Duodenum Pancreas And Portal Vein
Duodenum
Question 1. Describe the duodenum under the following headings:
Table of Contents
- Introduction
- Parts
- Relations of 2nd part
- Development of 2nd part
- Arterial supply of 2nd part
- Interior of 2nd part and
- Applied anatomy.
Answer:
1. Duodenum Introduction:
- Duodenum is the proximal, shortest, widest, and most fixed part of the small intestine.
- It extends from pylorus to the duodenojejunal flexure.
- It is 25 cm long and lies opposite to L1, L2, and L3 vertebrae.
- It is C-shaped and curved around the head of the pancreas.
- It is devoid of mesentery.
Read And Learn More: Anatomy Question And Answers
Note: The term duodenum is the Latin corruption of the Greek word vodka action, meaning 12 fingers.
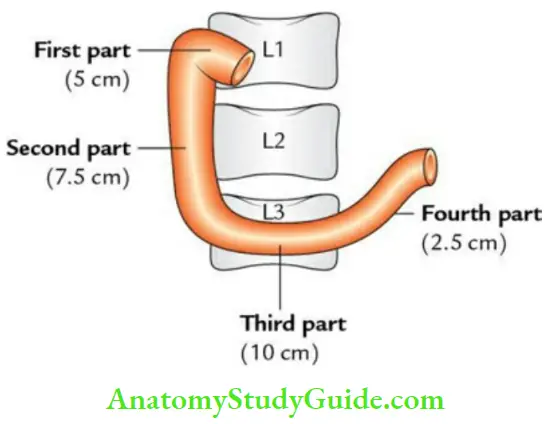
2. Duodenum Parts:
- The first part, 5 cm long
- The second part, 7.5 cm long
- The third part, 10 cm long
- The fourth part, 2.5 cm long
3. Duodenum Relations of 2nd part :
Peritoneal relations:
- It is retroperitoneal and fixed.
- Its anterior surface is covered with peritoneum except near the middle where it is related directly to the colon.
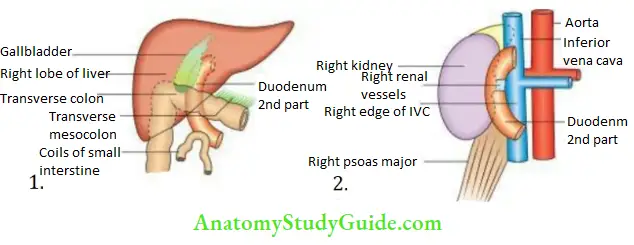
Visceral relations:
- Anterior:
- The right lobe of the liver
- The root of the transverse mesocolon
- Small intestine:
- Posterior:
- Right kidney
- Right renal vessels
- Inferior vena cava
- Right psoas major
- Medial:
- Head of pancreas
- Bile duct
- Lateral: Right colic flexure
4. Duodenum Development of 2nd part:
The upper half(i.e., up to the opening of the bile duct) develops from the foregut and the lower half (i.e., distal to the opening of bile duct) develops from the midgut.
Note: The mucous membrane is derived from the endoderm of the gut, while musculature is from the splanchnic layer of the lateral plate mesoderm.
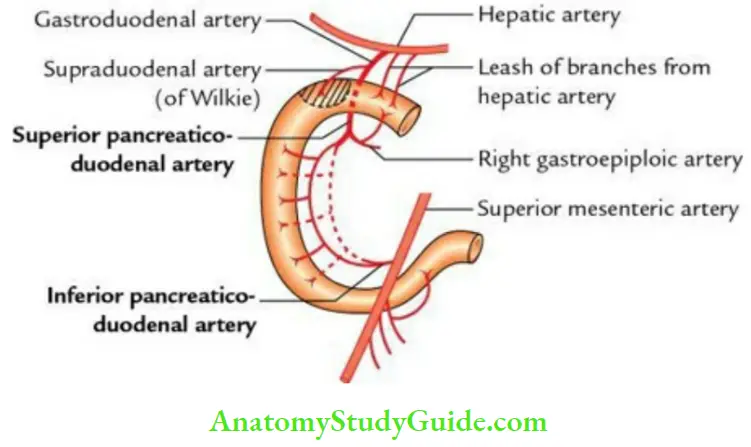
5. Duodenum Arterial supply of 2nd part:
- Above the opening of the bile duct, by the superior pancreaticoduodenal artery (from artery of the foregut).
- Below the opening of the bile duct, by the inferior pancreaticoduodenal artery (from artery of midgut).
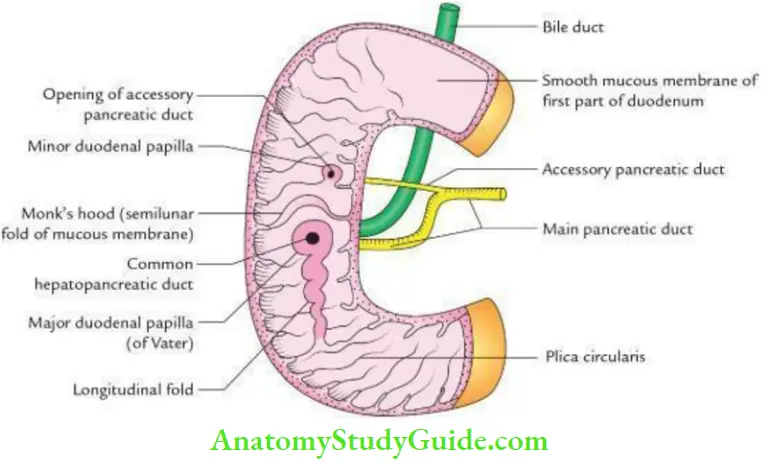
6. Duodenum Interior of 2nd part: It presents two important features
- Major duodenal papilla:
- Major duodenal papilla 8 to 10 cm distal to pylorus
- The main pancreatic duct along with the bile duct (also called hepatopancreatic duct) opens on its summit.
- Minor duodenal papilla:
- Minor duodenal papilla 6 to 8 cm distal to pylorus
- An accessory pancreatic duct opens on its summit.
7. Duodenum Applied Anatomy:
- The first part of the duodenum: Duodenum is vulnerable to peptic ulceration due to direct exposure to acidic chyme from the stomach. It may erode the gastroduodenal artery leading to severe hemorrhage.
- Duodenal obstruction: It may occur due to congenital stenosis, annular pancreas, compression by the superior mesenteric artery, or contraction of the suspensory muscle of duodenum.
- Duodenal: Duodenal diverticula are fairly common along the concave border at the points of entry of arteries in the duodenal wall.
Question 2. Draw a labeled diagram to show the internal features of the duodenum.
Answer:
It is drawn below:
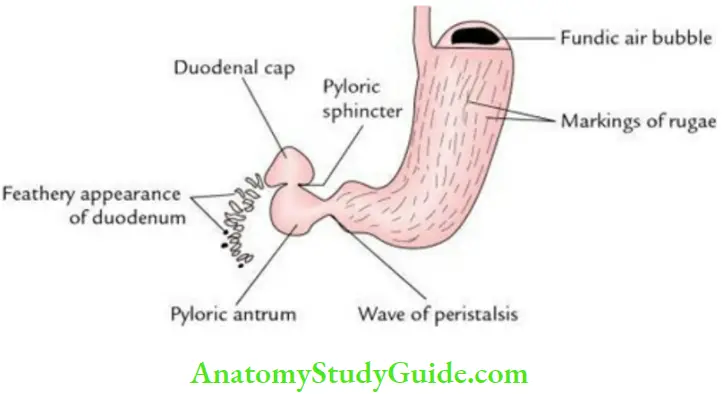
Question 3. Write a short note on the duodenal cap.
Answer:
- The duodenal cap is a radiopaque triangular shadow of the 1st part of the duodenum seen in the barium meal X-ray abdomen. It is formed due to the following factors:
- The first part of the duodenum runs upward, backward, and to the right to continue as the second part.
- The mucous membrane of the first part of the duodenum is smooth, i.e. devoid of circular folds.
- Knoblike pylorus invaginates into the first part of duodenum which keeps this part open so that it is filled with barium paste.
- The viscosity of the barium paste coming out of the narrow pyloric canal into the 1st part of the duodenum gives a conical appearance.
- The proximal half of the 1st part of the duodenum is mobile because it has mesentery.
Question 4. Write a short note on the ligament of Treitz.
Answer:
- It is a fibromuscular band that extends from the right crus of the diaphragm to the duodenojejunal flexure.
- It is formed:
- In the upper part by skeletal muscle fibers.
- In the middle part by elastic fibers.
- In the lower part by smooth muscle fibers.
Its length determines the shape of the duodenum, viz., C-shaped, J-shaped, or O-shaped.
Ligament of Treitz Applied Anatomy:
- It helps surgeons to identify the duodenojejunal junction.
- Its contraction may cause the narrowing of the angle of the duodenojejunal flexure leading to partial intestinal obstruction.
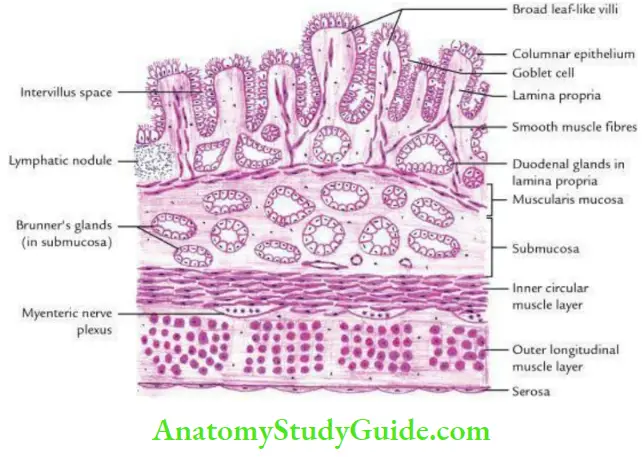
Question 5. Describe the histological features of the duodenum.
Answer:
- A histological section of the duodenal wall presents 4 layers from within outward; these are:
- Mucosa consists of lining epithelium, lamina propria, and muscularis mucosae.
- Lining epithelium is made up of columnar cells interspersed with goblet cells.
- Mucosa presents numerous short leaf-like projections of varying heights called villi.
- Each villus has a core of lamina propria and stands for smooth muscle fibers from muscularis mucosae.
- Muscularis mucosae is thin and made up of two layers of smooth muscle fibers.
- Submucosa presents extensive aggregations of mucous-secreting tubuloalveolar glands (Brunner’s glands).
- Muscularis externa consists of two layers of smooth muscle fibers – an inner circular and an outer longitudinal.
- The serous layer is a single layer of the squamous cells resting on the basement membrane.
Pancreas
Question 6. Describe the pancreas under the following headings:
- Introduction
- Location
- Parts
- Ducts
- Blood supply and
- Applied anatomy
Answer:
1. Pancreas Introduction:
- Pancreas is a soft-lobulated, elongated (15–20 cm long) exoendocrine gland.
- The exocrine part secretes pancreatic juice, while the endocrine part secretes insulin, glucagon, etc.
- It is J-shaped/retort-shaped and set obliquely.
2. Pancreas Location:
It lies retroperitoneally more or less transversely on the posterior abdominal wall at the level of the L1 and L2 vertebrae.
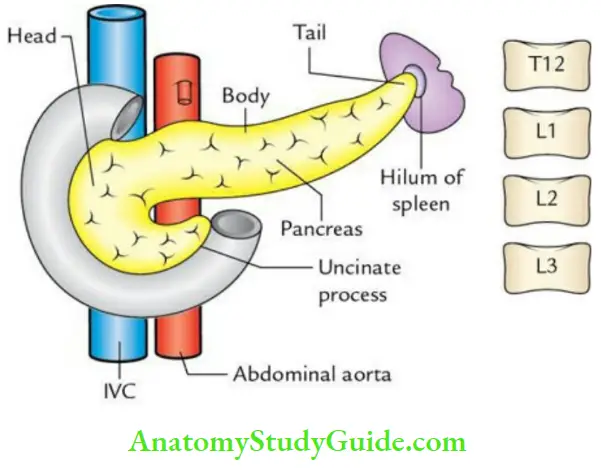
3. Pancreas Parts:
From right to left, the pancreas is divided into 4 parts:
- Head
- Neck
- Body
- Tail
1. Head of the pancreas:
- External features: It is an enlarged right end of the pancreas contained within the C-shaped curve of the duodenum.
- It is flattened from before backward and presents:
- Two surfaces: Anterior and posterior.
- Four borders: Superior, inferior, right, and left.
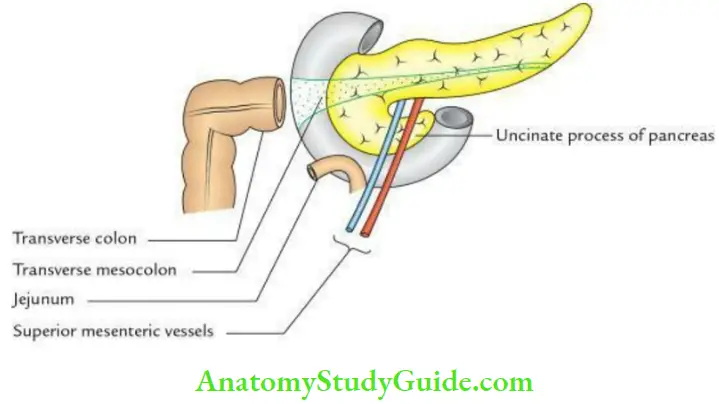
- One process: Uncinate process.
- It is flattened from before backward and presents:
- Relations:
- Posteriorly, it is related to 3 structures: From right to left, these are
- Common bile duct (embedded in a pancreatic groove)
- Inferior vena cava and terminal parts of the renal veins
- Aorta
- Anteriorly, it is related to 3 structures:
- Transverse mesocolon
- Coils of jejunum
- Superior mesenteric vessels in front of the uncinate process of the pancreas
- Posteriorly, it is related to 3 structures: From right to left, these are
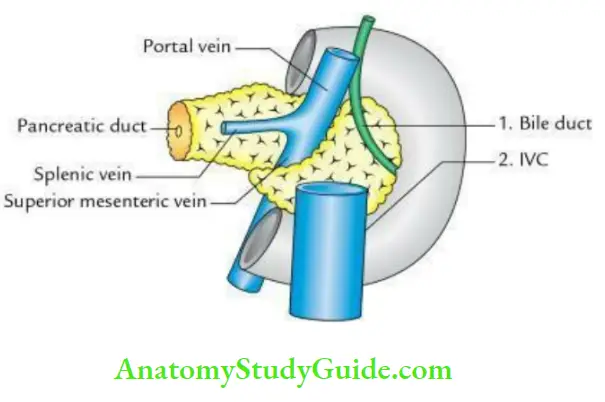
2. Neck of the pancreas:
- External features: It is a slightly constricted part between the head and body. It presents:
- Two surfaces: Anterior and posterior.
- Two borders: Superior and inferior.
- Relations:
- Posteriorly, it is related to 3 veins: termination of the splenic and superior mesenteric veins, and beginning of the portal vein.
- Anteriorly, it is related to two structures: pylorus and peritoneum covering the posterior wall of the lesser sac.
3. Body of pancreas:
- External features: It is prismoid in appearance and appears triangular in cross-section. It is directed slightly upward and backward. It presents:
- Three borders: Anterior, superior, and inferior
- Three surfaces: Anterior, inferior, and posterior
Note: A part of the body, a little to the left of the neck projects upward, and is called tuber mental.
- Relations:
- Anterior surface: It is related to 3 structures:
- Lesser sac and stomach.
- Splenic artery along its upper border.
- Transverse mesocolon attached to its lower border.
- Inferior surface: It is related to 3 structures. From right to left, these are:
- Duodenojejunal flexure
- Loops of jejunum
- Transverse colon
- Posterior surface: It is related to 3 structures:
- Left crus of the diaphragm
- Left psoas major (and the structures related to it)
- Left kidney
- Anterior surface: It is related to 3 structures:
4. The tail of the pancreas:
- External features: It is the narrow left extremity of the pancreas which along with splenic vessels lies within the lienorenal ligament.
- Relations:
- In front: Stomach (separated by the lesser sac)
- Behind: Spleen and splenic vessels
- Below: Left colic flexure
4. Pancreas Ducts:
The exocrine part of the pancreas is drained by two ducts:
Main pancreatic duct (duct of Wirsung):
- It lies near the posterior surface of the pancreas.
- It begins at the tail of the pancreas and runs toward the right through the body.
- At the neck, it bends to run downward, backward, and to the right in the head. Its lumen is about 3 mm in diameter.
- It receives numerous small tributaries, at right angles to its long axis in a herringbone pattern.
- In the head of the pancreas, it lies to the left of the bile duct.
- The two ducts enter the wall of the 2nd part of the duodenum.
- Here, they join to form the hepatopancreatic ampulla of Vater, which opens on the summit of the major duodenal papilla (8–10 cm distal to pylorus).
Accessory pancreatic duct (duct of Santorini):
- It begins in the lower part of the head, crosses in front of the main duct, and opens into the 2nd part of the duodenum at the summit of minor duodenal papilla (6–8 cm distal to pylorus).
- The accessory pancreatic duct communicates with the main duct.
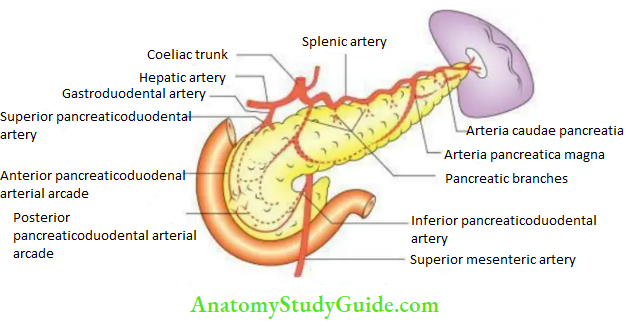
5. PancreasBlood supply:
- Arterial supply
- The upper halfofthe head is supplied by the superior pancreaticoduodenal artery, a branch of the gastroduodenal artery (from the coeliac trunk).
- The lower halfofthe head and its uncinate process is supplied by the inferior pancreaticoduodenal artery (from the superior mesenteric artery).
- The neck, body, and tail are supplied by the pancreatic branches of the splenic artery
(from coeliac trunk).
- Venous drainage:
- It is done by the superior and inferior pancreaticoduodenal veins.
- The superior pancreaticoduodenal vein drains into the portal vein.
- The inferior pancreaticoduodenal vein drains into a superior mesenteric vein.
6. Pancreas Applied anatomy:
- Carcinoma head of pancreas: Carcinoma pancreas is common in 80% of cases.
- It involves the head. Clinically, it presents as:
- Obstructive jaundice, due to pressure on bile duct and hepatopancreatic ampulla.
- Ascites, due to pressure on portal vein.
- Pyloric obstruction, due to pressure on pylorus.
- It involves the head. Clinically, it presents as:
Note: The prognosis of carcinoma head of the pancreas is very poor due to widespread metastasis along the retroperitoneal channels.
- Acute pancreatitis: It is a serious disease and occurs secondary to mumps. It may cause a collection of fluid in the lesser sac called the pseudocyst of the pancreas.
- Referred pain of pancreas:
- The pancreatic pain is referred to T6–T10 dermatomes on the front of the abdomen.
- However, the involvement of the local parietal peritoneum can cause severe pain in the middle of the back.
Question 7. Describe the histological features of the pancreas
Answer:
The pancreas is exoendocrine gland. The exocrine part secretes pancreatic juice, while the endocrine part secretes hormones like insulin and glucagon.
A histological section through the pancreas presents the following features:
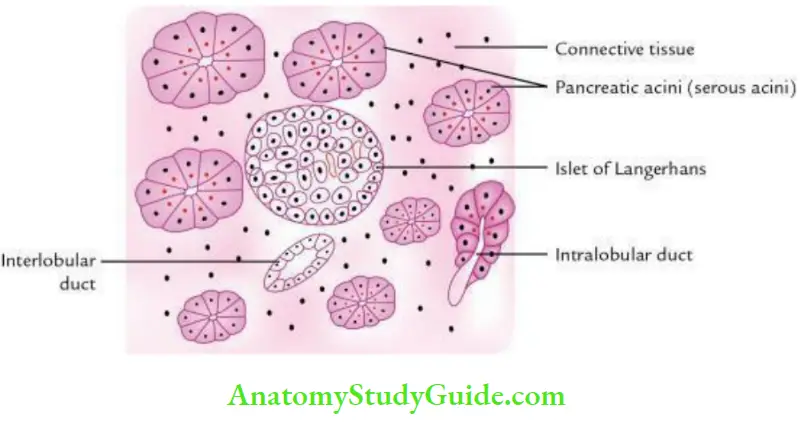
1. Pancreas Exocrine part:
Consists of: Masses of closely packed, darkly stained serous acini called pancreatic lobules.
- Cells lining the acini are truncated pyramidal shaped.
- Cells of acini possess round nuclei located near the base.
- Cells of acini have basal basophilia (dark stain) and apical eosinophilia (light stain).
- The Lumen of acini is hardly visible.
Ducts of various sizes in connective tissue between the lobules.
The ducts may be:
- Intercalated
- Intralobular, lined by cuboidal cells
- Interlobular, lined by columnar cells
Note: Cells of duct are better defined than the cells of acini.
2. Endocrine part:
Consists of large lightly stained ellipsoidal areas called islets of Langerhans scattered throughout the acinar tissue.
- Islets of Langerhans are made up of clumps of small poorly stained cells.
- Cells of islets are arranged in regular cords.
- Presence of fenestrated capillaries in between the cells.
- Cells of islets are of two main types: α (alpha) and β (beta).
- Alpha cells (20%) are present at the periphery, while beta cells (80%) are present in the central part.
Question 8. Describe the development of the pancreas and associated congenital anomalies in brief.
Answer:
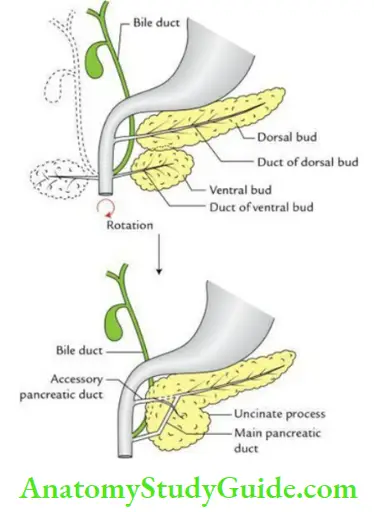
Development of pancreas:
The pancreas develops from two buds called dorsal and ventral pancreatic buds, which arise at the junction of the foregut and midgut. These buds soon unite to form the pancreas.
- Larger dorsal bud forms:
- Part of the head
- Whole of neck
- The whole body and
- Whole of tail
- Smaller ventral bud forms:
- The lower part of the head and
- Uncinate process
- The main pancreatic duct is formed by: The duct of the dorsal bud
- The accessory pancreatic bud is formed by: The duct of the ventral bud
Congenital anomalies
- Annular pancreas:
- It is a condition in which pancreatic tissue encircles the 2nd part of the duodenum and leads to duodenal obstruction.
- It occurs when the right and left parts of the bifid ventral pancreatic bud fail to fuse and the right bud migrates along the normal route, while the left part migrates in the opposite direction.
- As a result, the 2nd part of the duodenum becomes completely surrounded by the pancreatic tissue.
Accessory pancreatic tissue: The ectopic pancreatic tissue may be found in
- Gall bladder
- Stomach
- Spleen
- Small intestine
- Meckel’s diverticulum
Portal vein
Question 9. Describe the portal vein under the following headings:
- Introduction
- Formation
- Course
- Termination
- Parts
- Relations
- Tributaries and
- Applied anatomy.
Answer:
1. Portal Vein Introduction:
- The portal vein is the large vein (about 8 cm long and 2 cm wide) of the abdomen.
- It collects the blood from the gall bladder, pancreas, spleen, and abdominal part of the gastrointestinal tract and conveys it to the liver from where it is drained into the inferior vena cava through hepatic veins.
- It is called a portal vein because it begins in one set of capillaries (gut capillaries) and ends in another set of capillaries (liver sinusoids).
- It conveys absorbed products of the digested food from the intestine to the liver and provides 60–75% nutrition to the liver.
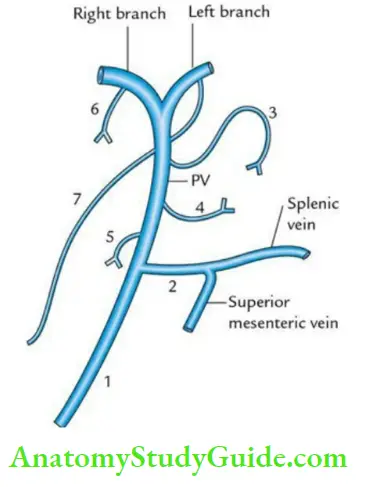
2. Portal Vein Formation:
It is formed by the union of the superior mesenteric and splenic veins behind the neck of the pancreas at the level of the L2 vertebra.
3. Portal Vein Course:
After formation, it runs upward and a little to the right, passing successively behind the neck of the pancreas, the first part of the duodenum, and the right free margin of the lesser omentum.
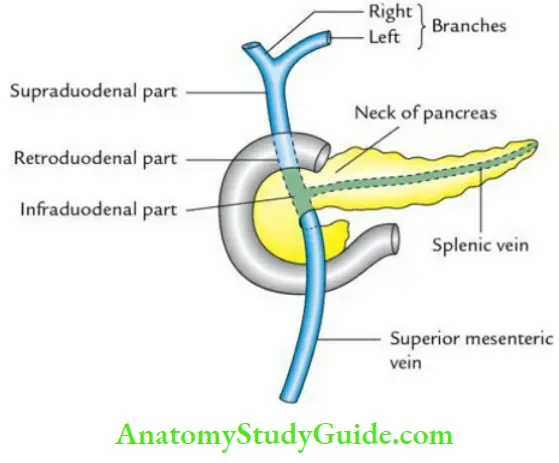
4. Portal Vein Termination
It terminates at the right end of the porta hepatis by dividing into right and left branches. The right branch is shorter and wider and enters the right lobe of the liver. The left branch is longer and narrower. It traverses porta hepatis to reach its left end and enters the left lobe of the liver.
5. Portal Vein Parts:
- The portal vein is divided into 3 parts:
- Infraduodenal part
- Retroduodenal part
- Supraduodenal part
6. Portal Vein Relations:
- Infraduodenal part:
- Anterior: Neck of the pancreas
- Posterior: Inferior vena cava
- Right side: Bile duct
- Retroduodenal part:
- Anterior: First part of the duodenum
- Posterior: Inferior vena cava
- Supraduodenal part:
- Anterior and to the right: Bile duct
- Anterior and to the left: Hepatic artery
- Posterior: Inferior vena cava
7. Portal Vein Tributaries:
8. Portal Vein Applied Anatomy:
- Portal hypertension:
- Normal portal pressure is 5–10 mmHg.
- Portal hypertension is usually caused by cirrhosis of the liver.
- It may lead to congestive splenomegaly, ascites, or complications of collateral circulation at portosystemic anastomoses.
Question 10. Define portocaval anastomoses with their sites and related clinical significance.
Answer:
The portocaval anastomoses are sites of communication between the tributaries of the portal vein and inferior vena cava. These communications form important routes of collateral circulation in portal obstruction.
Sites of portocaval anastomoses:
The 3 important sites of portocaval anastomosis are:
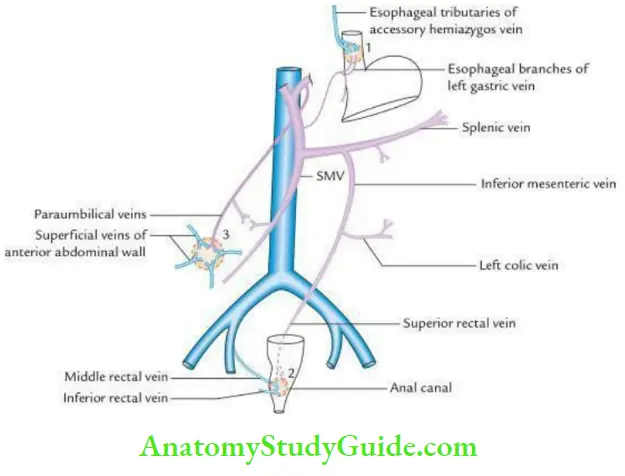
1. Lower end of esophagus:
- Here, the esophageal tributaries of the left gastric vein (a portal tributary) anastomoses with esophageal tributaries of the accessory hemiazygos vein (a systemic tributary).
Applied anatomy: In portal obstruction, these veins become distended and tortuous producing esophageal varices, which may bleed to cause hematemesis.
2. Anal canal:
- In the mid-anal canal close to the pectinate line, the superior rectal vein (a portal tributary) anastomoses with middle and inferior rectal veins (the systemic tributaries).
Applied anatomy: In portal obstruction, the radicals of the superior rectal vein in the anal columns dilate to produce internal hemorrhoids/piles.
3. Umbilicus:
Here paraumbilical vein a tributary of the portal vein anastomoses with the superficial veins of the abdomen-the tributaries of IVC.
Applied anatomy:
- In portal hypertension, the blood from the portal vein is diverted into systemic (caval) tributaries.
- This causes dilatation and tortuosity of caval tributaries, viz. – the superficial veins of the abdomen, which become tortuous and radiate from umbilicus like the spokes of wheel.
- This clinical sign is called caput medusae.
Note: Less important sites of portocaval anastomosis:
- Bare area of the liver: Here, hepatic venules (portal tributaries) are anastomose with the phrenic and intercostal veins (systemic tributaries).
- Posterior abdominal wall: Here, superior mesenteric and inferior mesenteric veins (portal tributaries) draining retroperitoneal organs (viz. duodenum ascending and descending colons) anastomose with retroperitoneal veins draining abdominal wall and renal capsule (systemic tributaries).
Question 11. Give a brief account of the development of the portal vein.
Answer:
- The portal vein develops in the 2nd and 3rd month of intrauterine life, from two vitelline veins (right and left), which lie one on either side of the developing duodenum.
- They soon get interconnected by three anastomotic channels; two ventral and one dorsal. The portal vein develops from these 3 channels.
The various parts of the portal vein derived from these channels are as follows:
- Infraduodenal part, from a left vitelline vein (between the point at which splenic and superior mesenteric veins open and the point where dorsal anastomotic channel joins the left vitelline vein.
- Retroduodenal part, from dorsal venous anastomosis.
- Supraduodenal part, from right vitelline vein between cephalic ventral venous anastomosis and dorsal venous anastomosis.
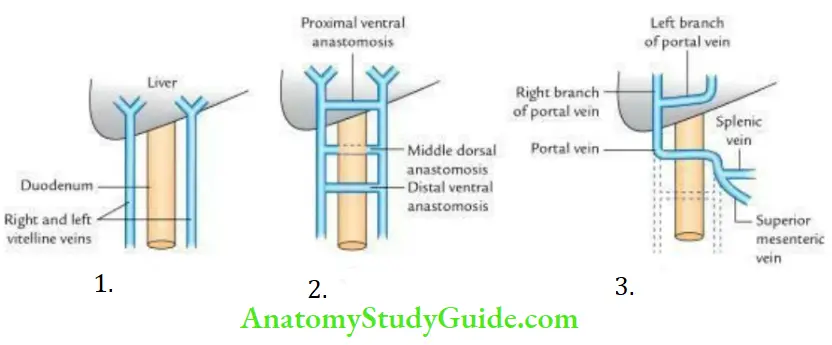
Note:
- The left branch is derived from proximal (cephalic) ventral anastomosis and part of the left vitelline vein cephalic to the ventral anastomosis.
- The right branch is derived from part of the right vitelline vein cephalic to the ventral anastomosis.
Leave a Reply