Large Intestine Surgical Anatomy
- The large intestine extends from the ileocaecal valve to the anus. It has five segments: Right colon, left colon, transverse colon, sigmoid colon, rectum and anal canal
- The average length is about 135–150 cm.
- Interestingly, alternating portions of the colon are mobile and fixed. The ascending colon and descending colon are fixed but the caecum, transverse colon and sigmoid colon are mobile. Mobile structures can undergo twisting (volvulus).
- Layers of colon: Mucosa, submucosa, muscularis propria and serosa. Inner circular and outer longitudinal muscle layers constitute muscularis propria. In spite of 4 layers, the wall of the colon is thin.
- Hence it distends much more in obstruction.
Read And Learn More: Gastrointestinal Surgery Notes
Table of Contents
Caecum
- 7.5 cm in both length and breadth
- Blind pouch
- Completely covered by peritoneum except posterior surface
- Mobile
Caecum Diseases:
- Carcinoma
- Tuberculosis
- Amoebic typhlitis
- Intussusception
- Volvulus—rare
Ascending Colon (15 cm Long)
- Caecum continues as ascending colon.
- Covered by peritoneum in front and on both sides.
- In 25% of patients, it has a mesentery.
- The right paracolic gutter is deep on the lateral aspect of ascending colon—space for paracolic abscess in cases of perforation peritonitis.
Transverse Colon (50 cm Long)
- The most mobile part of large intestine.
- It is suspended by transverse mesocolon, loops down and is adherent to the posterior wall of the omental bursa.
Transverse Colon Diseases:
- Cancer
- Ulcerative colitis
Descending Colon (25 cm Long)
- Continues as sigmoid colon
- Retroperitoneal (like ascending colon)
- Also has a paracolic gutter
Sigmoid (40 cm Long)
- S-shaped
- Ends as a rectosigmoid junction where taenia coli ends.
Sigmoid Diseases:
- Volvulus
- Diverticulosis
- Cancer
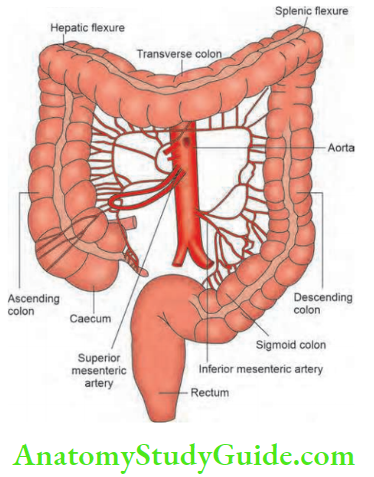
Right Colon: The big and hepatic flexure is broad.
Left Colon
- Small and splenic flexure is acute. Hence, ischaemic colitis commonly affects splenic flexure
- Splenic flexure is deeply situated. Therefore, malignancy in this area can be easily missed.
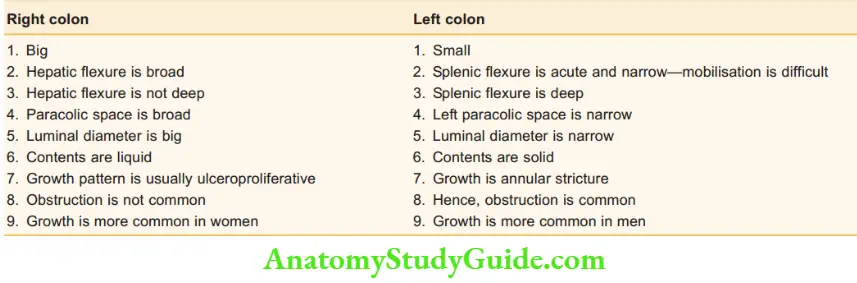
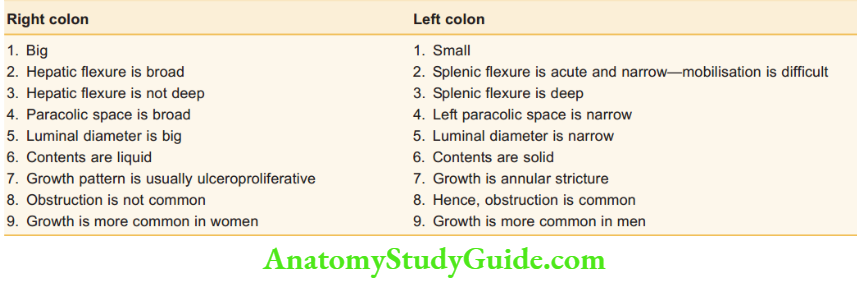
Comparison between Right and Left colon:
Muscle Coat
- Outer longitudinal muscle is arranged in the form of three strips called taenia coli.
- All three join at the rectosigmoid junction and form a complete longitudinal layer of the rectum. These three taenia coli converge at the base of the appendix.
- This is an important method to localise the appendix. Inner circular muscle coalesces distally to form an internal anal sphincter. No taenia over the rectum.
Recognise large intestine by:
- Taenia coli
- Omental appendices—appendicular epiploic ae
- Haustrations
- Large diameter (calibre)
Names of three Taenia coli:
- Mesocolic: Transverse colon and sigmoid colon are attached by this.
- Omental: To which omental appendices attach.
- Libera (free): Nothing is attached.
Colorectal Arterial Supply
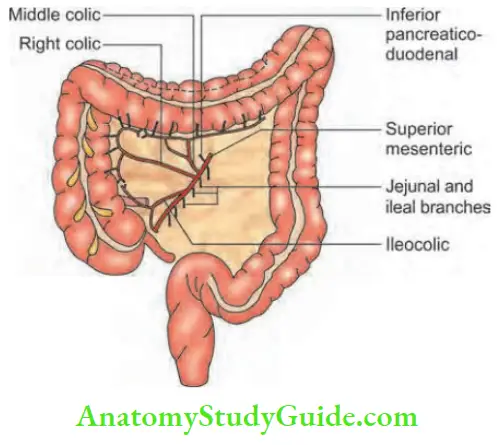
1. Superior mesenteric artery:
A branch of the abdominal aorta arises at the level of the first lumbar vertebra (L1). It supplies the entire small bowel and the right colon up to the proximal 2/3rds of the transverse colon.
Branches of the superior mesenteric artery (SMA) supplying the colon are:
- Middle colic artery: The middle colic artery supplies ascending colon, hepatic flexure and transverse colon. It divides into right and left branches.
- The right colic artery supplies the right colon.
- The ileocolic artery supplies the terminal ileum and ascending colon. It divides into anterior and posterior caecal branches and supplies the caecum and appendix through the appendicular artery.
Comparison Between Right And Left Colon:
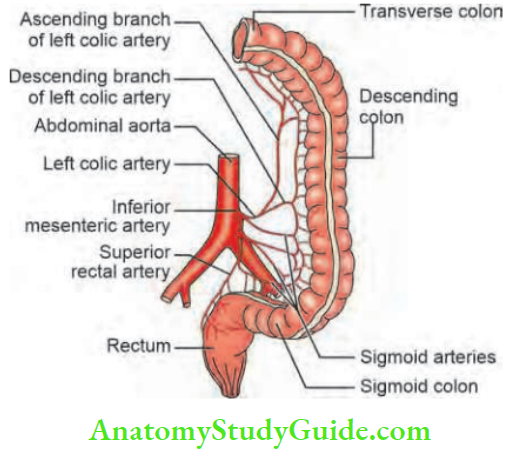
2. The inferior mesenteric artery (IMA): A branch of the abdominal aorta arising at the level of L3, supplies the left colon up to the mucocutaneous junction at the lower end of the anal canal (Hilton’s line).
Its branches are:
- Left colic artery: Left colic artery which anastomoses with branches of the middle colic artery. It divides into upper and lower branches supplying the descending colon.
- Three sigmoidal branches supply the sigmoid colon: The narrow point of blood supply between the first sigmoidal artery and left coelic artery is called Sudeck’s point.
- Superior haemorrhoidal artery (rectal):
- The anastomotic branches form the marginal artery of Drummond, which is relatively narrow in the region of splenic flexure (another reason for the development of ischaemia).
- That narrow point is called Griffith’s point.
- The Arc of Riolan is the anastomotic arcade formed between branches of IMA and SMA.
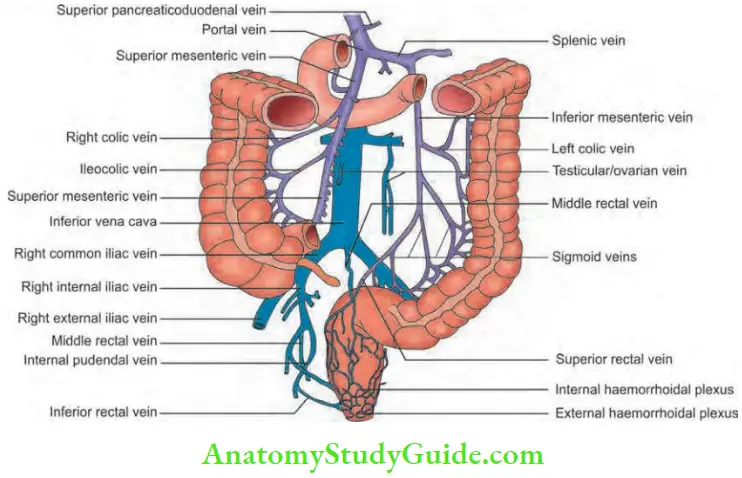
Colorectal Venous Supply
- Follows the corresponding artery and empties into superior and inferior mesenteric veins, ultimately draining into the portal vein.
- Thus, if the colorectal area gets infected secondary to inflammatory conditions or after a surgical procedure, the infection can easily spread to the portal vein and result in portal pyaemia.
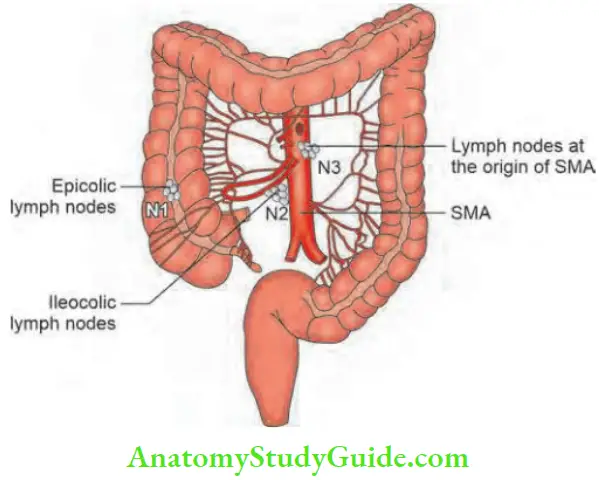
Lymphatic Drainage
- N1: Epicolic and paracolic nodes are the first to get involved.
- N2: Nodes at the origin of ileocolic and middle colic arteries—intermediate nodes.
- N3: Nodes at the origin of superior and inferior mesenteric arteries. They are involved in approximately 50% of the patients with carcinoma colon at presentation to the hospital. These are called principal nodes.
Colorectal Nerve Supply
- Sympathetic (inhibitory) arise from T10–T12 and L1–L
- Parasympathetic (stimulation).
- The vagus nerve supplies the right and transverse colon.
- Sacral nerves (S2–S4 which form nervi erigentes) supply the distal colon, i.e. splenic flexure onwards.
Colorectal Significance:
- Colonic pseudo-obstruction starts from splenic flexure.
- The transition zone of vagal supply to sacral nerve supply.
Tumours Of The Large Intestine
Benign tumours are usually referred to as polyps, which means elevated from the surface. Adenomatous polyps have got malignant potential. A few criteria have been incorporated into a system when malignancy develops in the polyp.
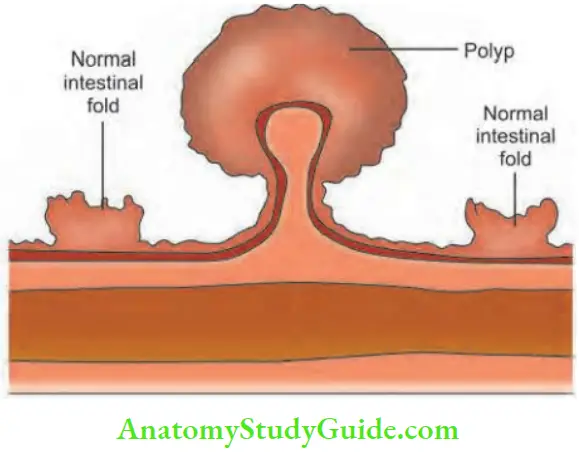
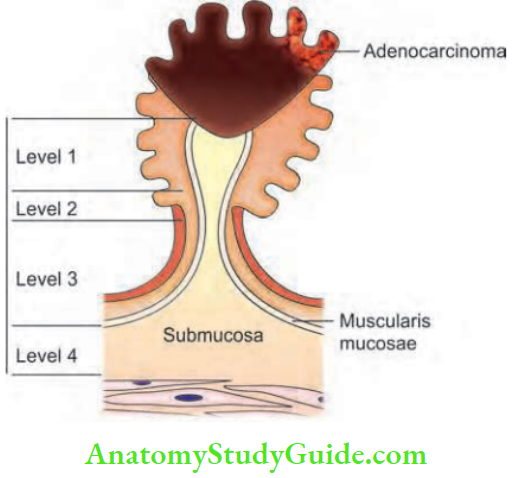
- It takes into consideration of level of invasion.
- Level 1: In this, carcinoma is limited to the top of the polyp. From the mucosa, it is invading through muscularis mucosa into the submucosa.
- Level 2: Carcinoma at the junction of head and stalk.
- Level 3: Carcinoma confined to anywhere in the stalk.
- Level 4: Infiltration into submucosa.
Adenomatous Polyp
- It may be a villous adenoma which is a flat lesion or a tubular adenoma having a pedicle. Tubular is more common.
- They give rise to bleeding, mucus diarrhoea and hypokalaemia.
- They can be single or multiple.
- They are dysplastic.
- They are premalignant and the risk of malignancy is greater with an increase in the size of the adenoma.
- They can be removed with the colonoscope— polypectomy.
- The malignant potential of villous adenoma is more than tubular adenoma.
- Adenoma less than 1 cm—the risk of malignancy is 1%; 1–2 cm is 10%; >2 cm is 30%.
- Most of the neoplastic polyps occur in elderly patients(>50 years).
- Most of them are pedunculated.
- Most pedunculated polyps are removed by colonoscopic snaring.
- Adenomas larger than 5 mm in diameter carry a risk of malignant potential.
- The more the polyps, the more chances of synchronous carcinoma.
- Flat adenomas also carry malignant potential.
Symptoms and signs of polyps: Bleeding per rectum is the most common symptom. Fresh bleeding is seen in rectal polyps. Typically, it is painless. It is intermittent. If it is associated with the change of bowel habits it is probably a malignant change. These changes include mucus discharge, tenesmus, and sometimes constipation. In children, polyps may project outside the anus. In such cases, it has to be distinguished from a prolapsed rectum.
Adenomatous Polyp Treatment:
- Colonoscopy and polypectomy is the standard treatment.
- If the specimen shows invasive carcinoma, radical surgery needs to be done.
Hamartomatous Polyp (Juvenile Polyp)
- This can occur in the colon as in Peutz-Jeghers syndrome. The risk of malignancy is very limited.
- Symptomatic polyps need to be treated.
- Juvenile polyps are usually single and occur in children. They give rise to bleeding and are easily resected. They do not have malignant potential.
Familial Polyposis Coli (Fpc) Or Familial Adenomatous Polyposis (Fap)
- FAP is a genetic disorder inherited as a Mendelian dominant. The gene APC (adenomatous polyposis coli) is located on the short arm of chromosome 5. Prevalence: 1 in 10,000. It is clinically defined by the presence of more than 100 colorectal adenomas.
- It is transmitted from both sexes. The incidence is same in either sex.

- When it is associated with desmoid tumour, craniofacial osteomas, epidermoid cysts, and congenital hypertrophy of retinal pigment epithelium, it is described as Gardner’s syndrome.
- When familial polyposis coli is associated with central nervous system tumour and glioblastoma, it is called Turcot’s syndrome.
- 50% of them have benign gastric polyps and 90% of them have duodenal polyps.
FAP Clinical Features:
- Runs in families; other members of the family are affected.
- Manifests at the age of 20 in the form of blood and mucus in the stool, loose stools, etc. It produces crampy lower abdominal pain.
- Anaemia, weight loss and protein malnutrition occur slowly.
- The mean age of development of carcinoma is 29 years.
FAP Complications: Malignancy (100% risk)
Family Polyposis Coli:
- Polyps are more than 100 (colorectal adenomas).
- Other mesodermal tumours—desmoid tumours, osteoma, and epidermoid cysts can be present (Gardner’s syndrome).
- Large bowel is predominantly involved.
- Year of development of carcinoma—mean age 39 years.
- Polyposis gene—autosomal dominant APC gene.
- Other syndrome—Turcot
- Sigmoidoscopy from the age of 15 at intervals is the investigation of choice.
- I leoanal anastomosis with pouch—restorative proctocolectomy—advisable above age of 30.
- Surgery is the only means of preventing colonic cancer.
- Remember as POLYPOSI
FAP Treatment:
- NSAID: Sulindac 300 mg, twice a day and aspirin 325 mg once a day have been found to decrease the size of polyps.
- Patients with FAP who are above the age of 30 have high chances of having a carcinoma in the colon. Hence, even when there is no malignancy, surgery is advisable.
Types of Surgery:
- Many patients do not like ileostomy. Hence, a subtotal colectomy with ileorectal anastomosis can be done.
- This is done provided that the rectum is examined frequently and endoscopic snaring of the polyps is done regularly, especially in a young patient.
- Restorative proctocolectomy with ileoanal anastomosis by using a pouch is another alternative.
- However, it is a major surgical procedure and should be undertaken only by an experienced surgeon.
Screening: Starts from the age of 10–12 years, repeat every 1–2 years.
Metaplastic Polyp
Also called hyperplastic nodules. They are of viral aetiology. They do not have malignant potential.

Hereditary Nonpolyposis Colorectal Cancer (Hnpcc)
- Autosomal dominant, no polyps
- Lynch’s syndrome 1: Site-specific colorectal cancer.
- Lynch’s syndrome 2: Cancer family syndrome—they have extracolonic cancers such as endometrial cancer, ovarian cancer, transitional cell cancer, etc.
- The lifetime risk of developing colorectal cancer is 80%.
- Synchronous carcinoma means more than one cancer at the time of diagnosis. Metachronous carcinoma which means the appearance of a second carcinoma after 6 months can occur here.
Diagnostic Criteria (Amsterdam Criteria II):
- At least 3 members in a family should have colorectal cancer—two of whom are first-degree relatives.
- At least two consecutive generations.
- At least one relative should have had colorectal cancer by less than 50 years of age.
- Exclusion of FAP.
Screening: Increased incidence of proximal colonic cancer.
Examination Of Colon
Anoproctoscopy: One can examine up to 10–12 cm of the anal canal and rectum. Rubber band ligation (for piles) and polypectomy can be done with this instrument.
Flexible sigmoidoscopy:
The scope measures about 60 cm in length. One can easily reach up to splenic flexure.
- A bowel wash or an enema is given before the procedure.
- No sedation is required.
Fibreoptic colonoscopy: Fibreoptic colonoscopy can assess the entire colon. It is 100–160 cm in length.
- Usually, there will be multiple polyps varying from a few millimetres to centimetres.
- A biopsy has to be taken. Polyps are visible after 15 years and certainly by the age of 30 years.
- It is the investigation of choice in most of the large intestinal lesions.
- It permits examination of the entire colon and terminal ileum.
- Colon is prepared by polyethene glycol given orally.
- The risk of perforation of the colon is less than 0.1%.
Colon Indications:
- Diagnostic: Lower gastrointestinal bleeding
- Inflammatory bowel diseases
- Abnormal finding in barium enema
- Family history of colorectal cancers
- Biopsy of caecum/ileum in suspected cases of cancer
- Ileocaecal tuberculosis—to take a biopsy


- Therapeutic:
- Control of bleeding—coagulation or injection sclerotherapy
- Snaring of polyps
- Removal of foreign body
- Detorsion of volvulus
- Decompression of pseudo-obstruction
Carcinoma Colon
Carcinoma Colon Introduction:
It is the second most common cancer and cancer-related death cases in the Western world next only to lung cancer. The incidence increases with age. Multiple synchronous lesions (more than 1 malignancy at the time of diagnosis) are found in about 5% of the patients.
- Colon is also one of the sites of metachronous cancer (new malignancy appearing after 6 months of curative surgery).
- More than 95% are adenocarcinoma and surgery remains the most effective treatment. Survival has improved because of early diagnosis and multimodality of the treatment.
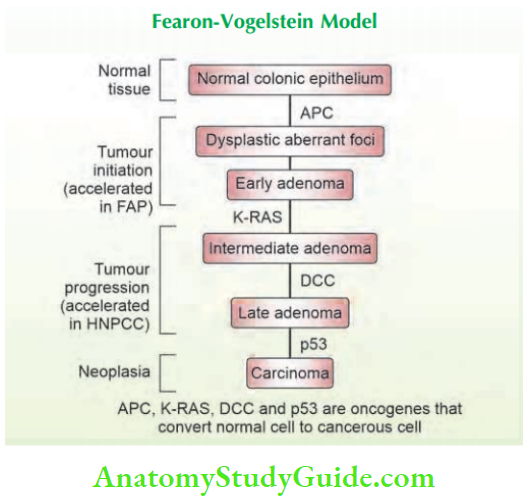
- Over a period of years, the understanding of the development of carcinoma has changed and more and more molecular biology of colonic cancer is being discussed.
- The Fearon-Vogelstein adenoma–carcinoma multistep model of colorectal neoplasia represents one of the best-known models of carcinogenesis.
Carcinoma Colon Terminology:
- Before we start the discussion on carcinoma colon, we shall study a few terminologies used in carcinoma colon.
- They are synchronous carcinoma, metachronous carcinoma, and familial colorectal carcinoma.
Synchronous Carcinoma
Moertel’s definition:
- Synchronous cancers as those occurring within 6 months of the first primary cancer, or two or more histologically distinct simultaneously detected malignancies or more than one malignancy at the time of initial diagnosis.
- This will happen especially in cases of the colon and upper aerodigestive tract wherein the stimulus or aetiological factor for malignancy affects different parts of the organ.
- The colon, head and neck, and oesophagus are the sites of synchronous carcinomas.
- In cases of carcinoma colon with specific aetiological factors such as familial polyposis coli, ulcerative colitis, and hereditary non-polyposis cancer, often carcinoma is synchronous.
- Thus, it is important to do a complete colonoscopy when a patient comes with colonic carcinoma because he/she may be having another synchronous carcinoma elsewhere.
Large Intestine clinical notes:
- A 68-year-old lady was admitted with a large bowel obstruction. A plain X-ray abdomen showed intestinal obstruction.
- An exploratory laparotomy was done. A 3 cm constricting growth was identified at the rectosigmoid junction and high anterior resection and anastomosis were done. On the 4th postoperative day, the patient was allowed a liquid diet.
- Distension increased. For another 3 days, distension went on increasing. A plain X-ray abdomen revealed obstruction with more gas than before. The patient was having colicky abdominal pain.
- An exploratory laparotomy was done. Findings at 2nd laparotomy— anastomosis was intact. The transverse colon was hugely dilated. Careful palpation of the splenic flexure revealed one more growth. A resection and anastomosis were done again.
- The patient was discharged after 10 days. The first surgeon agreed that after finding the rectosigmoid growth, he did not look for any other lesions (mistake). This was obviously a case of synchronous carcinoma.
Enhanced Recovery Programme (ERAS)
Enhanced Recovery After Surgery (ERAS)
- It is also described as ERP (enhanced recovery programme), also called fast track surgery.
- Traditionally hospital stay following colorectal surgery is about 10–14 days. Now, with a few important steps taken in the pre-, peri- and postoperative periods, it is possible to decrease hospital stay to 2–5 days.
Preoperative Steps:
- Metabolic response to injury/surgery produces increasing metabolic demands and nitrogen consumption. A few days into the postoperative period, there will be a catabolic phase resulting in loss of muscle mass.
- Carbohydrate loading done a few hours before surgery decreases postoperative complications by decreasing postoperative insulin resistance and negative nitrogen balance.
- Only patients with anterior resection need to have bowel preparation. For all other colonic surgery, a single enema is more than enough.
Perioperative Steps:
Laparoscopic surgery gives the best results in the form of less pain, fewer wounds, less manipulation, less handling of the bowel, no exposure to the environment. (Thus recovery is fast.) Anaesthetic requirements are less including analgesia.
- Avoid long-acting narcotic analgesics.
- Avoid pre-medication.
- Mid-thoracic epidural block can be offered.
- Avoid tubes and catheters such as nasogastric tube (Ryle’s tube) unless there is distension, postoperative drains (unless suspicious of doubtful anastomosis).
- Avoid central line and arterial lines.
- Preoperative-fluid restrictions—do not overload with water and sodium. Fluids should be less than 2 litres.
- Meticulous technique decreases the time taken for surgery, decreases in number of ports and small incisions for retrieval of specimen—all matters in ERAS.
Postoperative Steps:
- Analgesics should be planned well—epidural blocks.
- Early mobilisation.
- Look for ileus/complications. If present, one should be ready to manage.
- Early feeding—carbohydrate liquids.
Postoperative Chemotherapy
- pT1-2N0M0 do not require any adjuvant treatment, such patients can be kept on follow-up with routine 3 monthly CEA and annual CECT thorax/abdomen/ pelvis.
- pT3N0M0 or node-positive disease requires adjuvant treatment in the form of concurrent chemoradiotherapy and chemotherapy. 2 cycles of FOLFOX (5- FU + Leucovorin + Oxaliplatin) → Concurrent 5-FU/ Leucovorin and radiation → 2 more cycles of FOLFOX. Oral Capecitabine can be used in place of IV 5-FU.
- It is preferable to add Oxaliplatin in the chemotherapy regimen if nodes are positive for metastatic disease. In older population (>65–70 years), it might be of less benefit.
- Oxaloplatins have been shown to downsize liver metastasis. A chief complication of Oxaliplatin is peripheral neuropathy.
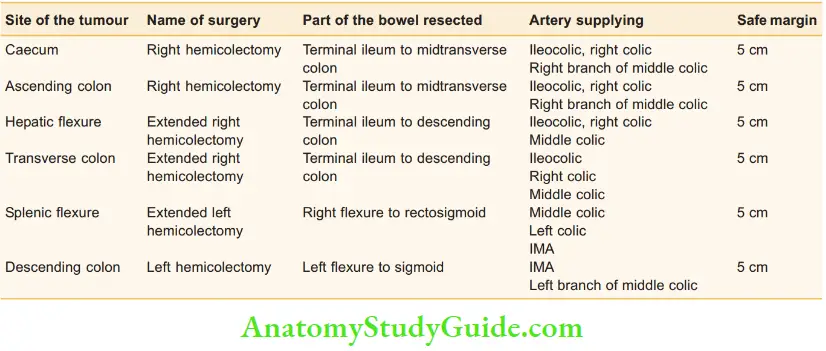
Sugeries In A Case Of Carcinoma Colon
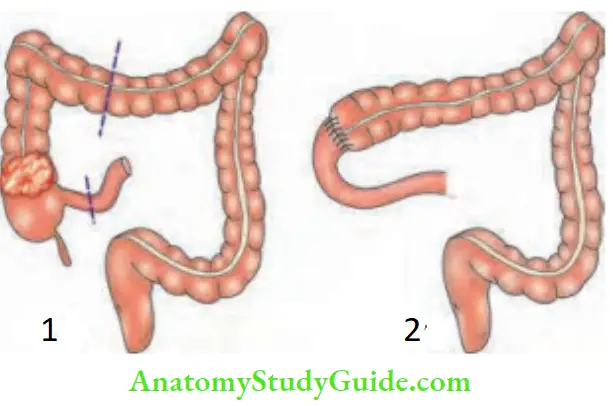
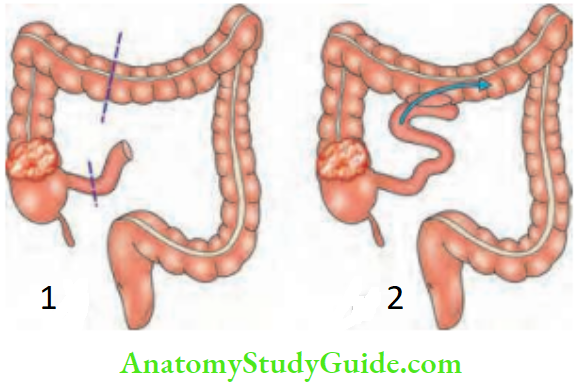
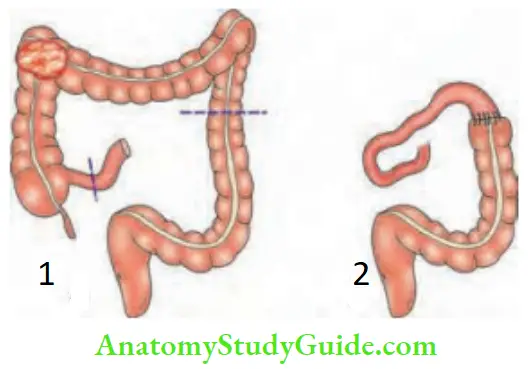
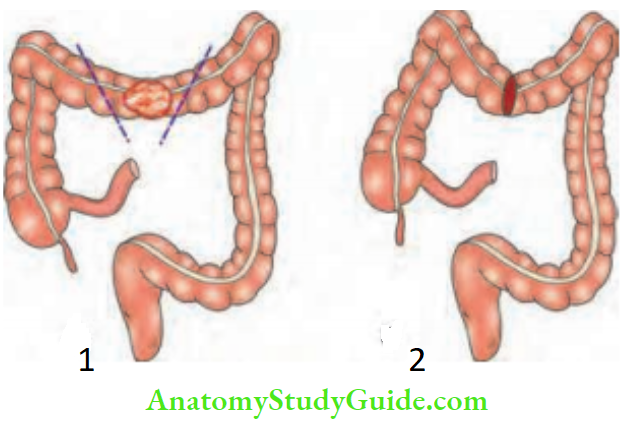
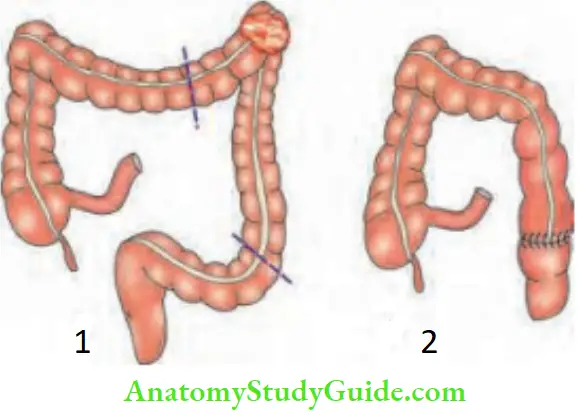
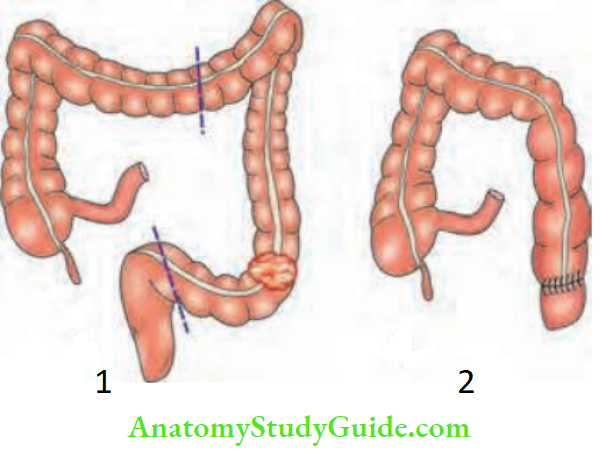
Summary of the resections for carcinoma colon:
Postoperative Radiotherapy
- Adenocarcinoma colon does not respond well to radiation. Routinely, it is not given. The small bowel is adjacent to the large bowel so it cannot tolerate high doses of radiation without developing radiation enteritis.
- Surgery remains the gold standard for carcinoma colon. Soft tissue infiltration into the psoas muscle or abdominal wall or inoperable recurrent tumours are indications for radiotherapy.
Colonic Structure
Colonic Structure Causes:
- Malignant: Adenocarcinoma colon is the commonest cause of stricture colon (rarely lymphomas, carcinoid).
- Tuberculosis: Uncommon cause of stricture in the ascending colon.
- Ischaemic: Uncommon/rare cause—left colon may be affected.
- Inflammatory bowel disease: Any ulcers, including amoebic, may heal with fibrosis resulting in stricture.
- Diverticular stricture
- Radiation stricture
- Endometriomas: Ectopic endometriosis tissue responds to cyclic hormonal stimulation causing inflammation and fibrosis.
Colonic Structure Clinical Features:
- Progressive constipation
- Change in bowel habits
- Bleeding per rectum
- Features of large bowel obstruction
- Mass may/may not be felt
Colonic Structure Investigation: Colonoscopy and biopsy
Colonic StructureTreatment:
- Single-stage resection and end-to-end anastomosis.
- Treatment of the cause.
Leave a Reply