Cardiovascular Agents
Drugs For The Treatment Of Congestive Heart Failure (or) Cardiac Agents
Congestive heart failure (CHF) is inability of the heart to pump blood effectively at the rate that meets the need of metabolizing tissues. This results in the reduced contractility which causes a decrease in cardiac output, increasing the blood volume of the heart. As a result the systemic and renal blood flow decreases, which causes edema and renal failure.
Table of Contents
Cardiac Glycosides
Cardiac glycosides are important class of naturally occurring drugs used in the treatment of CHF and associated edema. They occur mainly in plants and in animals such as poisonous toads. Digitalis purpurea or the foxglove plants, Digitalis lanata, Strophanthus gratus and Strophanthus Kombe are the major plant sources of cardiac glycosides.
Chemistry of Cardiac Glycosides
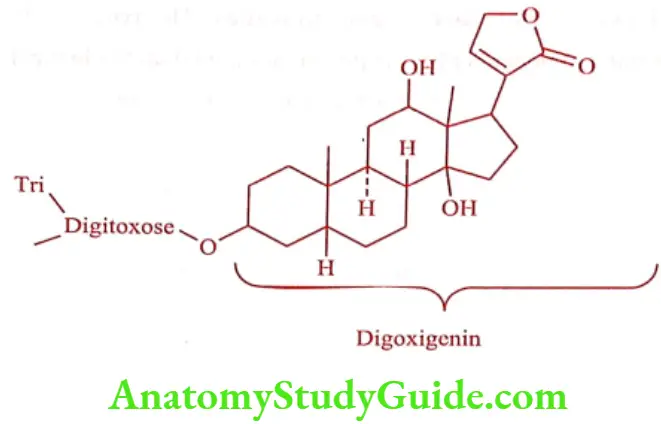
Cardiac glycoside composed of two portions
- Sugar portion (Glycone): Provides favorable solubility and distribution characteristics of the glycoside.
- Non-sugar portion (Aglycone): Responsible for the cardio tonic activity of the glycoside.
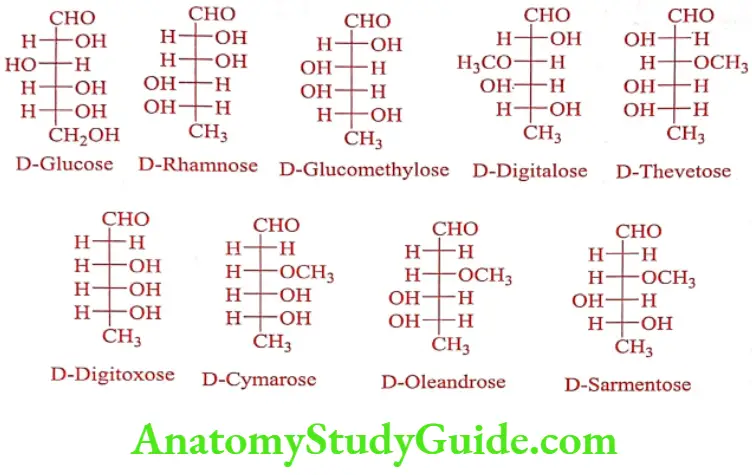
Glycone
The sugars found in the cardiac glycosides are D-Glucose, D-Digitoxose, L-Rhamnose, D-Cymarose, D-Digitalose, L-Thevetose, L-Oleandrose and D-Sarmentose. The number and the identity of sugar moiety vary from one glycoside to another. The sugar usually exists in B-configuration. The sugar (mono or polysaccharide) portion conjugates with the C-3 hydroxy group of the aglycone portion with B-1, 4-glucosidic linkages. The O-acetyl sugar D-Digitalose, L-Thevetose, D-Cymarose, L-Oleandrose and D-Sarmentose are more lipophilic and affect the pharmacokinetics of the glycoside.
Aglycone
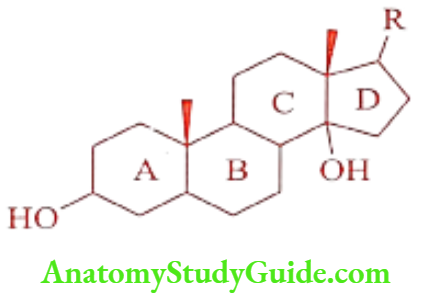
Aglycone portion is a steroid nucleus with a unique set of fused rings. Ring A/B and C/D are as cis fused, whereas ring B/C have a trans configuration. The steroidal nucleus carries two angular methyl groups at C10 and C13. The hydroxyl group at the 3rd position is the site of attachment for the sugar portion.
The C14 hydroxyl group is normally unsubstituted; however additional hydroxyl group may be found at C12 and C16, the presence or absence of which distinguishes the important genus like Digitoxigenin, Digoxigenin and Gitoxigenin.
The size of the unsaturated lactone ring at C17 position varies with the source of glycoside. It is classified into two types.
- Cardenolides
- Bufadienolides
Cardenolides are 5-membered, a, ẞ-unsaturated lactone (butyro lactone) ring, mostly occur in plants. Bufadienolides are 6-membered (a-pyrone) lactone ring with 2-conjugated double bonds and of animal origin.
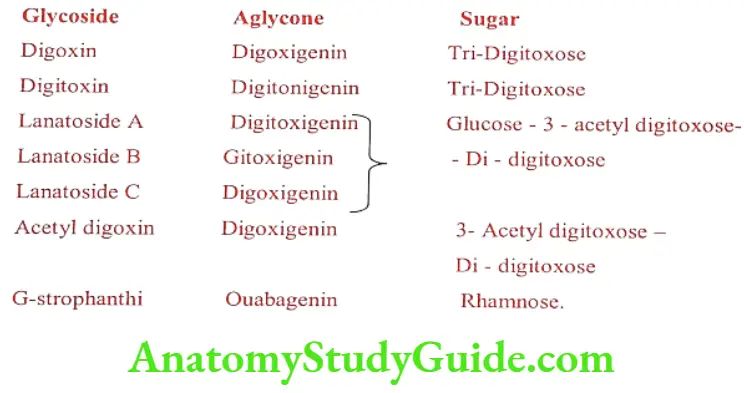
Pharmacologically, both have similar properties. The type of glycoside and the name of the structural components of these glycosides are tabulated in the Table 21.1
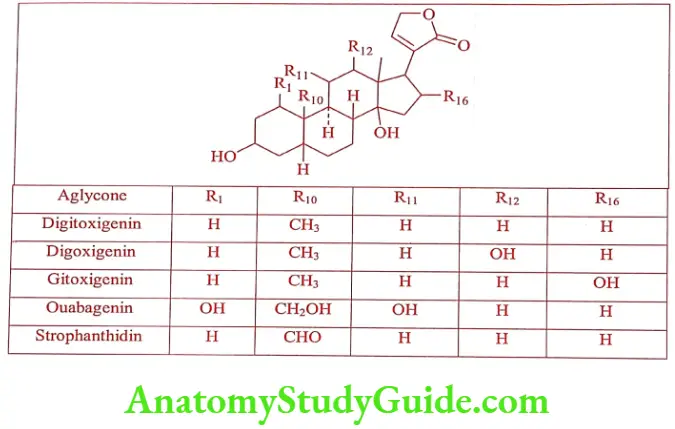
The cardiac glycosides from animal source (generally bufadienolides) have less medicinal importance because of their high toxicity. Pharmaceutical preparations of whole plants and partially hydrolyzed glycosides of Digitalis lanata and Digitalis purpurea have been widely used clinically.
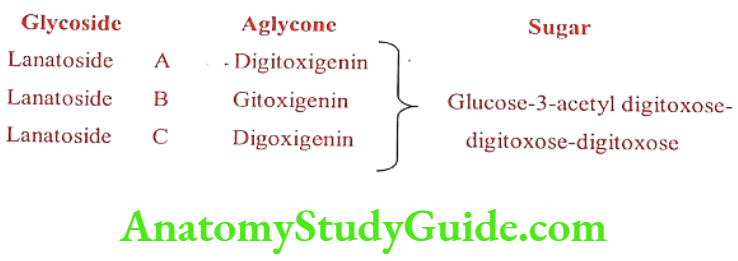
The glycoside present in Digitalis lanata and Digitalis purpurea are Lanatoside A, B and C. Composition of these glycoside are
Digoxin (Lanoxin)
Digoxin is a purified digitalis preparation from Digitalis lanata and represents the most widely used digitalis glycoside.
The structural components of various glycosides are given below:
Mechanism of Action
Congestive heart failure (CHF) is inability of the heart to pump blood effectively at the rate that meets the need of metabolizing tissues. This results in the reduced contractility which causes a decrease in cardiac output, increasing the blood volume of the heart. This in turn reduces the systemic blood pressure and renal blood flow, which leads to edema. Cardiac glycoside increases cardiac muscle contraction, reduces heart rate and decreases both edema and the heart size.
This causes a positive isotropic effect, which involves the ability to inhibit the membrane bound Na+/K+ adenosine triphosphate (Na*/ K* ATP ase) pump responsible for sodium/potassium exchange. The process of membrane depolarization /repoliarization is controlled mainly by the movement of these three ions, Na+, K+, Cat in and out of the cell.
On contraction (resting state) the concentration of Na+ is high outside the cell. On membrane depolarization, Na* fluxes in, leading to an immediate elevation of the action potential. The influx of calcium results in efflux of potassium out of myocardium. The Na+/K+ exchange requires energy and is catalyzed by the enzyme Na+/K+-ATPase.
Cardiac glycoside inhibits this enzyme, which reduces sodium exchange with potassium, which in turn increases intracellular calcium. Elevated calcium ion triggers myocardial contraction or a positive isotropic effect.
Drug Interaction
Digoxin-drug interaction is the common cause for digitalis toxicity. The drugs Quinidine, Verapanil, Rifampin increase the Digitoxin blood level to toxic level. The oral absorption of Digitoxin is also altered by certain drugs. For example, laxatives and Cholestyramine will decrease the absorption.
ADR: Tachycardia, atrial fibrillation, visual disturbance and rarely thrombocytopenia.
Dose: 0.4 to 0.6mg, i.v as loading dose followed by 0.125 to 0.5 mg i.v daily
Uses: It is used to treat congestive heart failure patients who are in sinus rhythm.
Non-Glycosidic Agents or Phosphodiesterase-3-inhibitors
Cardiac contraction involves G-protein signals transduction pathways. Activation of G-protein involves the formation of intracellular cAMP which increases intracellular calcium and contraction of cardiac muscle. When the cAMP is hydrolysed by PDE3, relaxation occurs. So, inhibition of PDE3 promotes cardiac contraction and vascular smooth muscle dilation.
PDE3 inhibitors are used only for short term therapy, long term therapy increases mortality in heart failure patients. Mainly they are used in conjucation with other treatment modalities like diuretics, vasodilators or cardiac glycosides. The generic name of PDE3 ends with “one” and PDEs ends with “fil”. (Phosphodiesterase – 5 – inhibitors are vasodilators and used for male erectile dysfunction).
Milrinone (Primacor)
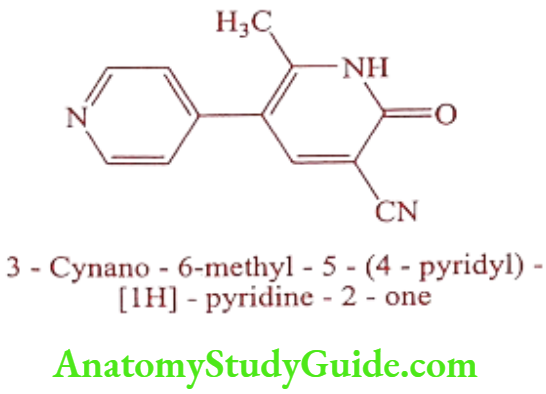
Milrinone is a phosphodiesterase-3-inhibitor that works to increase contractility in a failing heart. It is non-glycosidic ionotropic agent used for short-term intravenous treatment on the patients who have not responded to digitalis, diuretics and vasodilators. It is off-white to tan yellow crystalline compound soluble in methanol and slightly soluble in chloroform and water. It is available as sterile aqueous solutions of the lactate salt for intravenous infusion.
ADR: Allergic reaction, difficulty in breathing, swelling of face, lips, tongue or throat.
Dose: 50μg/kg as a loading dose should be administered slowly over 10mts.
Use: It is used for the short term treatment of heart failure.
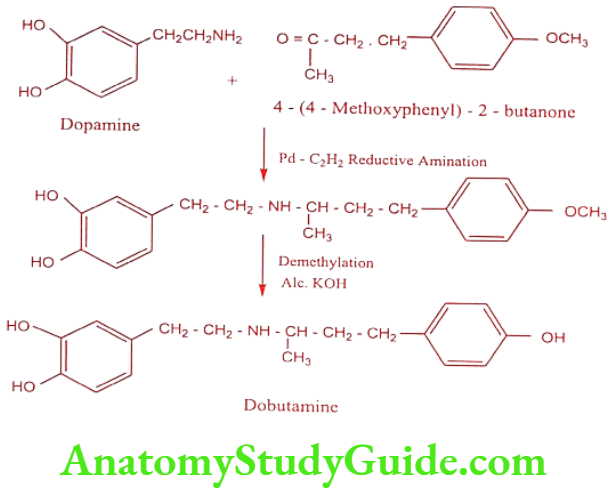
Dobutamine (Dobutrex)
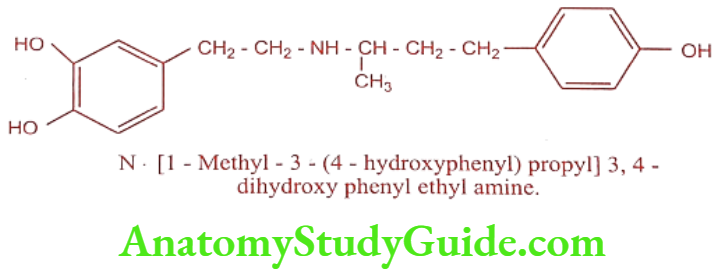
Dobutamine is an a and ẞ – adrenergic receptor agonist. It resembles Dopamine chemically, but possesses a bulky aromatic residue on the amino group despite the absence of a B-OH group. The (+) isomer has potent ẞ-agonist action. The (-) isomer has potent a1-agonist and poor ẞ-agonist actions.
Synthesis
ADR: Tachyarrhythmia, hypertension, eosinophilic myocarditis and angina.
Dose: 2.5 to 15μg/kg/mts.
Use: It is used for short term treatment of cardiac decomposition that may occur after cardiac surgery or in patients with congestive heart failure or myocardial infarction.
Drugs For The Treatment Of Angina Pectoris (Or) Antianginal Agents
Introduction
Angina pectoris (in Greek chock) is the chronic disease affecting the coronary arteries, which supply oxygenated blood from the left ventricle to all the heart tissues. When the lumen of the coronary arteries become restricted, it becomes less efficient in supplying blood and oxygen to the heart and the heart is said to be “ischemic” (oxygen deficient).
Angina is the primary symptom of severe pain originating in the chest, often radiating to the left shoulder and down the left arm. Therapy of angina is directed mainly towards alleviating and preventing anginas attack by altering the oxygen supply / oxygen demand ratio to the cardiac muscle or dilating the coronary vessels.
Clinical types of angina pectoris:
- Stable angina: It is characterized by episodes of chest pain commonly associated with exertion.
- Unstable angina: It is characterized by angina at rest with increased frequency and duration of angina attacks.
- Prinzmetal or Variant angina: Angina that occurs at rest and is due to spasm of the coronary arteries.
Antianginal agents may improve angina by reducing the demand or by increasing the supply of oxygen and dilates coronary arteries and decrease after load.
Classification
- Organic nitrates : eg. Nitroglycerin, Isosorbide mononitrate, Isosorbide dinitrate, Erythrityl tetranitrate, Pentaerythritol tetranitrate, Amyl nitrite.
- ẞ – adrenergic blockers : eg. Propranolol, Atenolol, Metoprolol.
- Calcium channel blockers:
-
- 1,4 – Dihydro pyridines : eg. Nifedipine, Nimodipine, Amlodipine, Nisoldipine, Felodipine, Nicardipine, Benidipine, Lacidipine.
- Phenyl alkyl amines : eg. Verapamil
- Benzothiazepines : eg. Diltiazem.
- Diamino propanol ether : eg. Bepridil.
- Potassium channel opener : eg. Nicorandil
- Miscellaneous : eg. Dipyridamole, Trimetazidine
Organic Nitrates
Organic nitrates are esters of simple organic alcohols or polyols with nitric acid. Amyl nitrite, Nitroglycerin, Isosorbide dinitrate, Erythrityl tetranitrate and Penta erythyritol tetranitrate are in clinical use. The chemical nature of these molecules as esters constitutes some problem in formulating these agents such as
- Volatility is an important concern in drug formulation because of the loss of the active principle from the dosage form.
- In addition, moisture should be avoided during storage to minimize the hydrolysis of the ester bond which lead to the decrease in the, therapeutic effectiveness.
- Due to its explosive property, these agents should be diluted with a variety of vehicles and excipients which eliminates this potential hazard.
Mechanism of Action
Myocardial ischemia occurs when the oxygen supply is insufficient to meet the myocardial oxygen demand. This occurs because of atherosclerotic narrowing of the coronary circulation or vasospasm of the coronary artery. The vasodilating effect of organic nitrates on the vein leads to pooling of the blood in the vein and decreased venous return to the heart (decreased preload) whereas vasodilatation of the coronary arterioles decreases the resistance of the peripheral tissues (decreased after load).
The decrease in both preload and after load results in generalized decrease in the myocardial work load. Organic nitrates restore the balance between oxygen supply by venous dilatation and oxygen demand by decreasing the myocardial work load.
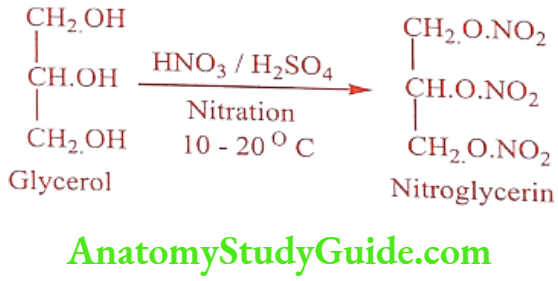
Nitroglycerin or Glyceryl trinitrate (Myovin, Nglong, Angised)
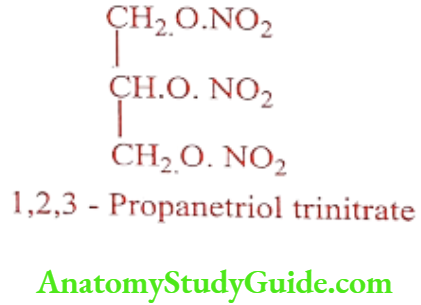
Synthesis
ADR: Facial flushing, dizziness, tachycardia, throbbing headache and tolerance.
Dose: 300 to 600μg.
Use: It is used extensively as an explosive in dynamite. It has a strong vasodilating action.
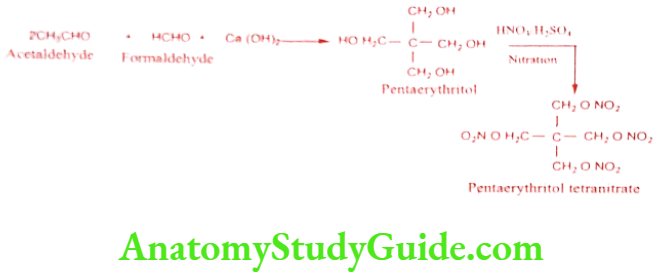
Pentaerythritol tetranitrate (Cardilate)
Synthesis
ADR: Facial flushing, dizziness, tachycardia, throbbing headache and tolerance.
Dose: 40 to 240mg daily in divided dose before meal.
Use: It is used prophylactically to reduce the severity and frequency of angina pectoris. It relaxes the smooth muscle of smaller vessels in the coronary vascular tree.
Isosorbide mononitrate (Imdur, Ismo, Monit, Monotrate, Solotrate)
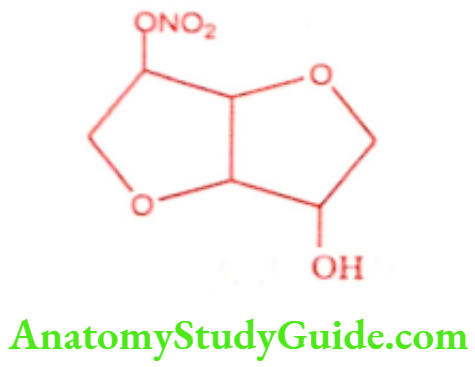
ADR: Hypotension, tachycardia, flushing, headache and dizziness.
Dose: Usual dose is 20mg, 2 to 3 times daily. The dose may be increased to 120mg daily if necessary.
Use: It is used principally in the treatment of angina pectoris.
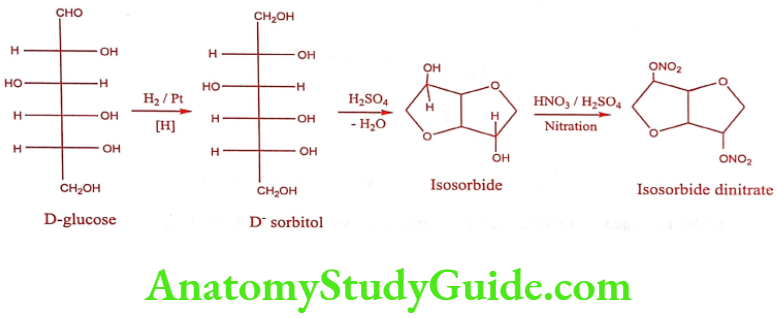
Isosorbide dinitrate (Sorbitrate, Isordil)
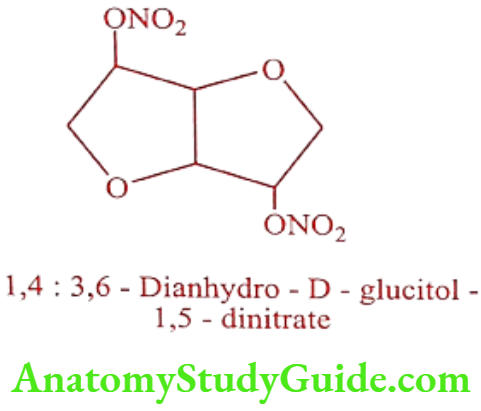
Synthesis
ADR: Hypotension, tachycardia, flushing and headache.
Dose: 20 to 120mg daily in divided doses.
Use: It is effective in the treatment of acute angina attack.
Calcium Channel Blockers
The second major therapeutic approach to the treatment of angina is the use of calcium channel blockers.
Potassium Channel Opener
Potassium channel openers are drugs that activate ATP sensitive potassium channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage sensitive calcium channels and decreases intracellular calcium levels. With available less calcium to combine with calmodulin, there is less activation of myosin light chain kinase (MLCK) and phosphorylation of myosin light chains. This leads to relaxation and vasodilation.
Being effective arterial dilators, potassium channel openers are used in the treatment of hypertension. These drugs are not first line therapy for hypertension because of their side effects and therefore they are demoted to treat severe hypertension. They are generally used in conjunction with a ẞ blocker and diuretic to attenuate the reflex tachycardia and retention of sodium and fluid, respectively.
Nicorandil (Ikorel, Dancor, Korandil, Nikoran)
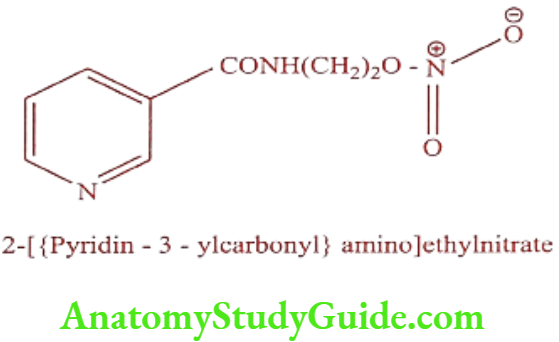
ADR: Headache, flushing, dizziness, mouth ulcer, nausea and vomiting.
Dose: 10mg bid, increase if necessary.
Use: It is used to treat angina.
Miscellaneous
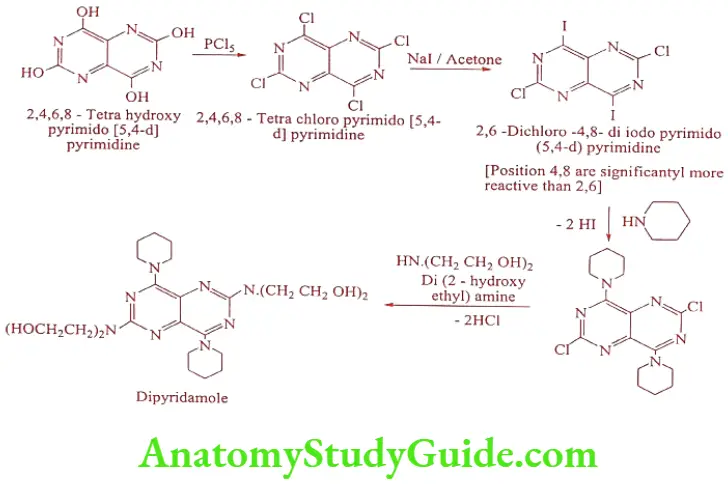
Dipyridamole (Cardiwell, Persantin) na vasa
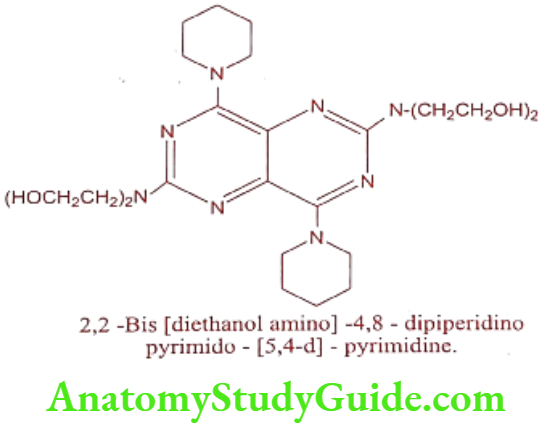
Dipyridamole is Phosphodiesterase inhibitor causes a long acting and selective coronary vasodilator by increasing coronary blood flow via selective dilation of the coronary arteries
Synthesis
The drug inhibits adenosine deaminase in erythrocytes and interferes with the uptake of vasodilator adenosine by erythrocytes. These actions potentiate the effect of prostacyclin which acts as an inhibitor to platelet aggregation.
ADR: GI disturbances, headache, dizziness, faintness and facial flushing.
Dose: 300 to 600mg/day in divided doses.
Use: It is a long acting vasodilator. Its vasodilating effect is selective for the coronary system. It is used to treat angina pectoris.
Trimetazidine (Vastarel MR, Cytogard, Carvidon)
ADR: GI disturbances, nausea and vomiting.
Dose: 40 to 60mg daily in divided doses.
Use: It is used as anti-ischaemic agent.
Drugs For The Treatment Of Cardiac Arrhythmiasis (or) Antiarrhythmic Drugs Introduction
Cardiac arrhythmias are the disturbance of normal rhythm of the heart may be due to alterations in impulse generation or disturbances in impulse conduction or a combination of both these factors.
Certain tissues in the heart concerned with initiation (impulse generation) and propagation (impulse conduction) of the heart beat called pacemaker tissues. They include SA (sinu atrial) node, AV (atrio ventricular) node, bundle of HIS, right and left bundle branches and Purkinje fibers.
Normally cardiac excitation (action potential) begins in the SA node located in the right atrial wall just below the opening of the superior venacava. Its fibers can generate and discharge impulses more rapidly than any other pacemaker tissues and their rate of discharge determines the rate at which the heart beats, that is why SA node is called as “cardiac pacemaker”.
Later the impulses travel from SA node to AV node through internodel fibers. From AV node impulses pass into bundle of HIS and through right and left bundle branches it reaches the large diameter of myofibers (Purkinje fibers) which rapidly conduct the impulse into mass of ventricular muscle tissues.
Arrhythmiasis Classification
Antiarrhythmic drugs are classified on the basis of mechanism of action into the following distinct classes
- Class I: Membrane stabilizing agents (Sodium channel blockers) :eg. Quinidine, Procainamide, Disopyramide,Lidocaine, Phenytoin, Mexiletine, Tocainide.
- Class 2: ẞ – adrenergic blockers : eg. Propranolol, Acebutalol. Esmolol, Atenolol, Timolol, Metoprolol, Sotalol.
- Class 3: Repolarization prolongators : eg. Amiodarone, Bretylium, Dofetilide, Ibutilide.
- Class 4: Calcium channel blockers : eg. Verapamil, Diltiazem.
Membrane stabilizing agents
Class I antiarrhythmic agents are drugs that have membrane stabilizing properties (ie. they shift membrane to more negative potential). Drugs in this class act in Na+ channel and interfere with the process by which the depolarization charge is transferred across the membrane. It is assumed that these drug bind to the Na+ channel and block its function, presenting Na* conductance as long as the drug is bound.
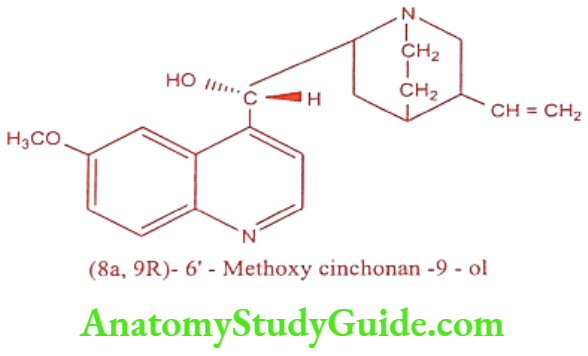
Quinidine (Natcardine, Quinidine)
Quinidine is an alkaloid isolated from Cinchona bark. It is a dextro rotatory diastereo isomer of Quinine. Structurally, Quinidine is composed of a quinoline ring and a bicyclic quinuclidine ring system, with a hydroxymethylene bridge connecting these two components.
Quinidine is basic in nature so it is always used as water soluble salt form such as sulfate, gluconate and polygalactouronate.
ADR: Muscle weakness, nausea, vomiting, diarrhea, cinchonism symptoms including impaired hearing, head ache, blurred vision, dizziness and vomiting, urticaria and skin reactions.
Dose: 200mg every 2 to 3 hrs for 5 to 8 doses.
Use: It is used to treat supraventricular and ventricular ectopic arrhythmias such as atrial and ventricular tachycardia, atrial flutter and atrial fibrillation.
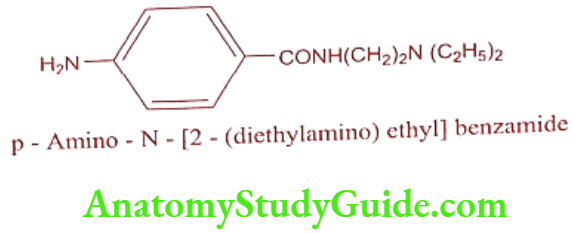
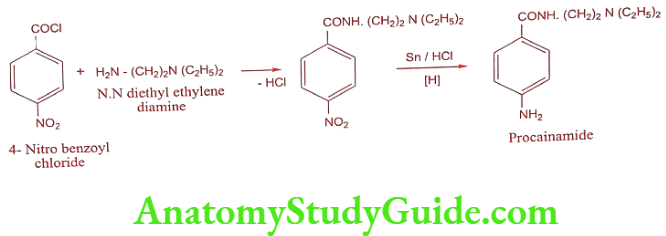
Procainamide (Pronestyl)
Synthesis
ADR: Severe hypotension, ventricular fibrillation, heart failure, agranulocytosis after prolonged treatment and psychosis.
Dose: 500 to 1000mg every 4 to 8 hrs, 500 to 600mg as slow infusion over 25 to 30mts.
Use: It is used in the treatment of ventricular arrhythmias.
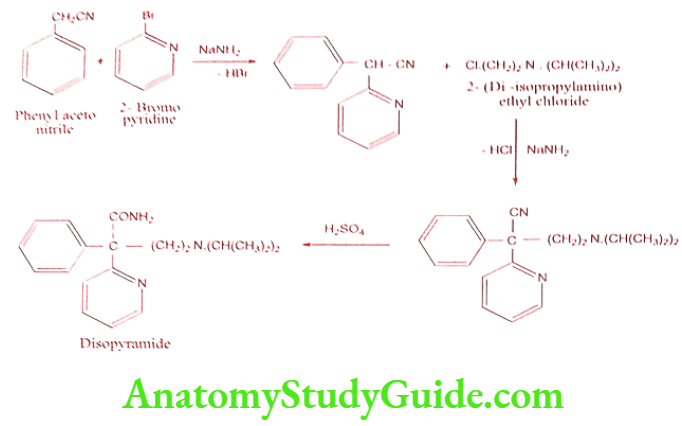
Disopyramide (Norpace, Regubeat)
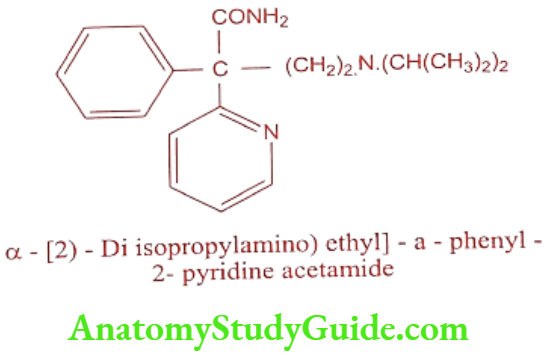
It is available as phosphate salt. It is administered as a racemic mixture, but its antiarrhythmic activities resides on S – enantiomer.
Synthesis
ADR: Adverse effects are primarily anticholinergic in nature includes impotence, constipation, and difficulty in micturition, dry mouth, blurred vision, nausea, bloating and abdominal pain.
Dose: 300 to 800mg daily in divided doses.
Use: It used in the treatment of refractory, life threatening ventricular tachyarrhythmias.
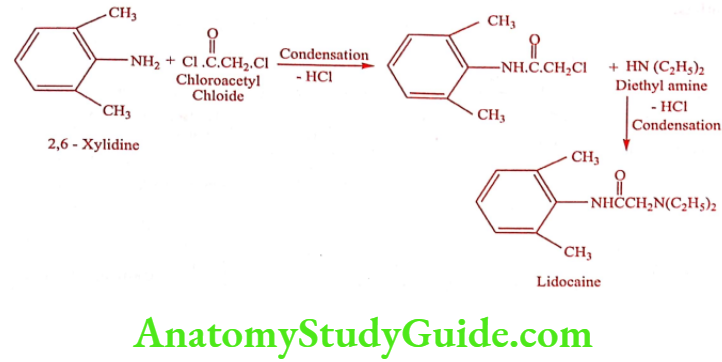
Lidocaine or Xylocaine or Lignocaine (Lignocip, Loxicard)
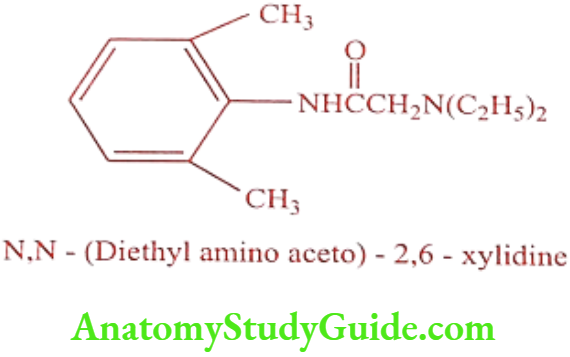
Lidocaine blocks sodium channel and shorten the action potential duration and reduce refractory period. Lidocaine is effective only when given parenterally. It’s orally inactive because of rapid first pass metabolism by the liver.
Synthesis
ADR: Dizziness, paraesthesia, drowsiness, confusion, respiratory depression and convulsions.
Dose: 1 to 1.5mg/kg, repeat if necessary.
Use: It is used only in ventricular tachyarrhythmias. It is also a potent local anesthetic agent.
Tocainide (Tonocard)
ADR: Gastrointestinal disturbance and CNS effects.
Dose: 400 to 600mg every eight hrs.
Use: It is used in the treatment of ventricular arrhythmias.
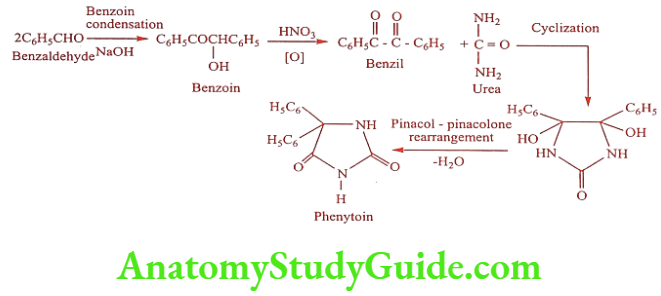
Phenytoin (Dilantin, Epsolin)
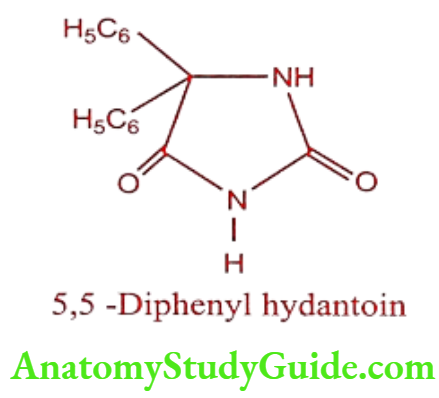
Phenytoin sodium is a hygroscopic solid which is slowly decomposed by atmospheric carbon dioxide into Phenytoin and sodium carbonate. It forms characteristics copper complex when treated with copper sulphate in pyridine solution.
Its cardiac electrophysiological actions are very similar to those of Lignocaine. The most prominent effect is depression of automaticity in ventricular and Purkinje fibres without affecting that in SA node.
Synthesis
ADR: Hypersensitivity, lack of appetite, head ache and dizziness.
Dose: Oral 100 to 200mg and i.v 100mg for every 10mts and maximum of 600mg.
Use: It is a narrow spectrum antiarrhythmic for ventricular arrhythmias, especially when induced by digitalis. It is useful against all types of seizures.
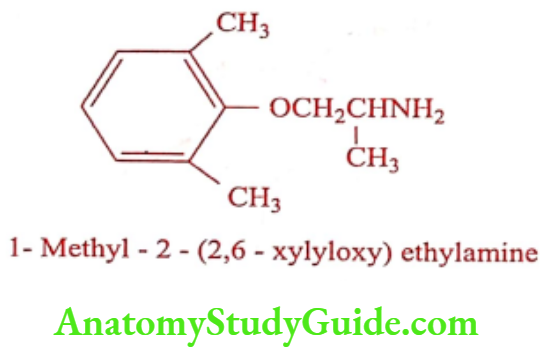
Mexiletine (Mexitil)
ADR: Oesophageal ulceration, confusion, blurred vision, sleep disturbances and speech difficulties.
Dose: 400mg as loading dose followed by 200 to 250mg after two hrs 3 to 4 times daily.
Use: It is a Class – IB antiarrhythmic agent. It is used for long term oral prophylaxis of ventricular tachycardia.
Adrenergic Blocking Agents
Sotalol (Betapace, Sotacor)
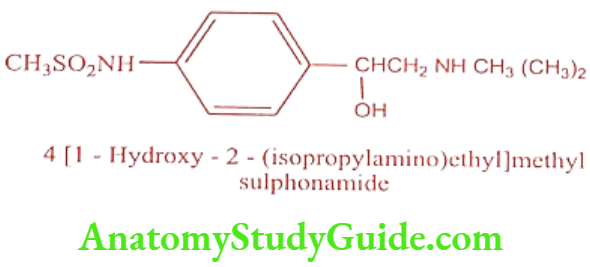
(+) Sotalol is a non-selective ẞ – adrenergic receptor antagonist. It contains chiral centre and marketed as racemic mixture. I enantiomer is more potent ẞ – adrenergic receptor antagonist than the d enantiomer but the two are equi potent as K+ channel blockers. It is a Class III antiarrhythmic drug and differs from other Class III agent because of its ẞ-adrenergic receptor blocking action.
ADR: Vertigo, paralysis, thrombocytopenia, eosinophilia and pulmonary edema.
Dose: Initial dose is 80mg twice daily and it can be increased to 240 or 320mg/day.
Use: It is used to treat life threatening sustained ventricular tachycardia, atrial fibrillation of flutter.
Repolarization Prolongators
Member of this class prolong ventricular repolarization and increases the effective refractory period.
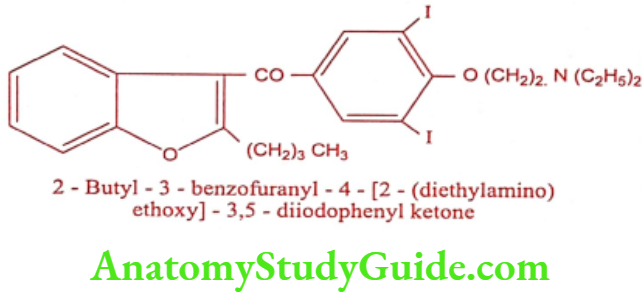
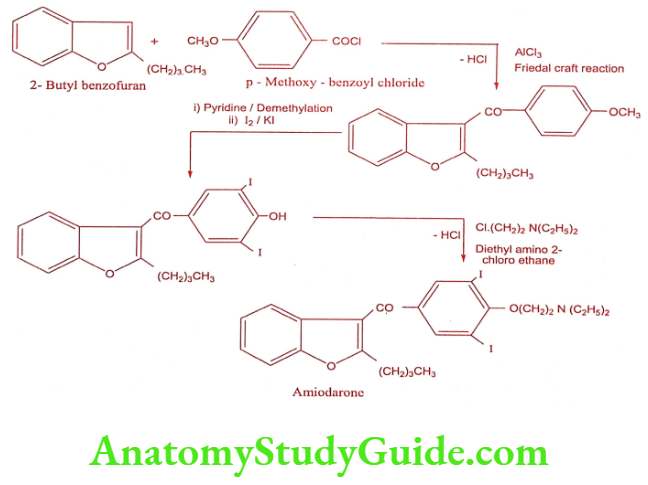
Amiodarone (Cordarone, Duran)
Amiodarone has a broad spectrum of activity and effective blockers of both Na and K+ channels.
Synthesis
ADR: Blue-grey discoloration of skin, photosensitivity, peripheral neuropathy, paraesthesia, myopathy, atoxia and metallic taste.
Dose: 800 to 1600mg/day as loading dose followed by 100 to 400mg daily.
Use: It is effective in maintaining sinus rhythm in patient who has direct current shock for atrial fibrillation. It is an antianginal agent.
Leave a Reply