Antitubercular Agents Introduction
Tuberculosis is a chronic infectious disease caused by various strains of Mycobacterium especially Mycobacterium tuberculosis which is an acid fast aerobic bacillus. It is transmitted via the respiratory route. The organism appears in water droplets expelled during coughing, sneezing or talking. Either in droplet form or through the air, the organism enters the respiratory tract.
Table of Contents
It mainly affects the lungs but can spread through blood stream and lymphatic system to the brain, bones, eyes and skin. In pulmonary tuberculosis the bacilli reach the alveoli and are ingested by pulmonary macrophages. Substance secreted by the macrophages stimulates surrounding fibroblast to enclose the infection site leading to formation of granulomas or tubercles.
Extra pulmonary tuberculosis is much more common in HIV infected patients. The drugs used in the treatment of tuberculosis are called antitubercular agents, which can be divided into two major categories like first line agents and second line agents.
All first line agents have a standard three letter and a single letter abbreviation as follows,
- Ethambutol is EMB or E,
- Isoniazid is INH or H,
- Pyrazinamide is PZA or Z,
- Rifampicin is RMP or R,
- Streptomycin is STM or S.
Drug regimens are similarly abbreviated in a standardized manner. The drugs are listed using their single letter abbreviations. A prefix denotes the number of months the treatment should be given for and a subscript denotes intermittent dosing and no subscript means daily dosing.
Most regimens have an initial high intensity phase, followed by a continuation phase (also called a consolidation phase or eradication phase) and the two phases divided by a slash. So, 2HREZ/4HR3: means Isoniazid, Rifampicin, Ethambutol,
Pyrazinamide daily for two months, followed by four months of isoniazid and rifampicin given three times a week.
Antitubercular Agents Classification
- First line agents. An effective bacterial agent, with an acceptable degree of eg. Isoniazid, Ethambutol, Rifampicin, Streptomycin, Pyrazinamide, Rifabutin. toxicity.
- Second line agents. For microbial resistance or patient related factors. eg. Ethionamide, Aminosalicylic acid, Cycloserine, Amikacin, Capreomycin.
First Line Agents
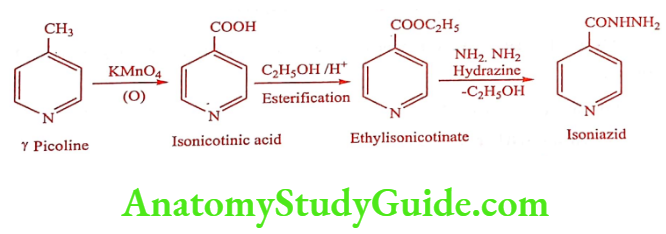
Isoniazid (INH) (Isonex, Tubernex forte, Nydrazid, Laniazid)
Synthesis
Food and various antacids, especially aluminium containing antacids interferes with absorption, therefore it is recommended that the drug to be taken on an empty stomach.
Mechanism of Action: It is a prodrug that is activated through an oxidation reaction catalyzed by an endogenous enzyme catalase peroxidase. The activated INH acylates an enzyme system found exclusively in M.tuberculosis which is essential for the synthesis of mycolic acid.
ADR: Peripheral neuritis and optic neuritis.
Dose: 5mg/kg daily.
Use: Primary drug for treatment of Mycobacterium tuberculosis. It is most potent and selective of the known tuberculostatic antibacterial agent and it is regarded as the most effective agents in the therapy of tuberculosis.
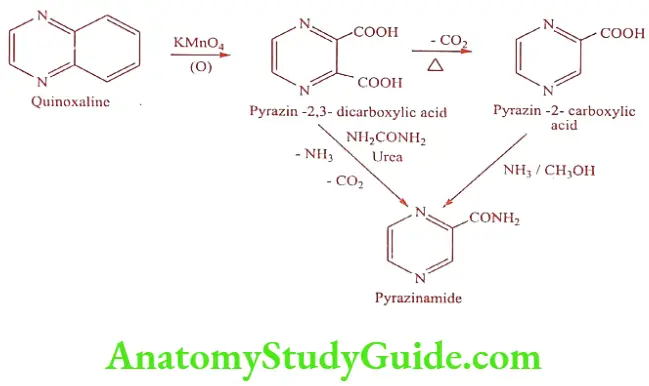
Pyrazinamide (Pyzid, Zypyra)
Synthesis
Mechanism of Action: Pyrazinamide is converted to Pyrazinoic acid by pyrazine amidase produced by susceptible organism. The Pyrazinoic acid lowers the pH of the surrounding M .tuberculosis, to such an extent that the organism is unable to grow.
ADR: Hepatotoxicity and jaundice.
Dose: 75mg/kg twice daily.
Use: It is a secondary tuberculostatic agent used in combination with other antitubercular drugs. It is an essential component of combination therapy.
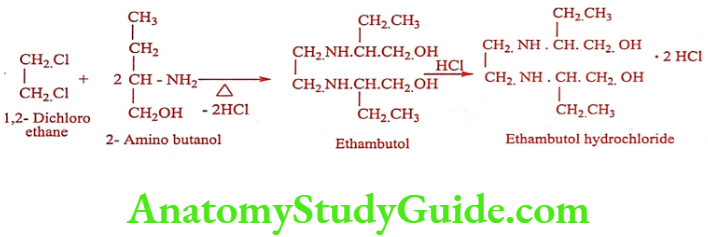
Ethambutol hydrochloride (Mycoback, Mycobutol, Mycobutol)
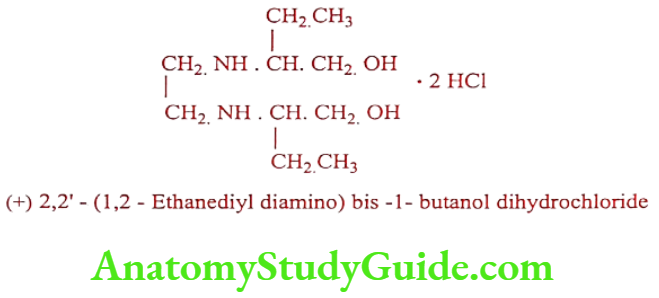
Synthesis
Mechanism of Action: It inhibits Mycobacterial arabinosyl transferase involved in the polymerization of D-arabino furanose to arabino glycan, an essential cell wall component.
ADR: It is not recommended for children under 5years of age. Retrobulbar neuritis with a reduction in visual acuity, constriction of visual field, central or peripheral scotoma and green-red color blindness.
Dose: 15mg/kg/day or 30mg/kg thrice daily.
Use: It is a tuberculostatic drug that is effective against tubercle bacilli resistant to Isoniazid or Streptomycin.
Rifampicin (Rifampin) (LS Rif, Rimpacin)
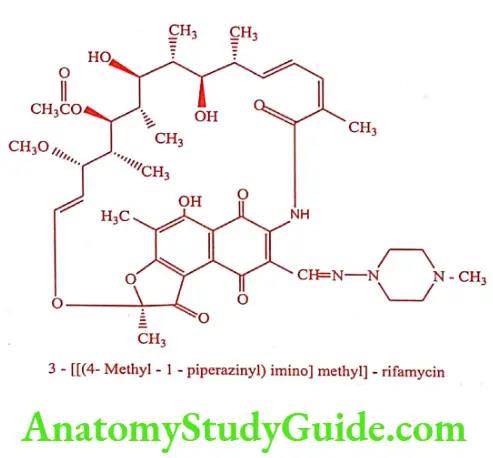
Mechanism of Action: It inhibits bacterial DNA-dependent RNA polymerase (DDRP) and blocks the chain formation of RNA synthesis. It has been suggested that the aromatic naphthalene ring (π-π) bonds to the DDRP
ADR: GI disturbances, skin reaction and eosinophilia. The drug is hepatotoxic and may produce thrombocytopenic purpura.
Dose: 10mg/kg daily or 2 to 3 times weekly.
Use: A broad spectrum antibiotic effective against most of the Gram positive bacteria and variably active against Gram negative organisms. Both Mycobacterium tuberculosis and Mycobacterium leprae are very susceptible to this drug. Its clinical use is mainly in the treatment of tuberculosis. It is not recommended in the treatment of HIV-infected patients, since it decreases the effectiveness of protease inhibitors.
Second Line Agents
Para aminosalicylic acid (Sodium – PAS)
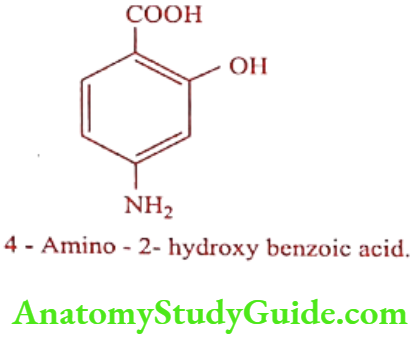
Synthesis
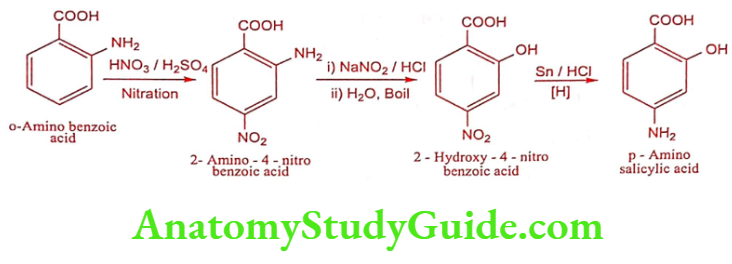
Mechanism of Action: It acts as antimetabolite interfering with the incorporation of PABA into folic acid.
ADR: Nausea, vomiting, GI irritation and diarrhea. Thyroid goiter is also a side effect because amino salicylic acid inhibits the synthesis of thyroid hormones.
Dose: 200mg/kg in divided dose.
Use: It is used in the treatment of tuberculosis. PAS is a bacteriostatic agent, so it only arrest but does not eradicate the tubercle bacilli. Therefore PAS is always used in combination with one or two other antitubercular drugs.
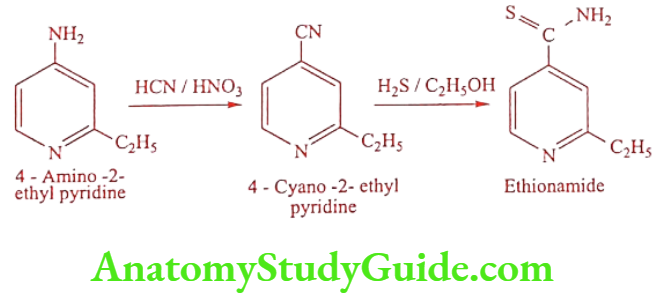
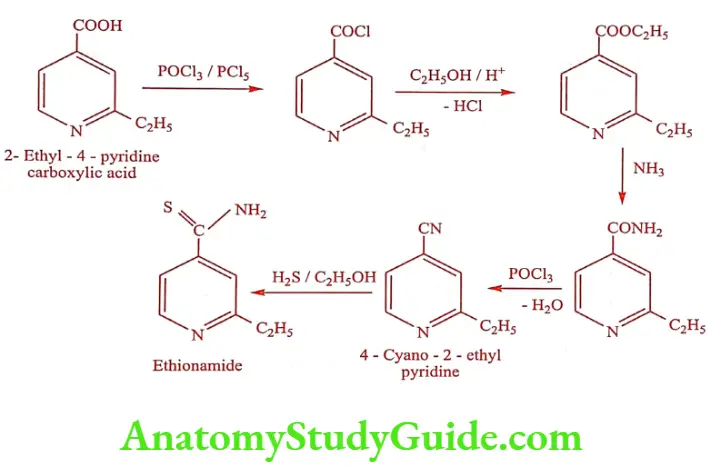
Ethionamide (Ethide, Mycotuf)
Synthesis
Method 1
Method 2
Mechanism of Action: Primary drug for treatment of Mycobacterium tuberculosis. It is most potent and selective of the known tuberculostatic antibacterial agent and it is regarded as the most effective agents in the therapy of tuberculosis.
ADR: Anorexia, excessive salivation and metallic taste.
Dose: 15 to 20mg/kg/day.
Use: It is less potent and more toxic than INH, so its general use should be avoided. It should be used only when the usual combination of Streptomycin, PAS and INH are ineffective or cannot be tolerated.
Cycloserine (Cyclokox, Cyclorine, Seromycin)
It is an antibiotic, isolated from Streptomyces species. The compound slowly dimerizes on standing or in solution.
Synthesis
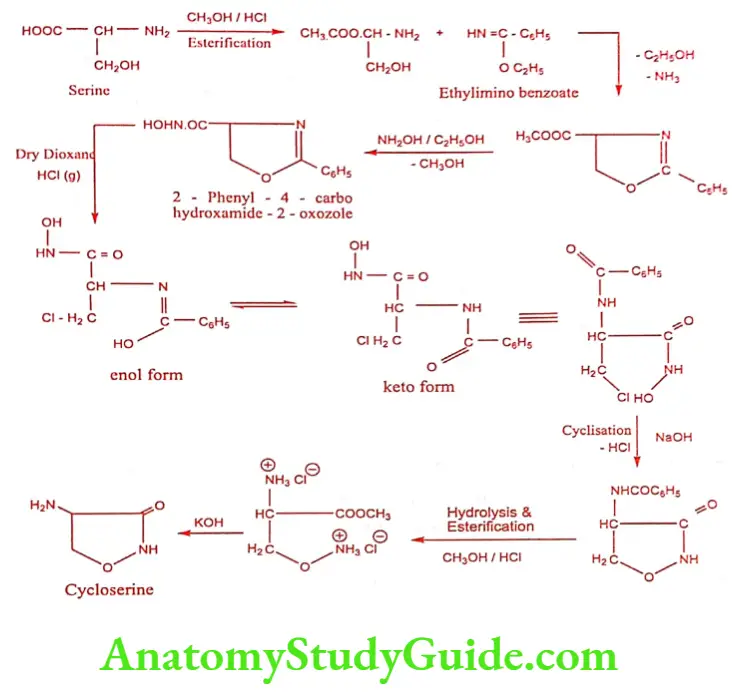
Mechanism of Action: D-alanine is an important component of peptidoglycan portion of the mycobacterial cell wall. The enzyme D-alanine racemase in mycobacterium converts L-alanine to D-alanine further incorporate into peptidoglycan portion by D-alanine ligase. D-cycloserine is an analogue of D-alanine; therefore it competitively inhibits both the enzyme.
ADR: Headache, dizziness and anxiety.
Dose: 250mg bid for 2 weeks.
Use: It is useful in the therapy of tuberculosis resistant to other drugs. It is always combined with other anti-tubercular drug.
Leave a Reply