Jaundice
- Jaundice or icterus refers to the yellow pigmentation of the skin or sclerae by bilirubin. Bilirubin pigment has a high affinity for elastic tissue and hence jaundice is particularly noticeable in tissues rich in elastin content.
- Jaundice is the result of elevated levels of bilirubin in the blood termed hyperbilirubinaemia. Normal serum bilirubin concentration ranges from 0.3-1.3 mg dl, about 80% of which is unconjugated.
- Jaundice becomes clinically evident when the total serum bilirubin exceeds 2 mg/dl. A rise of serum bilirubin between the normal and 2 mg/dl is generally not accompanied by visible jaundice and is called latent jaundice.
- Before considering the features and types of jaundice, it is essential to review the normal bilirubin metabolism.
Normal Bilirubin Metabolism
Table of Contents
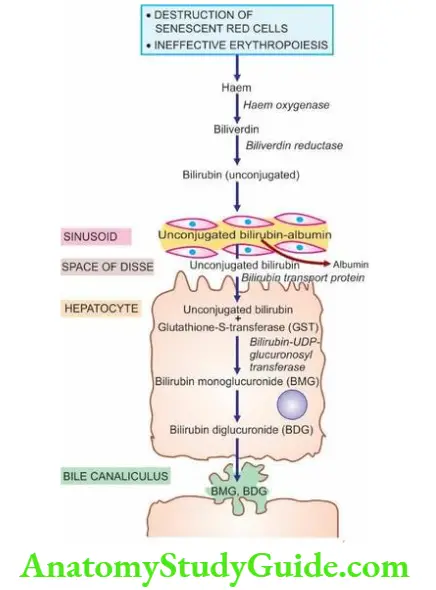
Normal metabolism of bilirubin can be conveniently described under 4 main headings—source, transport, hepatic phase and intestinal phase as illustrated schematically earlier.
1. Source Of Bilirubin: About 80-85% of the bilirubin is derived from the catabolism of haemoglobin present in senescent red blood cells.
- The destruction of effete erythrocytes at the end of their normal lifespan of 120 days takes place in the reticuloendothelial system in the bone marrow, spleen and liver.
- The remaining 15-20% of the bilirubin comes partly from non-haemoglobin haem-containing pigments such as myoglobin, catalase and cytochromes, and partly from ineffective erythropoiesis.
- In either case, haem moiety is formed which is converted to biliverdin by microsomal haem oxygenase for which oxygen and NADPH are essential requirements. Bilirubin is formed from biliverdin by biliverdin reductase.
2. Transport Of Bilirubin: Bilirubin on release from macrophages circulates as unconjugated bilirubin in plasma tightly bound to albumin.
- Certain drugs such as sulfonamides and salicylates compete with bilirubin for albumin binding and displace bilirubin from albumin, thus facilitating bilirubin to enter into the brain in neonates and increase the risk of kernicterus.
- Bilirubin is found in body fluids in proportion to their albumin content such as in CSF, joint effusions, cysts etc.
3. Hepatic Phase: On coming in contact with the hepatocyte surface, unconjugated bilirubin is preferentially metabolised which involves 3 steps: hepatic uptake, conjugation and secretion in bile.
1. Hepatic uptake: Albumin-bound unconjugated bilirubin upon entry into the hepatocyte, is dissociated into bilirubin and albumin.
The bilirubin gets bound to cytoplasmic protein glutathione-S-transferase (GST) (earlier called ligandin).
2. Conjugation: Unconjugated bilirubin is not water-soluble but is alcohol-soluble and is converted into water-soluble compound by conjugation.
- Conjugation occurs in the endoplasmic reticulum and involves conversion to bilirubin mono- and diglucuronide (BMG, BDG) by the action of microsomal enzyme, bilirubin- UDP-glucuronosyl transferase.
- The process of conjugation can be induced by drugs like phenobarbital. Conjugated bilirubin is bound to albumin in two forms: reversible and irreversible.
- Reversible binding is similar to that of unconjugated bilirubin. However, when present in serum for a long time (for example in cholestasis, long-standing biliary obstruction, or chronic active hepatitis), conjugated bilirubin is bound to albumin irreversibly and is termed delta bilirubin or pili protein.
- This irreversible conjugated delta bilirubin is not excreted by the kidney and remains detectable in serum for a sufficient time after recovery from the diseases listed above.
3. Secretion into bile: Conjugated (water-soluble) bilirubin is rapidly transported directly into bile canaliculi by an energy-dependent process and then excreted into the bile.
4. Intestinal Phase: The appearance of conjugated bilirubin in the intestinal lumen is followed by either direct excretion in the stool as stercobilinogen which imparts the normal yellow colour to stool or maybe metabolised to urobilinogen by the action of intestinal bacteria.
- Conjugated bilirubin is normally not absorbable whereas its metabolic product, urobilinogen, is reabsorbed from the small intestine and reaches enterohepatic circulation.
- Some of the absorbed urobilinogen is resecreted by the liver into the bile while the rest is excreted in the urine as urobilinogen.
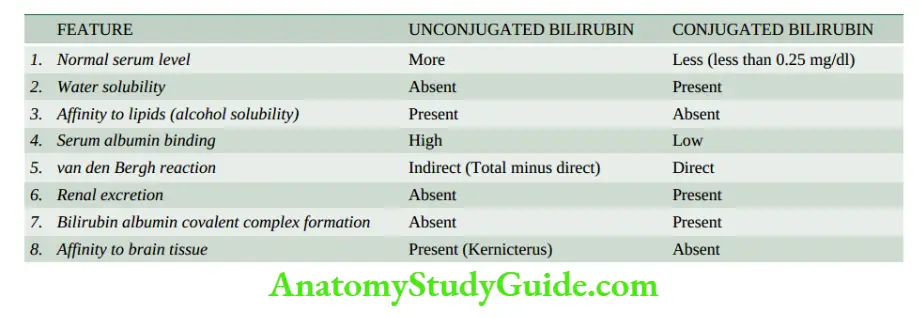
The major differences between unconjugated and conjugated bilirubin are summarised in.
Classification And Features Of Jaundice
Based on pathophysiology, jaundice may result from one or more of the following mechanisms:
- Increased bilirubin production
- Decreased hepatic uptake
- Decreased hepatic conjugation
- Decreased excretion of bilirubin into bile
-
- Accordingly, a simple age-old classification of jaundice was to divide it into 3 predominant types: pre-hepatic (haemolytic), hepatic, and post-hepatic cholestatic.
- However, hyperbilirubinaemia due to the first three mechanisms is mainly unconjugated while the last variety yields mainly conjugated hyperbilirubinaemia.
- A simple test to determine whether hyperbilirubinaemia is of unconjugated or conjugated variety is to determine whether bilirubin is present in urine or not; its absence in urine suggests unconjugated hyperbilirubinaemia since unconjugated bilirubin is not filtered by the glomerulus.
- Hence, currently, the pathophysiologic classification of jaundice is based on the predominance of the type of hyperbilirubinaemia. The presence of bilirubin in the urine is evidence of conjugated hyperbilirubinaemia.
Based on these mechanisms, the pathogenesis and main features of the two predominant forms of hyperbilirubinaemia are discussed below.
1. Predominantly Unconjugated Hyperbilirubinaemia
- Increased Bilirubin Production (Haemolytic, Acholuric Or Prehepatic Jaundice)
- Intra- and extravascular haemolysis
- Ineffective erythropoiesis
2. Decreased Hepatic Uptake
- Drugs
- Prolonged starvation
- Sepsis
3. Decreased Bilirubin Conjugation
- Hereditary disorders (for example Gilbert’s syndrome, Crigler-Najjar syndrome)
- Acquired defects (for example drugs, hepatitis, cirrhosis)
- Neonatal jaundice
2. Predominantly Conjugated Hyperbilirubinaemia (Cholestasis)
- Intrahepatic cholestasis (Impaired hepatic excretion)
- Hereditary disorders or ‘pure cholestasis’ (for example Dubin-Johnson syndrome, Rotor’s syndrome, fibrocystic disease of the pancreas, benign familial recurrent cholestasis, intrahepatic atresia, cholestatic jaundice of pregnancy)
- Acquired disorders or ‘hepatocellular cholestasis’ (for example viral hepatitis, drugs, alcohol-induced injury, sepsis, cirrhosis)
2. Extrahepatic cholestasis (Extrahepatic biliary obstruction)
- Mechanical obstruction (for example gallstones, inflammatory strictures, carcinoma head of the pancreas, tumours of bile ducts,
1. Increased Bilirubin Production (Haemolytic, Acholuric Or Prehepatic Jaundice)
- This results from excessive red cell destruction as occurs in Intra and extravascular haemolysis or due to ineffective erythropoiesis.
- There is an increased release of haemoglobin from the excessive breakdown of red cells that leads to the overproduction of bilirubin. Hyperbilirubinaemia develops when the capacity of the liver to conjugate a large amount of bilirubin is exceeded.
- In premature infants, the liver is deficient in enzymes necessary for conjugation while the rate of red cell destruction is high.
- This results in icterus neonatorum which is particularly severe in haemolytic disease of the newborn due to maternal antibodies.
- Since there is predominantly unconjugated hyperbilirubinaemia in such cases, there is a danger of permanent brain damage in these infants from kernicterus when the serum level of unconjugated bilirubin exceeds 20 mg/dl.
- Laboratory data in haemolytic jaundice, in addition to predominant unconjugated hyperbilirubinaemia, reveal normal serum levels of transaminases, alkaline phosphatase and proteins.
- Bile pigment being an unconjugated type is absent from urine (acholuric jaundice).
- However, there is dark brown colour of stools due to excessive faecal excretion of bile pigmented there is increased urinary excretion of urobilinogen.
2. Decreased Hepatic Uptake: The uptake of bilirubin by the hepatocyte that involves dissociation of the pigment from albumin and its binding to cytoplasmic protein, GST or ligandin, may be deranged in certain conditions example due to drugs, prolonged starvation and sepsis.
3. Decreased Bilirubin Conjugation: This mechanism involves deranged hepatic conjugation due to a defect or deficiency of the enzyme, glucuronosyltransferase.
- This can occur in certain inherited disorders of the enzyme (for example Gilbert’s syndrome and Crigler-Najjar syndrome), or acquired defects in its activity (for example due to drugs, hepatitis, and cirrhosis).
- However, hepatocellular damage causes a deranged excretory capacity of the liver more than its conjugating capacity (see below).
- The physiologic neonatal jaundice is also partly due to a relative deficiency of UDP-glucuronosyltransferase in the neonatal liver and is partly a result of the increased rate of red cell destruction in neonates.
2. Predominantly Conjugated Hyperbilirubinaemia (Cholestasis)
- This form of hyperbilirubinaemia is defined as the failure of normal amounts of bile to reach the duodenum. Morphologically, cholestasis means the accumulation of bile in liver cells and biliary passages.
- The defect in excretion may be within the biliary canaliculi of the hepatocyte and in the microscopic bile ducts (intrahepatic cholestasis or medical jaundice), or there may be a mechanical obstruction to the extrahepatic biliary excretory apparatus (extrahepatic cholestasis or obstructive jaundice).
- It is important to distinguish these two forms of cholestasis since extrahepatic cholestasis or obstructive jaundice is often treatable with surgery, whereas intrahepatic cholestasis or medical jaundice cannot be benefitted by surgery but may in fact worsen by the operation.
- Prolonged cholestasis of either of the two types may progress to biliary cirrhosis.
1. Intrahepatic Cholestasis: this is due to impaired hepatic excretion of bile and may occur from hereditary or acquired disorders.
1. Hereditary disorders
producing intrahepatic obstruction to biliary excretion is characterised by ‘pure cholestasis’ in Dubin-Johnson syndrome, Rotor syndrome, fibrocystic disease of the pancreas, benign familial recurrent cholestasis, intrahepatic atresia and cholestatic jaundice of pregnancy.
2. Acquired disorders: of intrahepatic excretory defect of bilirubin are largely due to hepatocellular diseases and hence are termed ‘hepatocellular cholestasis in viral hepatitis, alcoholic hepatitis, and drug-induced cholestasis such as from administration of chlorpromazine and oral contraceptives.
- The features of intrahepatic cholestasis include predominantly conjugated hyperbilirubinaemia due to regurgitation of conjugated bilirubin into blood, bilirubinuria, elevated levels of serum bile acids and consequent pruritus, elevated serum alkaline phosphatase, hyperlipidaemia and hypoprothrombinaemia.
- ‘Pure cholestasis’ can be distinguished from ‘hepatocellular cholestasis’ by elevated serum levels of transaminases in the latter due to liver cell injury.
- Liver biopsy in cases with intrahepatic cholestasis reveals a milder degree of cholestasis than the extrahepatic disorders.
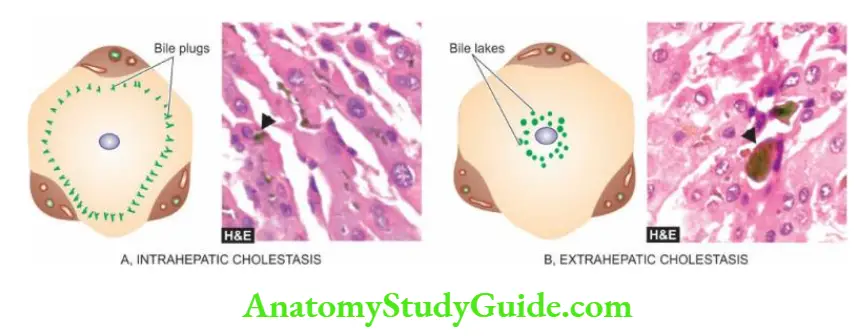
- The biliary canaliculi of the hepatocytes are dilated and contain characteristic elongated green-brown bile plugs. The cytoplasm of the affected hepatocytes shows feathery degeneration.
- Canalicular bile stasis eventually causes the proliferation of intralobular ductules followed by periportal fibrosis and produces a picture resembling biliary cirrhosis.
2. Extrahepatic Cholestasis
-
- Extrahepatic cholestasis results from mechanical obstruction to large bile ducts outside the liver or within the porta hepatis.
- The common causes are gallstones, inflammatory strictures, carcinoma head of the pancreas, tumours of the bile duct, sclerosing cholangitis and congenital atresia of extrahepatic ducts.
- The obstruction may be complete and sudden with eventual progressive obstructive jaundice, or the obstruction may be partial and incomplete resulting in intermittent jaundice.
- The features of extrahepatic cholestasis (obstructive jaundice), like in intrahepatic cholestasis, are predominantly conjugated hyperbilirubinaemia, bilirubinuria, elevated serum bile acids causing intense pruritus, high serum alkaline phosphatase and hyperlipidaemia.
- However, there are certain features which help to distinguish extrahepatic from intrahepatic cholestasis.
- In extrahepatic cholestasis, there is malabsorption of fat-soluble vitamins (A, D, E and K) and steatorrhoea resulting in vitamin K deficiency.
- Prolonged prothrombin time in such cases shows improvement following parenteral administration of vitamin K, whereas hypoprothrombinaemia due to hepatocellular disease ( intrahepatic cholestasis) shows no such improvement in prothrombin time with vitamin K administration.
- The stools of such patients are clay-coloured due to the absence of bilirubin metabolite, stercobilin, in faeces and there is virtual disappearance of urobilinogen from the urine.
- These patients may have a fever due to a high incidence of ascending bacterial infections (ascending cholangitis).
- Liver biopsy in cases with extrahepatic cholestasis shows more marked changes in cholestasis.
- Since the obstruction is in the extrahepatic bile ducts, there is a progressive retrograde extension of bile stasis into an intrahepatic duct system.
- This results in the dilatation of bile ducts and rupture of canaliculi with extravasation of bile-producing bile lakes.
Since bile is toxic, the regions of bile lakes are surrounded by focal necrosis of hepatocytes. - Stasis of bile predisposes to ascending bacterial infections with an accumulation of polymorphs around the dilated ducts (ascending cholangitis).
- Eventually, there is proliferation of bile ducts and the appearance may mimic biliary cirrhosis.
Neonatal Jaundice
- Jaundice appears in neonates when the total serum bilirubin is more than 3 mg/dl.
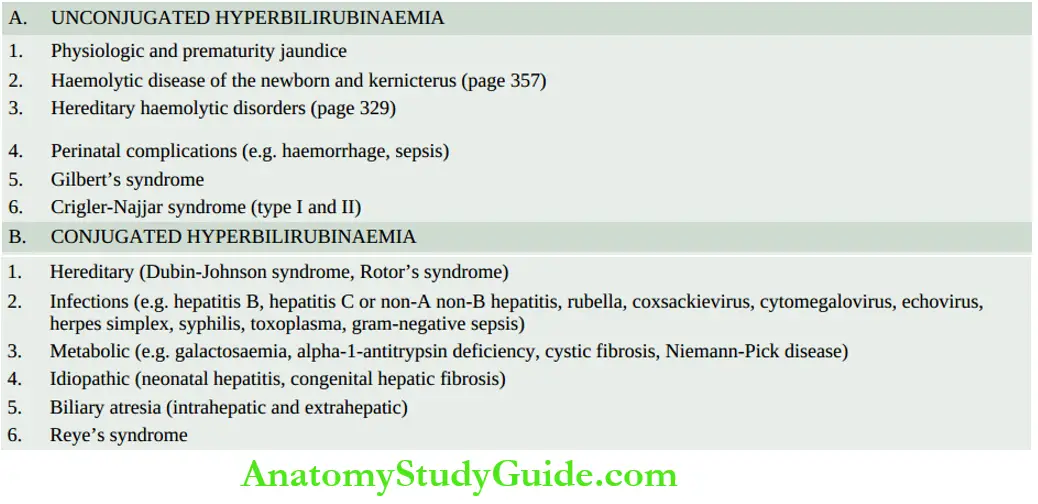
- It may be the result of unconjugated or conjugated hyperbilirubinaemia; the former being more common. Important causes of neonatal jaundice are listed. Out of these, the following conditions are discussed here:
- Hereditary non-haemolytic hyperbilirubinaemias
- Neonatal hepatitis
- Biliary atresias
- Reye’s syndrome
Hereditary Non-haemolytic Hyperbilirubinaemias
- Hereditary non-haemolytic hyperbilirubinaemias are a small group of uncommon familial disorders of bilirubin metabolism when haemolytic causes have been excluded.
- The commonest is Gilbert’s syndrome; others are Crigler-Najjar syndrome, Dubin-Johnson syndrome, Rotor’s syndrome, benign recurrent intrahepatic cholestasis and progressive familial intrahepatic cholestasis.
- The features common to all these conditions are the presence of icterus but almost normal liver function tests and no well-defined morphologic changes except in Dubin-Johnson syndrome.
- Gilbert’s syndrome and Crigler-Najjar syndrome are examples of hereditary nonhaemolytic unconjugated hyperbilirubinaemia, whereas Dubin-Johnson syndrome, Rotor’s syndrome and benign familial recurrent cholestasis are conditions with hereditary conjugated hyperbilirubinaemia.
- These conditions are briefly described below. Their distinguishing features of major forms are summarised.
Leave a Reply