Tumours Of The Biliary Tract
Benign Tumours
- Benign tumours such as papilloma, adenoma, adenomyoma, fibroma, lipoma, myxoma, and haemangioma have been described in the biliary tract but all of them are exceedingly rare.
- Adenomyoma is a more common benign tumour than the rest. All these tumours resemble their counterparts in morphology elsewhere in the body.
Malignant Tumours
- Carcinoma of the gallbladder and carcinoma of the bile ducts and ampulla of Vater are among the more frequent malignant tumours of the biliary tract.
Carcinoma of the Gallbladder
- Primary carcinoma of the gallbladder is more prevalent than other cancers of the extrahepatic biliary tract.
- Like cholelithiasis and cholecystitis, it is more frequent in women than in men (ratio 4:1) with a peak incidence in 7th decade of life. It may remain undetected until the time it is widely spread and rendered inoperable.
Aetiology A number of etiologic factors have been implicated.
1. Cholelithiasis and cholecystitis The most significant association of cancer of the gallbladder is with cholelithiasis and cholecystitis, though there is no definite evidence of a causal relationship.
- Cholelithiasis and cholecystitis are present in about 75% of cases of gallbladder cancer. On the other hand, the incidence of documented gallbladder cancer in the presence of cholelithiasis and cholecystitis is about 0.5% only.
- Porcelain gallbladder is particularly likely to become cancerous.
2. Chemical carcinogens A number of chemical carcinogens structurally similar to naturally occurring bile acids have been considered to induce gallbladder cancer.
- These include methyl phenanthrene, various nitrosamines and pesticides. Workers engaged in the rubber industry have a higher incidence of gallbladder cancer.
3. Genetic factors There is a higher incidence of cancer of the gallbladder in certain populations living in the same geographic region suggesting a strong genetic component in the disease.
- Japanese immigrants and Native Americans of South-Western America have increased frequency while American Indians and Mexicans have lower incidence.
4. Miscellaneous Patients who have undergone previous surgery on the biliary tract have a higher incidence of subsequent gallbladder cancer.
- Patients with inflammatory bowel disease (ulcerative colitis and Crohn’s disease) have a high incidence of gallbladder cancer.
Morphologic Features The commonest site is the fundus, followed next in frequency by the neck of the gallbladder.
Grossly, cancer of the gallbladder is of 2 types infiltrating and fungating type:
- The infiltrating type appears as an irregular area of diffuse thickening and induration of the gallbladder wall.
- It may have deep ulceration causing direct invasion of the gallbladder wall and liver bed. On section, the gallbladder wall is firm due to scirrhous growth.
- Fungating type grows like an irregular, friable, papillary or cauliflower-like growth into the lumen as well as into the wall of the gallbladder and beyond.
Histologically, the following patterns are observed:
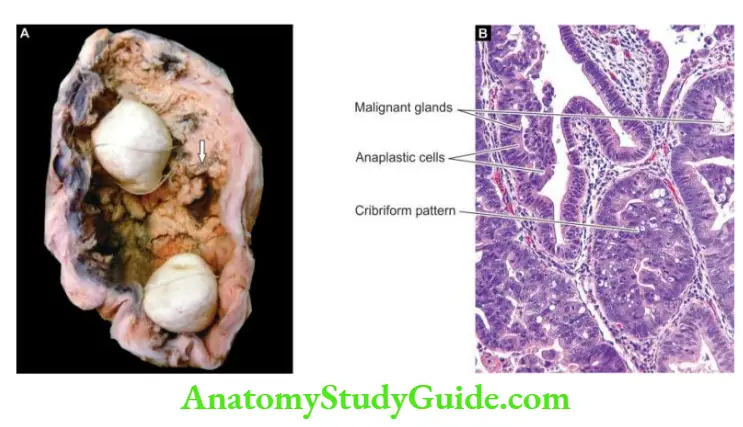
- Most gallbladder cancers are adenocarcinomas (90%). They may be papillary or infiltrative, cribriform, well-differentiated or poorly-differentiated, intestinal, biliary or gastric foveolar type.
- Most are non-mucin secreting but some are mucinous carcinomas forming mucus pools. Perineural invasion carries prognostic significance in Gall bladder adenocarcinoma.
- About 5% of gallbladder cancers are squamous cell carcinomas arising from the squamous metaplastic epithelium.
- A few cases show both squamous and adenocarcinoma patterns of growth called adenosquamous.
Clinical Features Carcinoma of the gallbladder is slow-growing and causes symptoms late in the course of the disease. Quite often, the diagnosis is made when the gallbladder is removed for cholelithiasis.
- The symptomatic cases have pain, jaundice, noticeable mass, anorexia and weight loss.
- In such cases, the growth has usually invaded the liver and other adjacent organs and has metastasised to regional lymph nodes and more distant sites such as the lung, peritoneum and gastrointestinal tract.
Carcinoma of Ampulla of Vater and Extrahepatic Bile Ducts
- In its pure form, the term ampullary carcinoma is used for adenocarcinoma located in the ampulla of Vater, and often its origin from pre-existing villous or tubulovillous adenoma of the ampulla may be demonstrable.
However, when the tumour is advanced, it is indistinguishable from 3 other cancers in the vicinity:
- cancer of adjacent duodenal mucosa with secondary involvement of ampulla;
- cancer of the terminal third of the bile duct infiltrating in the ampulla; and
- carcinoma of the head of a pancreas merging into the ampulla.
Therefore, in advanced cancer involving the ampulla, the term periampullary carcinoma is used that encompasses cancer from all 4 anatomic sites
- ampulla of Vater,
- duodenum,
- the terminal part of the common bile duct, and
- the head of the pancreas.
Unlike other diseases of the biliary passages, this cancer is more common in males with a peak incidence in 6th decade of life.
Etiology Ampullary carcinoma frequently arises from a pre-existing polyp in the ampulla, or maybe a part of familial adenomatous polyposis, Gardner’s Syndrome or neurofibromatosis type
- Unlike gallbladder carcinoma, there is no association between carcinoma of the common bile duct and gallstones.
- Instead, bile duct cancers are associated with a number of other conditions such as ulcerative colitis, sclerosing cholangitis, parasitic infestations of the bile ducts with Fasciola hepatica (liver fluke), Ascaris lumbricoides and Clonorchis sinensis.
Morphologic Features Ampullary carcinoma may be centred on the ampulla bulging into the duodenum (intra-ampullary carcinoma) or may form circumferential growth around the ampulla (periampullary carcinoma).
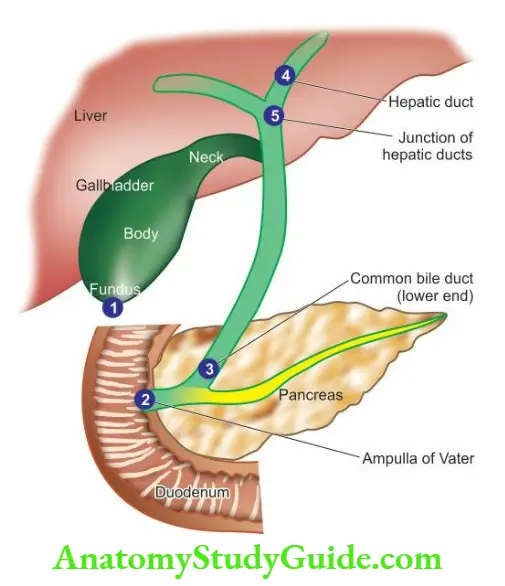
- Extrahepatic bile duct carcinoma may arise anywhere in the biliary tree but the most frequent sites, in descending order of frequency, are:
- the ampulla of Vater, the lower end of the common bile duct, hepatic ducts, and the junction of hepatic ducts to form the common bile duct.
Grossly, ampullary carcinoma projects into the duodenal lumen and has a papillary surface. Bile duct carcinoma is usually small, extending for 1-2 cm along the duct, producing a thickening of the affected duct.
- Histologically, the tumour is usually adenocarcinoma varying from well-differentiated to poorly differentiated and may or may not be mucin-secreting. Perineural invasion is frequently present.
Clinical Features Obstructive jaundice is the usual presenting feature which is characterised by intense pruritus. Pain, steatorrhoea, weight loss and weakness may be present.
- The tumour usually metastasises to the regional lymph nodes. The prognosis of ampullary carcinoma is better than pancreatic cancer and bile duct carcinoma.
Tumours of the Biliary Tract
- Primary carcinoma of the gallbladder is more prevalent than other cancers of the extrahepatic biliary tract and is usually adenocarcinoma.
- Extrahepatic bile duct carcinoma and carcinoma of the ampulla of Vater are less frequent and
has varying grades of differentiation.
Leave a Reply