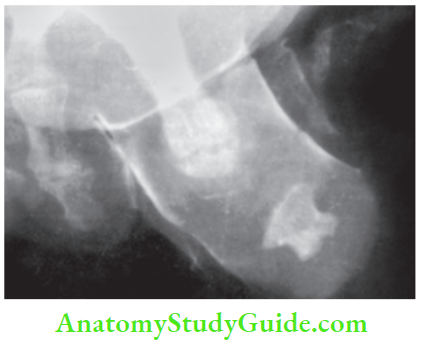
- Fistulography or sinusography to determine the exact extent or origin of the sinus or fistula. A dye such as lipiodol (poppy seed oil containing 40% iodine) is used.
- Biopsy from the edge of the sinus is done if a specific aetiology is suspected (for example. tuberculosis, malignancy).
Sinuses And Fistulas Management
Following are a few examples:
- Sequestrectomy for osteomyelitis.
- Control of tuberculosis for tubercular sinus in the neck.
- Removal of the foreign body, if present (clinical notes)
- If the track is well formed and epithelialised, the entire track should be removed even if the disease is under control.
Sinuses And Fistulas Basic Principles
- Antibiotics
- Adequate rest
- Adequate excision
- Adequate drainage
Sinuses And Fistulas Clinical notes
1. A patient who had undergone surgery for varicose veins had persistent seropurulent discharge from the inguinal incision. Initially, it was thought to be due to infection.
- The discharge persisted for a period of two months. The wound was explored. A gauze piece was found and removed. The wound healed well.
- Retrospective analysis of the surgery revealed slipping of the ligature applied to the long saphenous vein and several gauze pieces were used to control the bleeding point.
2. We had a 60-year-old man who had a small sinus in the loin with a watery discharge. He had seen many doctors over many years. He was treated with antibiotics and antitubercular treatment without any relief. X-ray KUB revealed a staghorn calculus.
Acute Infections Sinuses Fistula And Surgical Site Infection Multiple Choice Questions
Question 1. Treatment of cold abscess is:
- Excision
- Incision and drainage
- Marsupialisation
- Nondependent aspiration
Answer: 4. Nondependent aspiration
Question 2. The following are true about tubercular sinuses in the neck:
- Usually multiple
- The edge is bluish in colour
- Induration is highly characteristic
- Jugulodigastric nodes are commonly affected
Answer: 3. Induration is highly characteristic
Question 3. The ideal treatment of a carbuncle is:
- Drainage
- Incision and drainage
- Excision
- Aspiration
Answer: 3. Aspiration
Question 4. The following are true about Ludwig’s angina except:
- It is caused by Staphylococcus aureus
- Diffuse swelling in the submental and submandibular region is common
- Putrid halitosis is common
- It may also give rise to mediastinitis
Answer: 1. It is caused by Staphylococcus aureus
Question 5. The following are true about pyaemic abscesses except:
- They are usually multiple
- They are deep to the deep fascia
- The diagnostic feature is a high local rise in temperature
- It occurs due to a psychological process
Answer: 3. The diagnostic feature is a high local rise in temperature
Question 6. The following are true about carbuncles:
- Nape of the neck is the most common site
- Cribriform appearance is diagnostic
- Abscesses do not communicate with each other
- Staphylococcus is the most common organism
Answer: 3. Abscesses do not communicate with each other
Question 7. The following are true about erysipelas except:
- Rose pink rash is common
- Cuticular lymphangitis is an important component
- The pinna never gets affected in facial erysipelas
- It is caused by Streptococcus pyogenes
Answer: 3. The pinna never gets affected in facial erysipelas
Question 8. Muscles are spared in which condition?
- Gas gangrene
- Necrotising fasciitis
- Pyomyositis
- Acute embolic gangrene
Answer: 2. Necrotising fasciitis
Question 9. The following are features of necrotising fasciitis type 2:
- It is monomicrobial—β-haemolytic streptococci
- It may also occur in young, healthy individuals
- The organism is not sensitive to clindamycin
- It may give rise to toxic shock syndrome
Answer: 3. The organism is not sensitive to clindamycin
Question 10. Which of the following is true regarding the prevention of surgical site infections?
- Preoperative hair clipping should be done just prior to the surgical procedure
- Skin is prepared by 20% povidone-iodine
- Blood sugar levels should be maintained within 200 mg/dl
- Positive pressure ventilation at a temperature of 25°C is ideal
Answer: 1. Preoperative hair clipping should be done just prior to the surgical procedure
Leave a Reply