Dental Injuries in Primary Dentition Introduction
Trauma to the primary dentition may involve the soft tissues, the supporting bone, or the primary teeth.
Table of Contents
The first two types of injuries have been toddler fall injuries and fall-at-play are the most common modes of trauma to primary dentition in the early childhood years.
The various injuries encountered by primary dentition are luxation injuries and crown and/or root fractures.
Luxation or displacement injuries are 9.8 times more common than crown/root primary tooth fractures.
Read And Learn More: Paediatric Dentistry Notes
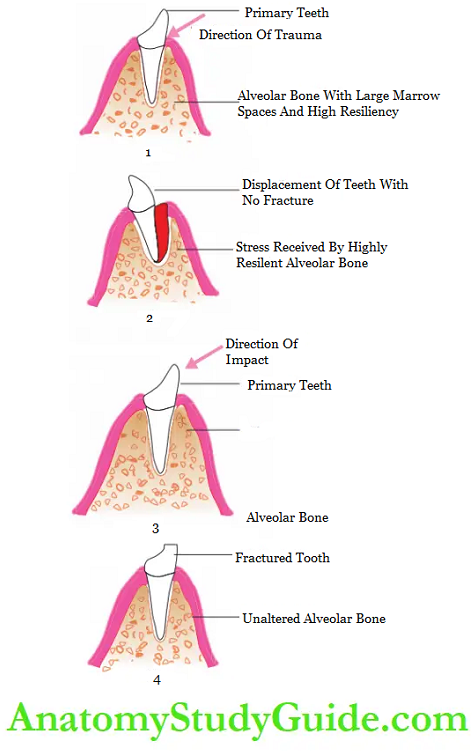
- The primary alveolar bone is less dense, less mineralized, has larger marrow spaces, and has high resiliency.
- Any impact on primary teeth is passed onto the alveolar bone.
- The bone receives the impact owing to its high resiliency and relays the same back to displace the tooth.
Consequences Of Dental Injury In Primary Teeth:
The vitality of the involved tooth is a question of significance.
The traumatized tooth has to be kept under constant observation for the first 6 weeks.
Threon, the review has to be done once in 3 months for the first year and once every 6 months till natural exfoliation of the tooth.
Brown-to-black discoloration of a tooth indicates that it is turning non-vital.
Pulp canal obliteration may be associated with yellowish discoloration.
Internal resorption and external resorption are the other undesirable consequences that may require extraction of the involved tooth.
The fundamentals of management of dental injuries in primary dentition are as follows (incisors are the most commonly avulsed or traumatized tooth in children, so it has been taken as the example to discuss the decision-making parameters):
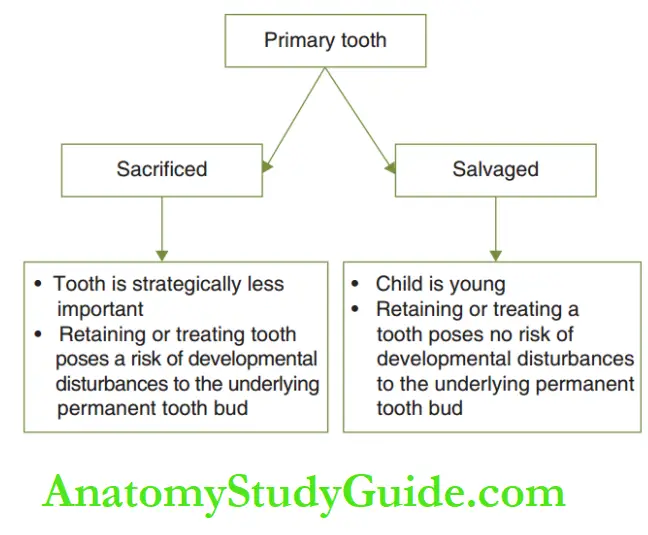
1. Early loss of primary incisors can delay the eruption of the permanent tooth. But loss of a primary incisor, when the child is older than 5 years, can hasten the eruption of permanent incisors.
2. Developmental disturbances to the permanent tooth bud can occur due to traumatic injury to primary incisors, due to the treatment rendered, or due to the associated residual septic foci.
3. A young child who has encountered trauma may have bleeding sores in and around the mouth and displaced/avulsed/fractured teeth. Hence, the child is anxious.
In such a case, pharmacological modes of behavior management such as conscious sedation for calming down an anxious child and general anesthesia for a child lacking cooperative ability (young pre-schoolers/toddlers) may be required.
4. The aforementioned points are weighed when the decision to salvage/sacrifice the traumatized primary incisor is made.
Objectives Of The Line Of Treatment
The objectives of the line of treatment of dental injuries in primary dentition to obtain the desired outcome are as follows:
1. Reassure to relieve the anxiety of the parent and make a choice of an appropriate behavior management strategy to render effective and efficient treatment to the child.
2. Minimise the number of dental extractions as loss of anterior primary teeth can also lead to loss of facial alveolar bone. damage to the gubernacular cord and cause a delay in the eruption of a permanent successor.
3. Primary teeth need not be saved if there is a risk of potential developmental disturbances to a succedaneous permanent tooth.
4. Constant reviews are required to follow the pulp status of the traumatized tooth.
5. The erupting tooth bud pertaining to the traumatized primary tooth has to be reviewed regularly.
Luxation Injuries
Luxation injuries include the following:
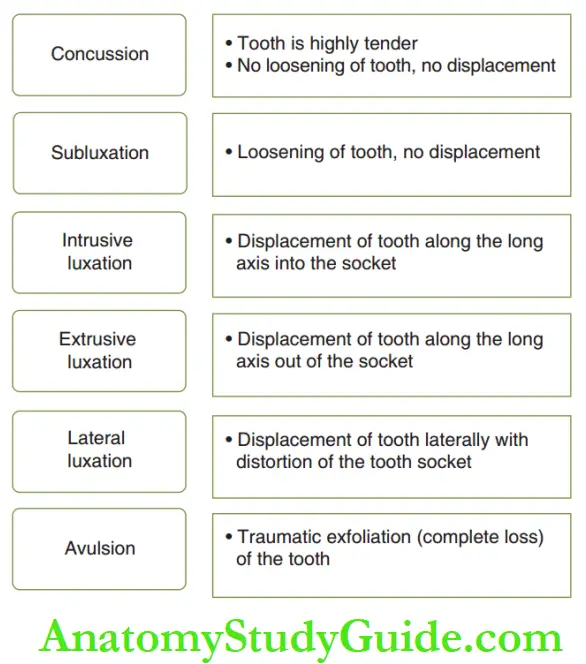
- Concussion
- Subluxation
- Intrusive luxation
- Extrusive luxation
- Lateral luxation (displacement)
- Avulsion
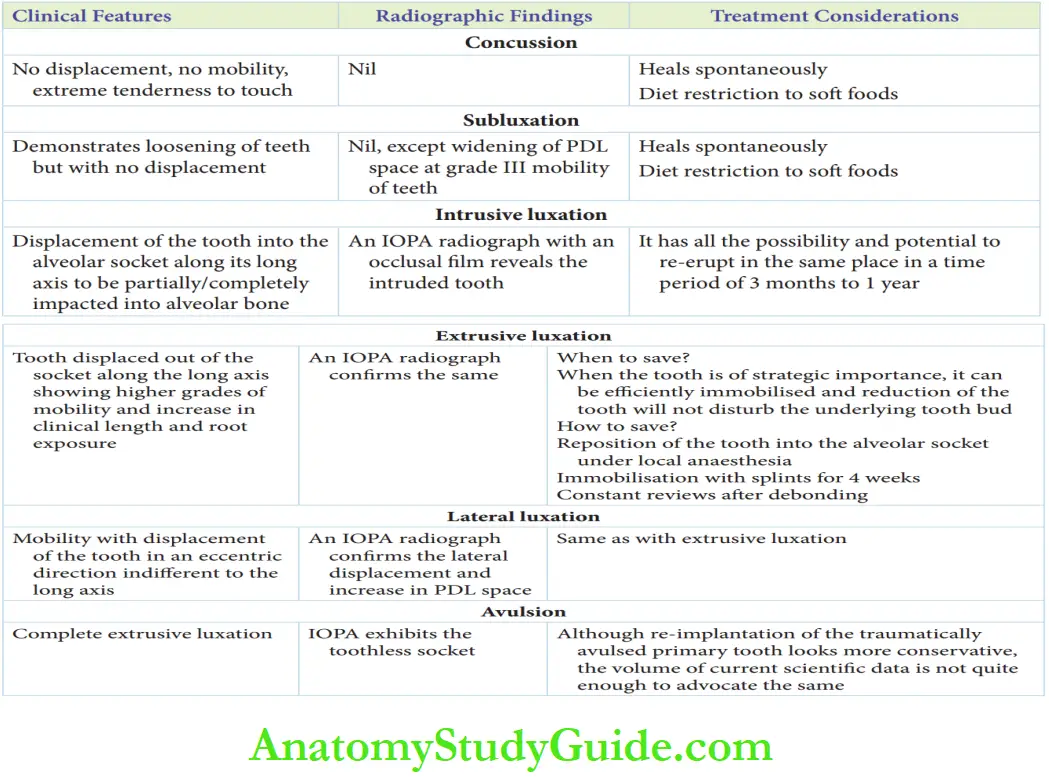
Concussion–Subluxation
Concussion and subluxation are injuries to the supporting structures of a tooth.
Concussion demonstrates no increase in mobility whereas subluxation demonstrates loosening of teeth but with no displacement.
Concussion makes the tooth extremely tender to the touch.
The periodontal ligament is the tissue involved in both lesions.
The concussion shows no positive radiographic signs. Subluxation depicts the widening of the periodontal ligament space in a tooth with grade III mobility.
Concussion and subluxation Management
Concussion and subluxation involve no break or discontinuity or comminution of the alveolar socket wall.
They undergo self-remission in 7 days and require no intervention.
Instructions include diet restriction to soft foods and maintenance of good oral hygiene to avoid bacterial contamination of the inflamed periodontal ligament.
Intrusive Luxation
Intrusive luxation is the displacement of the tooth into the alveolar socket along the long axis of the tooth.
The tooth may partially/completely get impacted into the alveolar bone.
Radiographic Investigation
An IOPA radio graph reveals the intruded tooth. It can also describe the probable trauma inflicted on the developing tooth bud.
The assessment is better with a combination of OPA and occlusal film.
Radiographic Investigation Management:
- The intruded tooth has all the possibility and potential to erupt back into place.
- Significant re-eruption can be expected in 3 months and complete re-eruption in 1 year.
- The permanent tooth bud has to be assessed and reviewed for developmental disturbance although prevention may not be possible after trauma has been incurred.
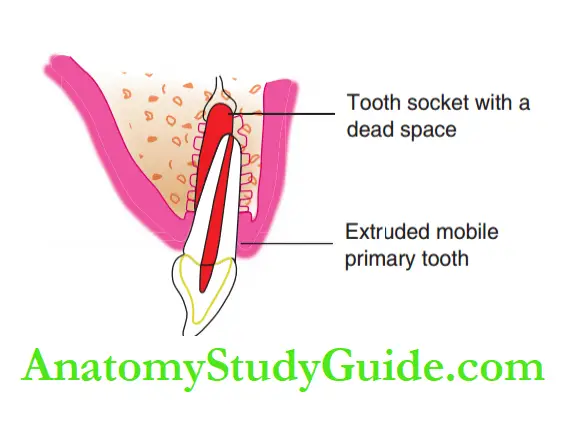
Extrusive Luxation
- Extrusive luxation is the displacement of a primary tooth out of the socket along the long axis.
- The tooth demonstrates a high grade of mobility and an increase in the clinical length of the crown. Root exposure may also be vivid.
- An IOPA radiograph confirms the extrusion of the tooth along its socket.
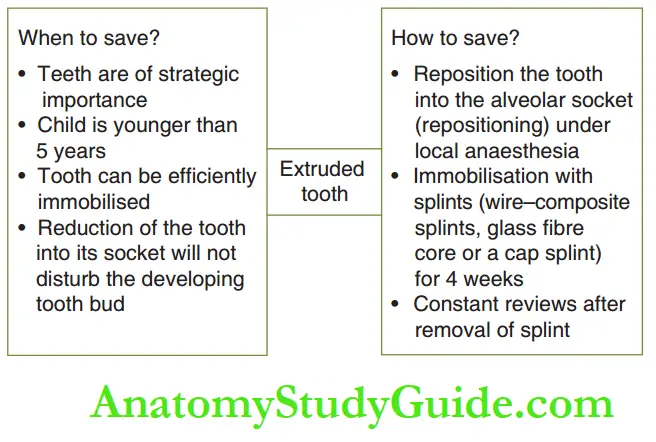
- The conditions in which the tooth can be saved and the line of treatment are depicted.
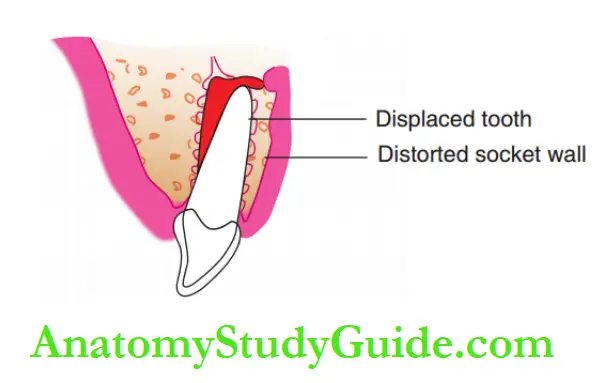
Lateral Luxation
Lateral luxation is the displacement of the tooth in an eccentric direction different from its long axis.
Clinical and radiographic findings confirm the displacement with mobility and distorted tooth socket with enlargement of the periodontal ligament space, respectively.
Treatment considerations are quite identical to those of extrusive luxation.
Repositioning of the laterally displaced tooth has to be performed with extra caution as it may loosen from the socket.
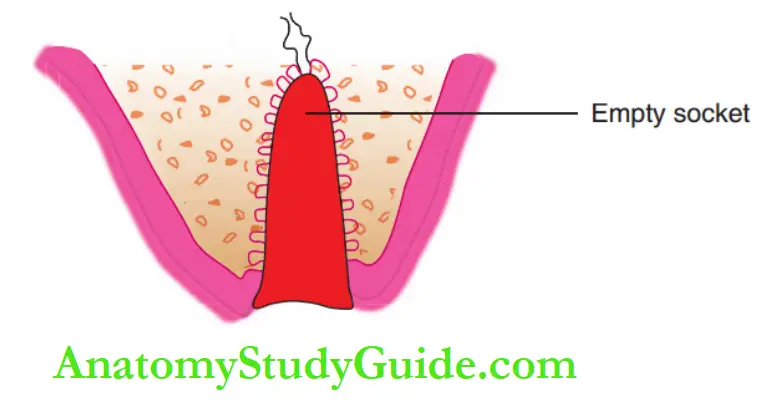
Avulsion
Avulsion or exfoliation is the complete extrusive luxation of the tooth.
There are two diverse schools of thought on the management of an avulsed tooth.
The factors that favor the re-implantation of a tooth are as follows:
- Alveolar socket walls are intact.
- The extraoral time of an avulsed tooth is less than 2 hours.
- An avulsed primary tooth is strategically important.
- The avulsed tooth can be efficiently stabilized.
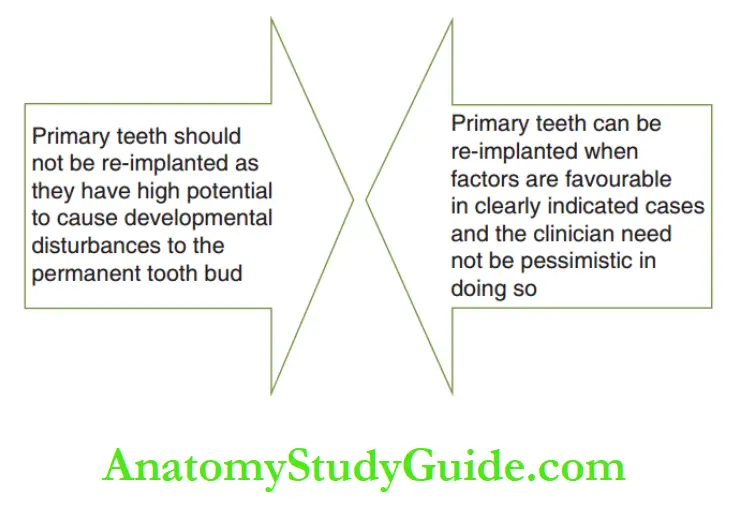
Although re-implantation of the traumatically avulsed primary tooth looks more conservative, the existing scientific data is not enough to advocate the same.
Re-implantation of avulsed primary incisors requires more longitudinal scientific evidence and may possibly be accepted at large sooner.
The bottom line is that any avulsed primary tooth cannot be re-implanted.
Instead, a functional space maintainer (removable/fied) is advocated for functional rehabilitation.
The clinical features of various luxation injuries.
Tooth Fractures
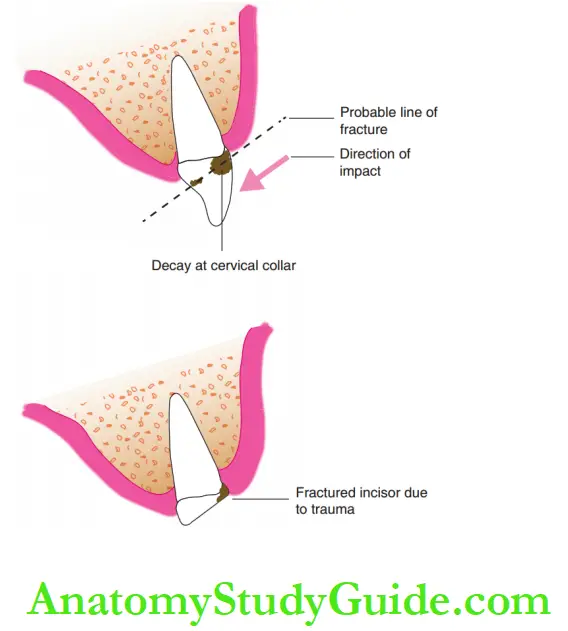
Primary tooth fractures are possible but rare.
The most commonly fractured teeth are maxillary central incisors that are grossly cavitated with early childhood caries (ECC) lesions at the cervical collar.
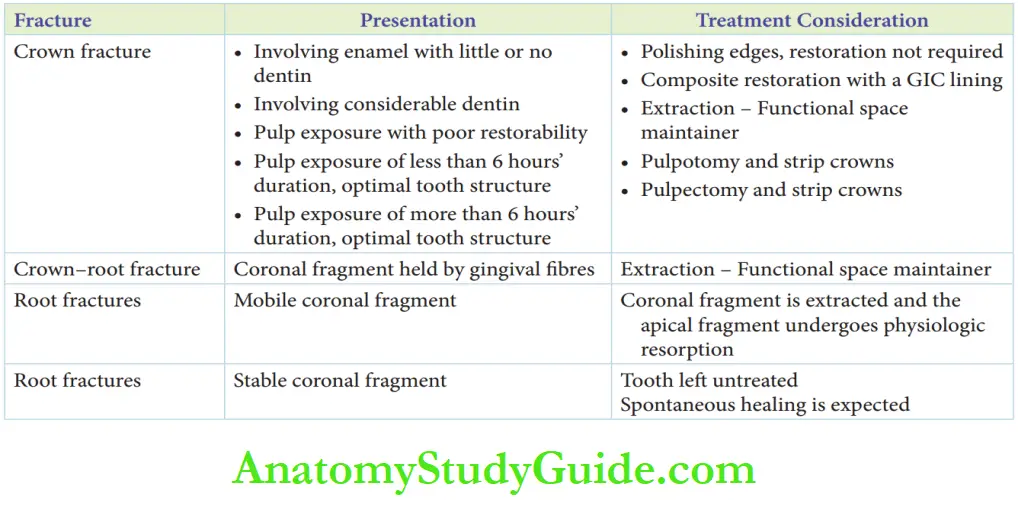
Crown Fractures:
- The crown fracture may involve the enamel with little or no dentin involved.
- Sometimes, the fracture may involve the pulp tissue.
- When the pulp is exposed, the storability of the tooth structure is the key element to deciding if the teeth can be preserved or not.
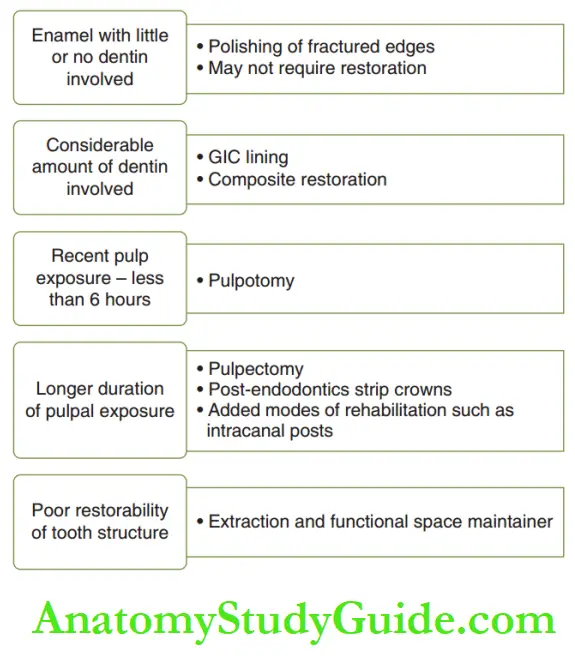
The duration of the exposure to pulp plays a vital role in arriving at the treatment.
Poor storability of tooth structure may warrant an extraction of the tooth followed by a functional space maintainer.
The possible kinds of involvement in a crown fracture and their line of treatment are enumerated.
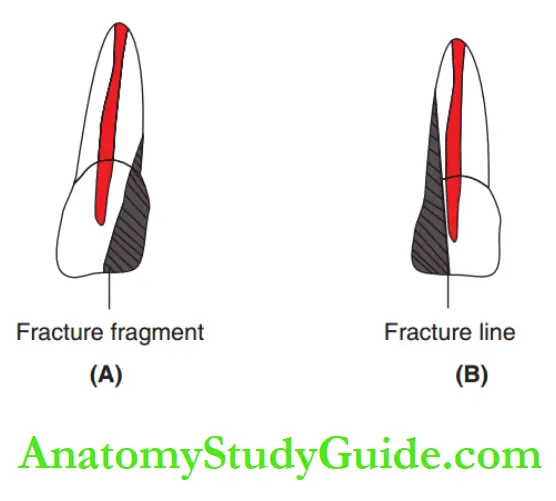
Crown–Root Fractures
A fracture line running through the crown and root may be associated with the crown still being held in place by the gingival fires.
The child may complain of transient pain on mastication.
On account of poor storability and inability to obtain a leak-proof coronal seal, the remnant tooth structure is preferably extracted.
Extraction can be followed by a functional space maintainer.
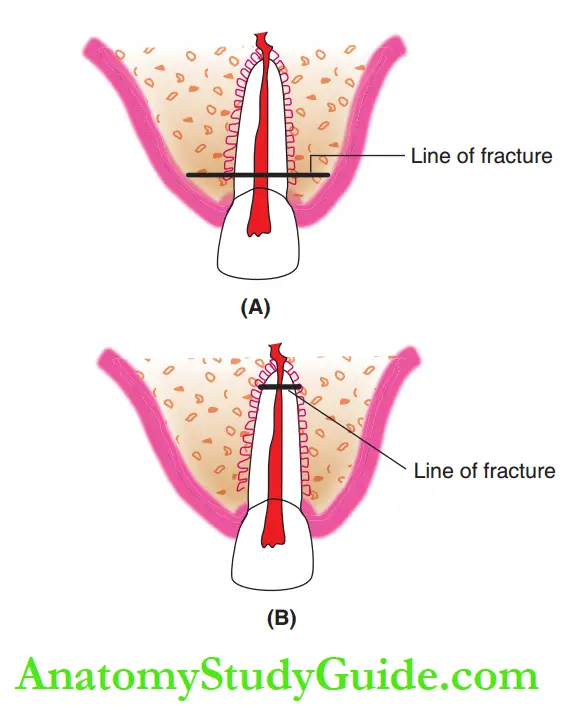
Root Fractures
Fractures of the root may clinically present with a mobile coronal fragment or a stable coronal fragment.
1. Mobile coronal fragment: In this case, the fracture line is more coronal than the apical part of the root.
The coronal fragment can be extracted and the apical fragment can be left untouched to undergo physiologic resorption.
2. Stable coronal fragment: The fracture is more apical than the coronal part of the tooth. The tooth is left untreated. Spontaneous healing can be expected.
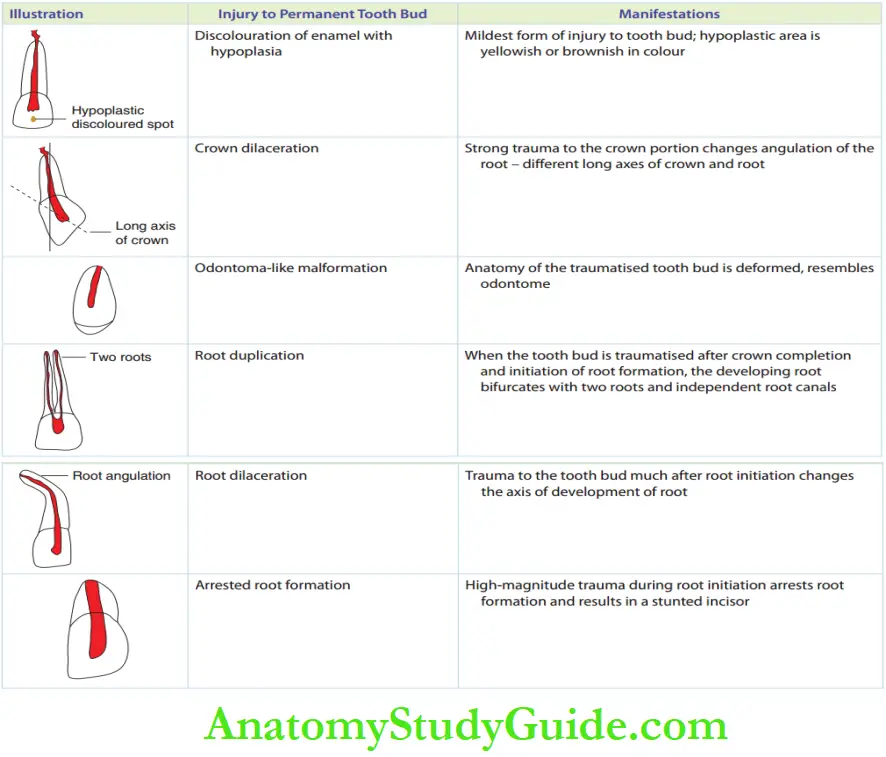
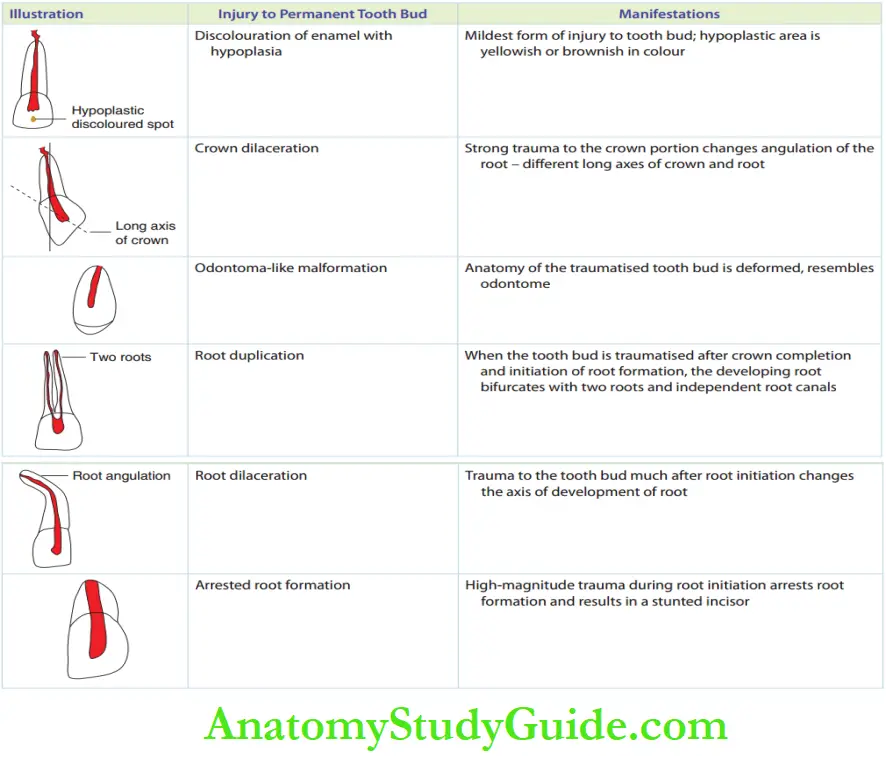
Disturbances To Developing Permanent Tooth Buds
Traumatized primary teeth can potentially infect one of the following developmental disturbances on the developing permanent teeth.
When primary teeth are displaced inwards or sideward, they inflate physical trauma to the developing tooth bud.
The developing toothbud may show one or more of the features depicted.
Traumatic Dental Injuries Summary
1. Consequences of dental injury in primary teeth – The vitality of the involved tooth should be reviewed first at 6 weeks, then once in 3 months for the first year, and once every 6 months from there on till exfoliation.
2. Fundamentals of the management of dental injuries in primary dentition:
- Early loss of primary incisors delays eruption of the permanent incisor
- Treatment of a traumatized primary tooth or associated residual septic foci can produce developmental disturbances to the permanent tooth bud
- A young child who encountered trauma is anxious, so pharmacological modes of behavior management are required
3. The objectives and line of management are as follows:
- Reassure parents, relieve patient anxiety
- Minimize the number of extractions
- Primary teeth need not be saved if there is a risk of developmental disturbances to the permanent tooth
- Constant reviews of a traumatized tooth and the erupting tooth bud are required
4. Traumatic injuries in primary dentition are as follows:
- The primary alveolar bone is less dense and possesses high resiliency. Hence, luxation or displacement injuries are 9.8 times more common than primary tooth fractures.
5. Luxation injuries of primary teeth
6. Tooth fractures – Primary tooth fractures although rare are possible commonly with maxillary central incisors that are grossly cavitated at their cervical collars.
7. Disturbances to developing permanent tooth buds Traumatically injured primary teeth can potentially inflict developmental disturbances on developing permanent teeth.
Leave a Reply