Tubular Reabsorption And Secretion
Reabsorption is the process by which the solute and water is absorbed from renal tubule into peritubular capillaries. Essential substance like glucose, amino acids, electrolytes are reabsorbed from renal tubule.
Table of Contents
Secretion is the process in which the solute and water is secreted from peritubular capillaries into renal tubule. This process is opposite of reabsorption. Various waste products and toxic drugs are secreted into renal tubule.
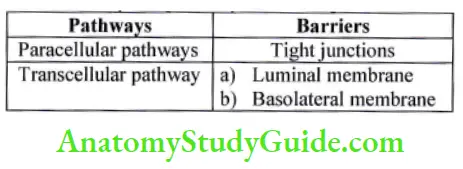
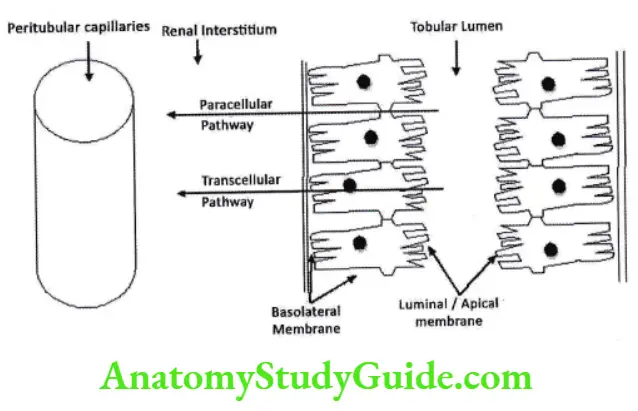
Pathways of reabsorption and secretion
There are two pathways of reabsorption and secretion paracellular and Transcellular. In paracellular pathway solute pass from tight junction between two adjacent cells while in Transcellular pathway the solute has to cross luminal membrane and basolateral membrane.
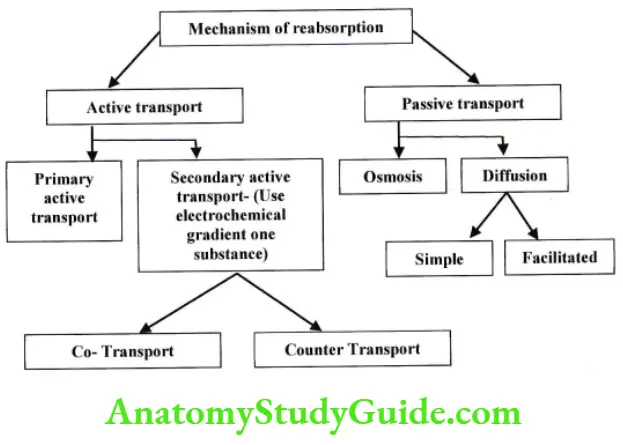
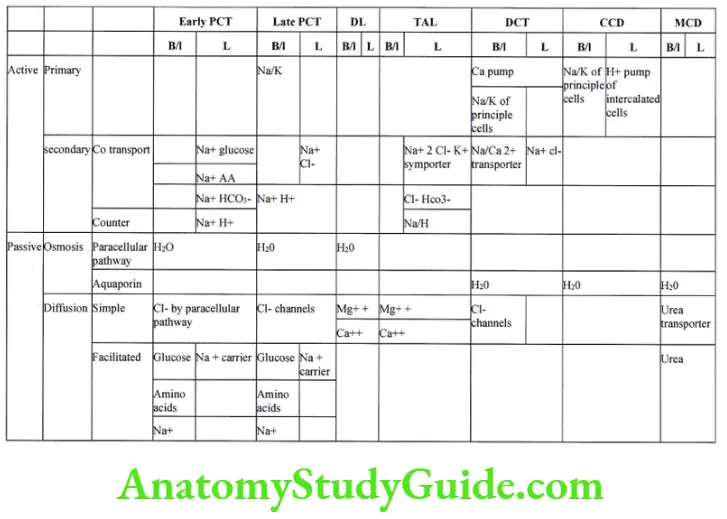
Reabsorption takes place by 2 basic mechanisms – active and passive transport:
- Active transport – energy is required to transport substance against concentration gradient (uphill).
- Primary active transport – energy is utilized in form of ATP e.g. Na+ K+ pump.
- Secondary active transport – energy is utilized in form of electrochemical gradient of one substance to transport other substance.
- Co transport – when both substance moves in same direction. E.g. Na+ Glucose.
- Counter transport – when two substance moves in opposite direction E.g. Na+ H+.
- Passive transport – energy is not required, transport occurs along concentration gradient (downhill).
- Osmosis- when solvent moves along concentration gradient
- Diffusion- when solute moves along concentration gradient
- Simple – transport of solute without the aid of transmembrane integral proteins.
- Facilitated – transport of solute with the aid of transmembrane integral Proteins.
Transport maximus (TMAX):
- Amount of plasma filtered is known as filtration load or tubular load’
- Filtration load or tubular load = GFR X Plasma concentration of substance.
- Essential filtered substance is reabsorbed by active and passive mechanism’ Each transport system has a maximum capacity to transport substance which is known is (Tmax) transport maximus. It is due to saturation of specific transport system. Tmax depends on.
- Carrier Proteins
- Specific enzymes
- Affinity to substance
- When the filtration load is greater than maximum reabsorption rate (T Max) then substance starts to appear in urine.
Consider example of glucose absorption in PCT
- Tmax for glucose (TmG) is 375mglmin
- Normal plasma Glucose concentration is 1 mg/ml and GFR is 125 ml/min.
- So filtration load of glucose is 1 mg/ml X 125 ml/min = 125 mg/min.
- When plasma Glucose concentration exceeds 2 mg/ml, filtration load becomes (2mg/ml X 125 ml/min) 250mg/min.
- At this point glucose start to appear in urine, which is known as renal threshold for glucose.
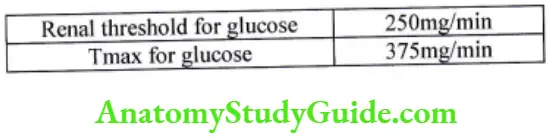
Difference in Renal threshold for glucose and Tmax for glucose is because all nephron does not have same Tmax. Tmax for some nephron starts at 250mg/min, while at 375 mg/min all nephron have reached their Tmax.
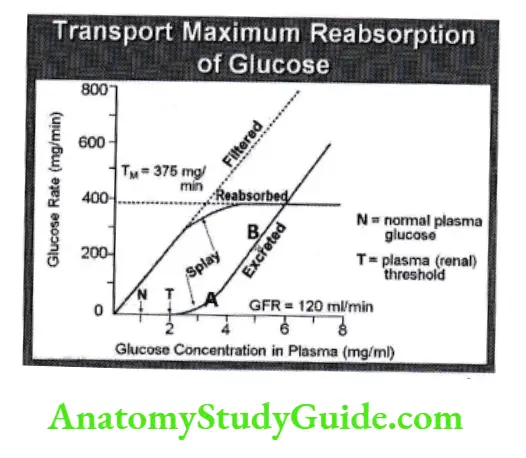
Splay: – It is small triangular region on glucose curve between renal threshold and TmG. it represents the concentration difference between a maximum renal reabsorption and its appearance in the urine. It is cause due to heterogeneity in glomerular size variability in TmG of different nephron.
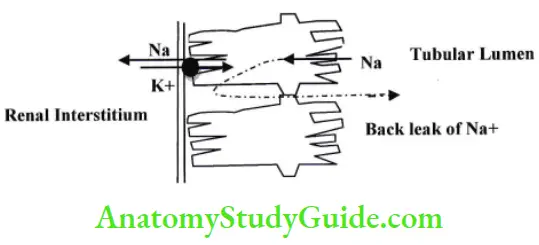
Exception to Tmax is Na+ K+ pump in early PCT’ It does not follow Tmax.
- As T max of Na+ K+ pump is greater than actual rate of Na+ reabsorption.
- Significant amount of Na+ back leak in tubular lumen, so not enough Na+ is available for Na+ K+ pump. Back leak depends on.
- Permeability of tight junctions.
- Starling forces in interstitium.
Na+ K+ pump follows gradient time transports which depends on.
- Electrochemical gradient.
- Time for which substance remains in tubules.
- Selective Permeability for substance.
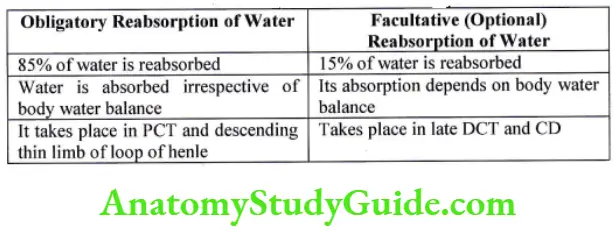
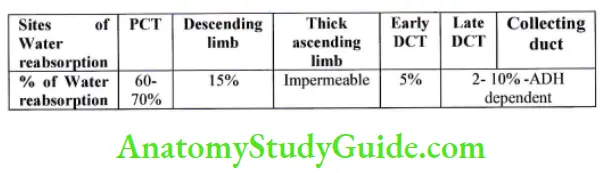
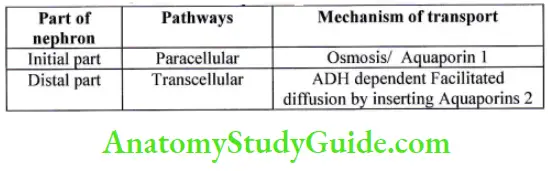
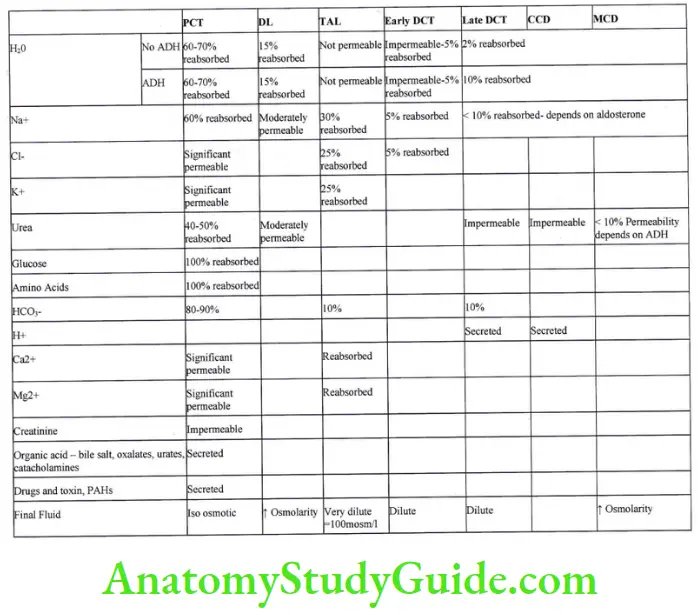
Reabsorption of Water
Regulation of sodium and water reabsorption
It is regulated by
- Glomerulo tubular feedback
- Starling forces between peritubular capillaries and renal interstitial
- Pressure natriuresis and diueresis
- Hormonal
- Aldosterone
- Angiotensin 2
- Atrial natriuretic Peptide
- Sympathetic system
Glomerulo tubular feedback
It is fundamental capacity of kidney to increase absorption rate in response to increased filtration rate. It prevents overloading of DCT. It is second line of defense to buffer effect of spontaneous changes in GFR on urinary output. Distal segments of the nephron have a very low capability to increase tubular reabsorption of water and solutes; therefore, a large increase in distal flow rates would result in loss of filtrate in the urine.
Glomerulotubular balance is operated in PCT which reabsorb around 67vo of the filtered load of solutes and water at any rate of GFR. Probable explanation for this phenomenon could be, the alteration in GFR produce change in the starling forces of the peritubular capillaries leading to proportionally increased or decreased total reabsorption.
Starling forces between peritubular capillaries and renal interstitial
Reabsorption = KfX net reabsorption pressure.
Kf is reabsorption coefficient that depends on surface area and hydraulic conductivity.
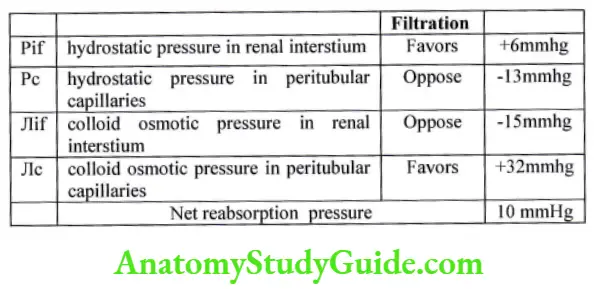
Hydrostatic pressure in peritubular capillaries (Pc):
It depends on
- If Arterial pressure increases, hydrostatic pressure in peritubular capillaries also increases, which inhibits reabsorption. This action is buffered by auto regulatory mechanism which maintains constant GFR.
- Increase in afferent and efferent arteriolar resistance will decrease the renal blood flow, decrease hydrostatic pressure in peritubular capillaries and thus will increase reabsorption rate.
Colloid osmotic pressure in peritubular capillaries (JIc):
It depends on
- Systemic plasma Colloid osmotic pressure.
- Filtration fraction – When filtration fraction increases, more water.is filtered. It leads to concentration of plasma proteins that increases Colloid osmotic pressure in capillaries. it increases reabsorption rate in peritubular capillaries.
Pressure natriuresis and diueresis
GFR is auto regulated between pressure 75-180mmhg. When blood pressure exceeds 160mmhg, then filtration of sodium and water increase knows as pressure natriuresis and diuresis.
Increase arterial Pressure,
- Increases capillary r:ydrostatic pressure will increase filtration rate and will decreases the reabsorption.
- More sodium at macula densa, will inhibit secretion of renin and so will decrease angiotensin 2, which will reduce Na+ and water reabsorption.
Hormonal control
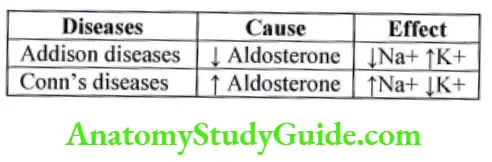
- Aldosterone
- It is secreted by zona glomerulosa of adrenal gland.
- It acts on principal cells of cortical collecting duct and late dct.
- It stimulates Na+k+ pump on basolateral membrane and it increase sodium permeability on luminal side. Thus it increases Na+ absorption.
Applied:-
- Angiotensin 2
- It is secreted by Juxta Glomerular apparatus in response to decrease sodium, decrease blood volume or decrease blood pressure.
- It increase aldosterone secretion which increase sodium absorptions.
- It increases efferent arteriolar resistance thus increases GFR, increases filtration fraction.
- It decreases peritubular capillary hydrostatic pressure and increases colloid osmotic pressure in peritubular capillaries thus increase reabsorption rate.
- Antidiuretic hormone – It increase water reabsorption in late DCT, and collecting duct.
- Atrial natriuretic peptide – It is secreted by atria in response to increased plasma volume. It inhibit absorption of Na+ and water.
Sympathetic system
It causes
- Afferent vasoconstriction: it decreases GFR, and increases Na+ and water reabsorption.
- It stimulate rennin Angiotensin aldosterone system which also increases Na+ and water reabsorption.
Leave a Reply