Gallstone Ileus – Gallstone Obturation
Gallstone ileus Introduction:
Table of Contents
Gallstone ileus is more common in women and accounts for 1–4% of all presentations to hospital with small bowel obstruction. The term gallstone ileus is a misnomer,
As the condition is a mechanical obstruction of the gut and not a true ileus.
- It should be suspected in a patient who has gallstones and presents with intestinal obstruction.
- Elderly females above the age of 60 are usually affected.
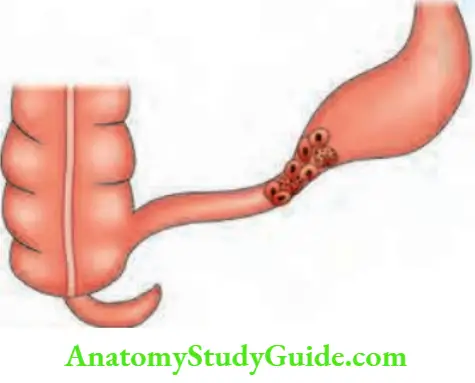
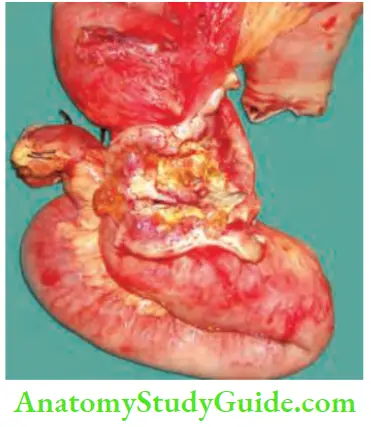
- Gallstone reaches the terminal ileum by forming ‘cholecystoduodenal fistula’ due to recurrent attacks of cholecystitis.
- Due to recurrent inflammation, adhesions develop between gallbladder and duodenum (common) or gallbladder and colon or stomach (rare). Large stones cause pressure necrosis, resulting in formation of a cholecystoduodenal fistula.
- Terminal ileum is the narrowest portion of the gut wherein gallstone gets impacted. Sometimes, the stone may ulcerate from gallbladder into jejunum, colon, etc


Gallstone ileus Clinical features
- They are suggestive of small intestinal obstruction—abdominal pain is severe, vomiting and distension.
- Step ladder peristalsis may be seen. History suggestive of recurrent cholecystitis may be present.
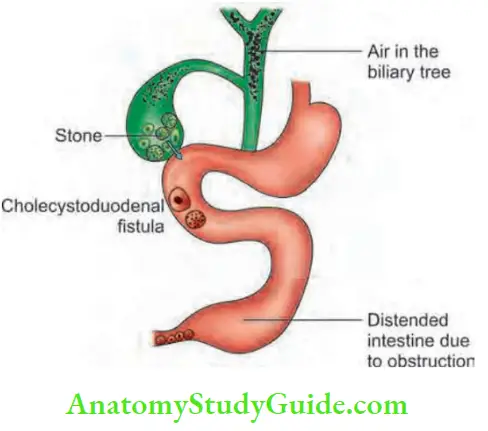
Rigler’s triad: Pneumobilia, the presence of an aberrant gallstone and enteric obstruction.
Bouveret syndrome: It is a gastric outlet syndrome secondary to stone lodged in proximal duodenum due to cholecystoduodenal fistula. Proximal migration of the stone will precipitate obstruction.
Gallstone ileus Investigations
1. Plain X-ray abdomen (erect position):
- May demonstrate multiple gas and fluid levels and stone in the gallbladder and also in the lower abdomen suggesting gallstone ileus.
- Air may be found1 in the biliary system.
2. Small bowel enema:
- May demonstrate partial obstruction.
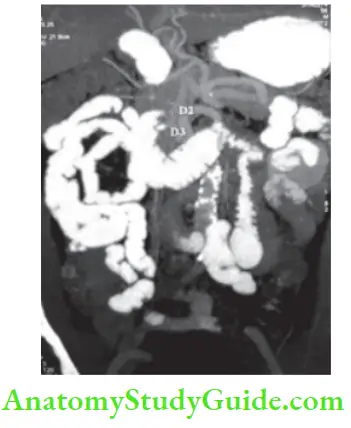
- Computed tomography (CT) scanning is the investigation of choice. It has a preoperative diagnosis of gallstone ileus with a sensitivity of 93%.
- It will also indicate any inflammation of the gallbladder, fistula—air pockets in the gallbladder, distal stone and proximal dilatation.
3. Computed tomography (CT):
- CT Scanning is the investigation of choice. It has a preoperative diagnosis of gallstone ileus with a sensitivity of 93%.
- It will also indicate any inflammation of the gallbladder, fistula—air pockets in the gallbladder, distal stone and proximal dilatation.
Gallstone ileus Treatment
- There is difference of opinion regarding what is the ideal surgery to be done in case of gallstone obstruction. It is because many patients are elderly, with co-morbidity and they have intestinal obstruction (dehydration, bowel oedema, bacterial proliferation, etc).
- Whatever it is, the first step is always to do enterolithotomy by incising the ileum and delivering the stone/stones.
- It may be possible to crush the stone and pass it onto caecum, avoiding enterolithotomy. Search the proximal intestine for any other stones.
What must be done next? Two types are described.
- Single stage procedure: If general condition of the patient is good, and gallbladder is gangrenous or inflamed (more chances of perforation), enterolithotomy, cholecystectomy followed by closure of the duodenal fistula is done.
- Two-stage procedure: If general condition is not good or with no active inflammation of the gallbladder, enterolithotomy is the procedure of choice, followed 6 weeks later by cholecystectomy with closure of the duodenal fistula

Mesenteric Vascular Occlusion Definition
Acute mesenteric ischaemia is an abrupt reduction in blood flow to the intestinal circulation of sufficient magnitude to compromise the metabolic requirements and potentially threaten the viability of the affected organs
Anatomy of Mesenteric Vasculature
- The mesenteric arterial and venous circulation of the abdominal viscera form an extensive vascular network.
- There are a large number of collateral pathways that protect against ischaemic changes.
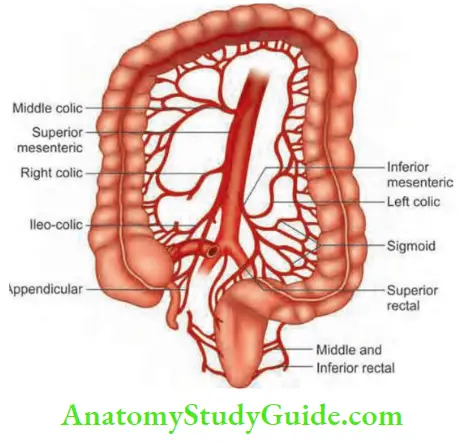
- The three major branches of aorta responsible for the arterial supply of the intestine are: Coeliac artery supplies the foregut, superior mesenteric artery (SMA) supplies midgut and inferior mesenteric artery supplies hindgut. The venous drainage includes the superior and inferior mesenteric vein.
Normal Anatomy and Variations
- Coeliac axis: Normal coeliac axis anatomy is seen in only 55% of patients. An anomalous right or left hepatic artery has been reported in about 50% of patients.
- Superior mesenteric artery: It supplies the entiresmall intestines and right one-third of the transverse colon.
- Inferior mesenteric artery (IMA): It supplies the left colon including rectum and surgical anal canal. The
- IMA arises at the level of the third lumbar vertebra supplies the large bowel from the mid-transverse colon to upper rectum. Several collateral networks exist in the branches of These collaterals are important when rectosigmoid or splenic flexure resection is performed;
- Collaterals: Like collaterals in the leg, many collaterals exist between 3 major branches—coeliac artery, SMA and IM Because of these extensive collaterals, patients remain asymptomatic with normal bowel function may have chronic occlusion of one or
two mesenteric vessels.
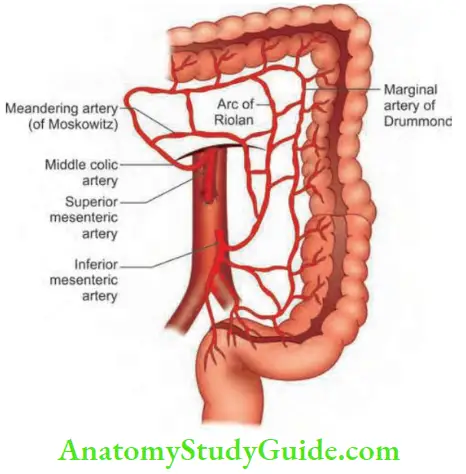
Griffiths’ point: Between branches of left colic and SMA.
Sudeck point: Sigmoidal arteries and superior rectal vessels.
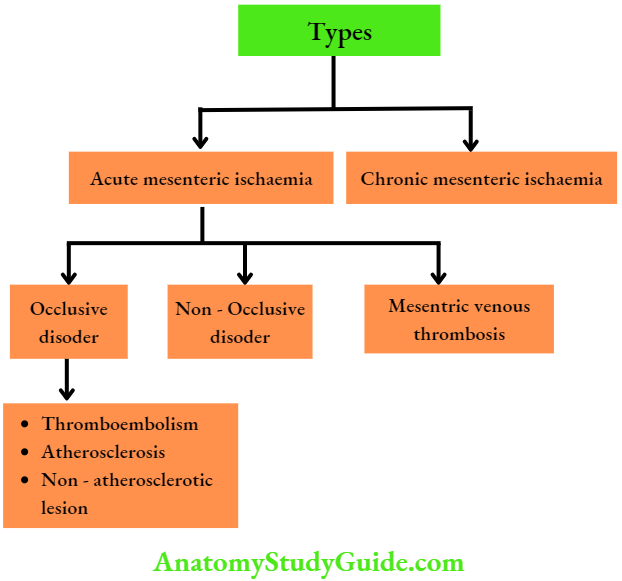
Mesenteric Vascular Occusion Types
- Acute mesenteric ischaemia (AMI): It is a sudden occlusion of an artery or vein resulting in gangrene. It has a mortality rate of 60 to 90%.
- Chronic mesenteric ischaemia (CMI): It is associated with stenosis of the coeliac artery, superior mesenteric artery or inferior mesenteric artery.
- NOMI: Non-occlusive mesenteric ischaemia
Mesenteric Vascular Occlusion Pathogenesis
- Ischaemic damage to the intestine occurs with decreased blood supply to a level at which delivery of oxygen and various nutrients cannot maintain oxidative metabolism. ‘
- Cell integrity is lost resulting in cell death. In low-flow states, blood is shunted from arterioles to venules near the base of the villus resulting in necrosis of the intestinal villi.
Non – Occlusive Mesenteric Ischaemia(NOMI)
It is a discrete clinical entity where mesenteric flow is impeded due to arterial spasm.
NOMI Causes
- Typically these patients are critically ill in intensive care units (ICU), intubated. The pathology resides in
- The mesenteric arcades where severe spasms have limited flow. Like AMI, they can have loose and bloody stools, and abdominal pain out of proportion to signs. Tenderness is present.
- Diagnostic arteriography is the only way to demonstrate the small vessel mesenteric arterial spasm that
leads to NOMI.
NOMI Treatment
Direct catheter delivery of papaverine (30–60 mg/hour) may have to be given for a few days.
- Systemic anticoagulants are given. Vessel spasms can be overcome by maximizing cardiac output.
- Peritonitis or clinical evidence of bowel perforation mandates exploration and resection of the ischaemic segment. Also, the primary cause of acute illness is treated.
NOMI Etiology
- Pharmacotherapy
- Digoxin stress response
- Digitalis
- Cocaine
- Alpha agonists
- Vasopressin
Sympathetically mediated
- Hypovolaemia or haemorrhagic shock
- Haemodialysis
- Cardiopulmonary bypass
- CCF
- Arrhythmias
- Pancreatitis
- Septic shock
- End-stage renal disease
Hirschsprungs Disease Congenital Megacolon
Hirschsprung’s disease: Hirschsprung’s disease is also called congenital megacolon, aganglionic megacolon or primary megacolon. It is one of the common causes of neonatal intestinal obstruction.
Hirschsprung’s disease Pathophysiology
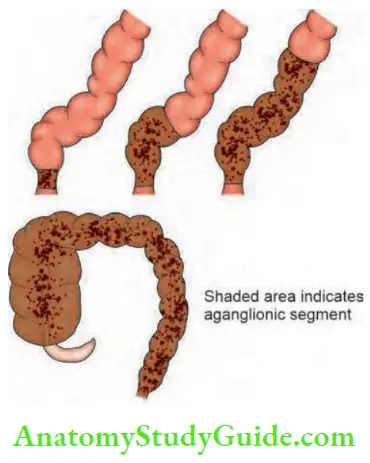
- The disease always involves the anus and rectum wherein parasympathetic ganglion cells are absent in the neural plexus of the intestinal wall. The defect involves internal sphincter.
- As a result of this, there is a terminally constricted, non-relaxing segment, in the rectum and sigmoid (lower part), above which the pelvic colon (sigmoid) is enormously dilated. Rectosigmoid area is involved in 80% of cases.
- Circular muscle hypertrophy, mucosal hyperaemia and ulcers are present in the dilated segments.
- In between, there may be a transition zone (cone), which contains a few parasympathetic ganglion cells.
- Rarely, Hirschsprung’s can also involve the entire sigmoid colon or even the entire colon.
- Hirschsprung’s rarely occurs in adults also.

Hirschsprung’s Disease Types
- Ultrashort segment: Anal canal and terminal rectum are aganglionic.
- Short segment: Anal canal and entire rectum is completely involved.
- Long segment: Anal canal, rectum and part of colon involved.
- Total colonic: Anal canal, rectum and the whole length of the colon is involved.
Hirschsprung’s Disease Clinical Features:
Male children are commonly affected when compared to females.
Incidence: 1 in 4000 to 5000 live births.
- The child presents with acute neonatal intestinal obstruction as manifested by failure to pass meconium or delay in passing meconium with abdominal distension.
- Within 12–24 hours, all features of intestinal obstruction can be found. If it is complicated by enterocolitis, it may result in perforation and septicaemia.
- A severe diarrhoea with blood and mucus, abdominal distension and vomiting can occur within a few hours, followed by hypovolaemic shock.
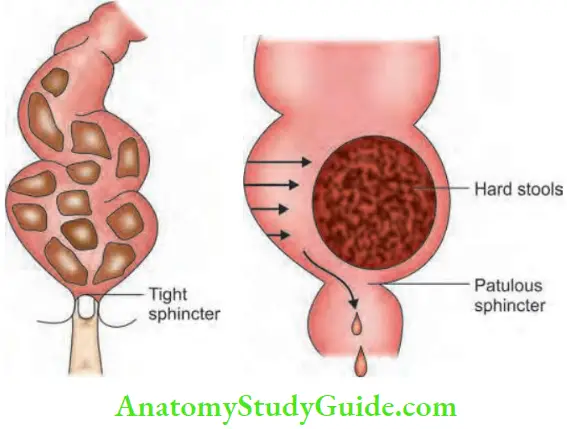
- Rectal examination reveals that the rectum is empty, finger is gripped by anal sphincter and there is no perianal soiling. On the other hand, in acquired megacolon, the rectum is loaded with faecal matter, perianal soiling is present and there is no sphincter activity
- Chronic variety: Chronic constipation manifests in the first few weeks of life. The child may be brought with abdominal distension. Stools are goat pellet-like
Hirschsprung’s Disease Differential Diagnosis
Acquired megacolon: Usually manifests by one to two years of age. The rectum is loaded with faecal matter.
Differential Diagnosis:
- Hypothyroidism
- Meconium plug syndrome
- Intestinal pseudo-obstruction
- Colonic neuronal dysplasia
Hirschsprung’s disease Complications
- Intestinal obstruction, perforation, peritonitis
- Enterocolitis
- Growth retardation
Hirschsprung’s disease Investigations:
- Full-thickness rectal wall biopsy: Under GA there is an absence of parasympathetic ganglion cells and hypertrophic nerve fibres in the nerve plexus. It should be taken above the anorectal junction. Today submucosal suction biopsy is more popular than biopsy since it avoids haemorrhage, infection and scarring.
- Barium enema: 3.6% solution of barium is used, the intermediate zone appears as a cone with proximal dilatation and a distal narrow zone which is characteristic of Hirschsprung’s disease.
Hirschsprung’s disease Treatment
- Emergency Cases:
- Right transverse loop colostomy: In most of cases, the aganglionic segment is limited to the rectosigmoid region.
- A full thickness biopsy of the colostomy is sent for histopathological examination.
- Definitive Surgery:
- Can be done usually between the age of 3 and 6 months (8 to 10 kg of weight).
- Resection of aganglionic bowel (anorectum) followed by a pull-through procedure. Maintaining continence is the main aim.
- A few points of comparison between ‘Duhamel’s and Swenson’s pull-through’ are mentioned below.
Duhamel’s:
- Retrorectal pull- Through
- Technically easy
Swenson’s:
- Endorectal pull – Through
- Difficult
Steps of Duhamel’s Pull-through Surgery
- The rectum is transected above the peritoneal fold and is closed.
- The proximal ganglionic segment is pulled down behind the rectum (retrorectal space created by using blunt dissector).
- An incision is made in the posterior wall of the anorectal above the dentate line and is deepened through the entire bowel wall.
- The end of the proximal colon is sutured to the opening in the posterior anal canal all around.
- The adjacent walls of the rectum (posterior wall) and colon (anterior wall) are crushed by using a Kocher’s forcep which falls off by itself by the 14th day.
- The open end of the rectum (above) is closed end to side to the colon.
- Other types of surgery: Soave’s mucosectomy and pull-through operation.
Pseudointestinal Obstruction
Acute colonic pseudo-obstruction (ACPO) is also called Ogilvie’s syndrome. It is massive colonic distension in the absence of a mechanically obstructing lesion.
Pseudo-obstruction Pathogenesis
- It occurs mainly due to malfunctioning of sacral parasympathetic nerves (S2–S4). It results in atony of the descending colon resulting in functional obstruction.
- It is interesting to note that the junction of the dilated and collapsed bowel is near the splenic flexure.
- This is the place wherein parasympathetic supply by the vagus ends and sacral autonomic nervous system starts. An increased sympathetic tone results in colonic dilatation due to inhibition of contraction.
Pseudo-obstruction Clinical Features
- Elderly bedridden patients with cardiac/lower respiratory illness are the victims.
- Aerophagia and drugs which decrease colonic mobility are precipitating factors.
- Failure to pass faeces and flatus for several days.
- Tachypnoea due to elevation of the diaphragm due to distended colon is common.
- Rectal examination reveals some faeces (in cases of mechanical obstruction, the rectum is empty).
- Plain X-ray abdomen erect may or may not show one or two air fluid levels. Distension is mainly colonic.
- Carcinoma colon is to be differentiated by barium enema.
- Caecal perforation is a dangerous complication.
- Hence, look for right iliac fossa tenderness.
Pseudo-obstruction Causes
1. Retroperitoneal irritation:
- Blood
- Urine
- Fracture spine and pelvis
2. Drugs:
- Levodopa
- Tricyclic antidepressants
3. Metabolic:
- Uraemia
- Diabetes
- Myxoedema
- Hypokalaemia
4. Viral infections
Pseudo-obstruction Treatment
- It is conservative, provided acute abdomen is ruled out.
- Colonoscopic decompression is the method of choice.
- Prokinetic drugs such as cisapride or mosapride have been tried in selected cases.
- Rarely, even after colonoscopic decompression, caecal tenderness continues. If distension persists, laparotomy followed by tube caecostomy may have to be done.
Chronic Mesenteric Ischaemia
It is a form of severe atherosclerotic disease affecting multiple mesenteric arteries. Most of patients are asymptomatic due to rich collateral network. The most common cause—is atherosclerosis. Other causes are vasculitides—Takayasu disease, and coarctation of the aorta.
Women are more commonly affected than men. When a patient is not eating, the circulatory demands of the resting bowel are easily met and there is no pain.
- After eating, in times of high demand, pain occurs.
- Hence called postprandial pain. Pain typically begins 15 to 45 minutes after eating and is described as crampy, affecting the upper and periumbilical abdomen. It is due to a phenomenon called the “Gastric steal” phenomenon.
- A metabolically active stomach “steals” from the splanchnic circulation. Fixed proximal arterial obstruction does not allow for blood volume to compensate. Small bowel ischaemia and pain follow.
- Patients develop an aversion to eating or “food fear” as the disease progresses.
- Over some time, significant weight loss occurs.
- Triad of CMI: Postprandial pain, food fear and weight loss.
- CT angiography is the investigation of choice.
- Endovascular therapy stenting and bypass grafts can be used. Endarterectomy can also be done if significant thrombus is present in the SMA.
Chronic Mesenteric Ischaemia Strictures
Common causes are tubercular stricture of the ileum or jejunum in
- India and Crohn’s disease in the Western world.
- Radiation stricture, ischaemic strictures and nonspecific strictures are the other causes.
- Malignant strictures.
- Carcinoma rectosigmoid junction tumours. Small bowel enema or enteroscopy are very useful investigations.





Stricture Causes
- Hirschsprung’s disease—congenital megacolon
- Atresia and stenosis
- Arrested rotation with bands
- Volvulus neonatorum
- Meconium ileus
- Imperforate anus
Intestinal Obstruction—Special Causes
1. Adhesive Obstruction
- Firstly, strangulation should be ruled out by clinical and radiological tests. extended nonoperative therapy may be advised, for example, if one can wait for 48 hours in a case of intestinal obstruction.
- In these cases, 4–6 days of waiting is sometimes worth it, especially in a patient who has been operated many times earlier.
- During this extended period, careful monitoring is important to look for any new symptoms/signs of strangulation.
- Early postoperative adhesions (bread and butter adhesions) can also be given extended nonoperative therapy because mostly it is partial obstruction.
2. Intestinal Obstruction In Crohn’S Disease
- As far as possible, resection should be avoided in Crohn’s disease because the aim is to save as much as possible.
- 30% of patients eventually develop obstruction which requires resection.
- Again, if possible do strictureplasty
- Strictureplasty should not be done in patients with intra-abdominal abscesses or intestinal fistulae.
- Some cases of Crohn’s obstruction also respond well to medications—one more reason for nonoperative treatment.
3. Intestinal Obstruction In Pregnancy
- The commonest cause of intestinal obstruction in pregnancy and puerperium is adhesive bands.
- Volvulus is the second most common cause of intestinal obstruction—the intestine volvulates around an adhesive band and that is why the primary cause is adhesive bands
- Inguinal hernia and intussusception are the other causes.
- The consequences of intestinal obstruction in pregnancy do not differ from those found in nonpregnant women except that in the pregnant patient, a second entity, the foetus, is also threatened.
- Most of the intestinal obstructions tend to occur in the third trimester.
- Maternal mortality for intestinal obstruction in pregnancy (10–33%) is higher than in nonpregnant patients.

- In the first half of the pregnancy, nausea, vomiting and episodes of constipation are quite common. Hence, they are confused for hyperemesis gravidarum, acute duodenal ulcer and gastritis.
- In the second half of the pregnancy, symptoms can be confused for toxaemia, constipation, Braxton Hicks contractions, etc.
- Ultrasound can help in the diagnosis by detecting dilated intestinal loops, fluid in the peritoneal cavity and intussusception. It also helps to rule out ovarian torsion, gallstone disease, etc.
- Premature labour can be prevented with tocolysis (abolition of uterine contraction).
- Abdominal surgery in the third trimester does not induce labour.
- Negative laparotomy carries a small risk of disturbing the pregnancy.
- Volvulus and intussusception are the two major causes of small intestinal obstruction in pregnancy.
- Both can give rise to gangrene. Hence an intervention is required before gangrene sets in.
- The diagnosis and treatment of a pregnant patient suspected of having a bowel obstruction should be no different from those given to a nonpregnant one.
4. Ileosigmoid Knotting
It is rare type of knotting between sigmoid and ileum carrying significant mortality if not treated timely.
Ileosigmoid Knotting:
- It is also called compound volvulus.
- The predisposing factor is long pelvic mesocolon.
- The ileum twists around the sigmoid colon resulting in gangrene of the ileum or sigmoid colon or both.
- Even though the sigmoid is also twisted, features are similar to small intestinal obstruction—not massive distension as seen in sigmoid volvulus.
- Resection anastomosis of gangrenous segment followed by anastomosis of the bowel (ileoileal/colic and colocolic).
5. Iliac Crest Graft Hernia With Obstruction
- This is also a rare hernia following bone graft removal from the iliac crest for treatment of fractures.
- Iliac crest is the common donor site of bone grafts. If the bone graft removed is large, the intestines can herniate resulting in intestinal obstruction.
- Tenderness in the surgical site scar can cause diagnostic difficulty.
- It is confused for haematoma.
- CT scan gives the diagnosis.

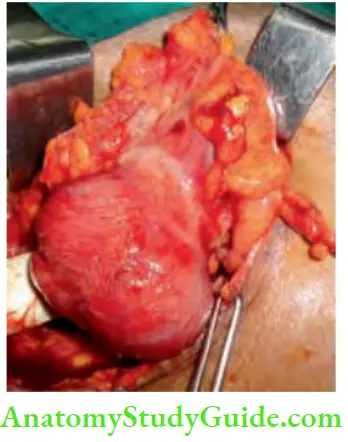
Following is the case report of a patient who had undergone an iliac crest bone graft and developed a hernia
Intestinal Obstruction Clinical Notes:
- A 50-year-old man presented to the casualty with abdominal pain, vomiting and distension. Features were suggestive of intestinal obstruction. On examination, there was a bulge in the region of right iliac fossa—more lateral.
- There was a scar of a bone graft incision. On questioning the patient, he says that he had fractured the humerus. Two months back, nailing and bone grafting had been done.
- Ultrasound revealed bowel loops. CT scan showed a large bone graft defect with herniation of the intestines resulting in intestinal obstruction.
- Emergency surgery, reduction of hernia contents and mesh repair were done. Recovery was uneventful.
6. Food Bolus Obstruction
This complication can occur, particularly when a GJ or partial gastrectomy is done.
Factors Precipitating this Condition:
- Unmasticated, undigested particles
- Coconut pieces, jackfruit seeds gulped coins, etc.
- They get impacted in the terminal ileum which is the narrowest portion of the gut.
Treatment: Squeeze the bolus into the caecum. Otherwise, enterotomy and removal may be necessary.
7. Obstruction Due To Internal Hernia
Syn: Stammer’s Hernia:
1. These are rare causes of intestinal obstruction. Due to some congenital defect in the mesentery, the floating, mobile intestines can herniate
The defect may be in:
- Mesentery
- Transverse mesocolon or
- Broad ligament
- Foramen of Winslow
Hence, whenever a surgical procedure is done for resection of the bowel or GJ, etc. Once the anastomosis is completed, the rent in the mesocolon as in GJ or rent in the small bowel mesentery should be closed.
2. Herniation can also occur through one of the potential spaces (fossae) in and around a viscus.
Internal Hernia:
Wherever a defect is present which is an anatomically present recesses or congenital or following surgery, loop of the small intestine can herniate resulting in hernias.
- They are difficult to diagnose. The diagnosis is by exclusion.
- Triggering factors: Inflammation in the vicinity with or without an adhesion and band triggers herniation and complications.
- Most of these cases present as acute abdomen with features of intestinal obstruction.
- CT scan is the best investigation in such cases.
- It should be remembered that an important vessel runs in the close vicinity of these sites in most of cases.
- Treatment is reduction, suturing the defect or resection anastomosis if the intestine is gangrenous taking care not to damage the vessel. Decompression without dividing the constricting ring may be required
Duodenal Fossa:
- Left paraduodenal fossa: The inferior mesenteric vein lies very close to the free border here.
- Right duodenojejunal fossa: The superior mesenteric artery runs in its free border.
Colonic Fossa:
- Superior ileocaecal fossa
- Inferior ileocaecal fossa
- Sigmoid fossa
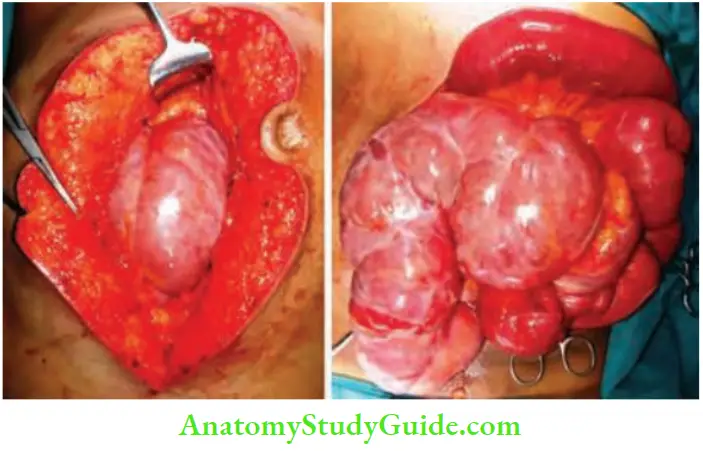
8. Abdominal Cocoon Syndrome
It is characterized by small bowel encapsulation by a fibro-collagenous membrane or “cocoon”. It is a rare cause of intestinal obstruction secondary to kinking and/or compression of the intestines within the constricting cocoon.
Three types have been recognized:
- Primary form: Primary form is probably caused by subclinical peritonitis leading to the formation of a chemical peritonitis was caused by retrograde menstruation, leading to the formation of a cocoon. This was first reported by Foo1 KT, et al. and he coined the term “abdominal cocoon” in 1978.
- Secondary: Secondary causes include the placement of Le Veen shunts for refractory ascites, continuous ambulatory peritoneal dialysis, systemic lupus erythematosus, use of povidone iodine for abdominal wash-out, an adrenergic blocker practolol, etc.
- Tuberculosis: Tuberculosis also is a factor in a few cases.
Diagnosis is established by CECT scan and treatment is separation of bowel loops and removal of the membrane in toto or in pieces.
Intestinal Obstruction Clinical Notes:
- We had a 30-year-old man with nil previous history of abdominal pain or any illness, who presented to the hospital with colicky abdominal pain, 2 times bilious vomiting and distension.
- On examination tympanitic vague mass was palpable in the right iliac fossa. X-ray was suggestive of intestinal obstruction. Abdominal ultrasonography revealed clustering of the small bowel loops in the right iliac fossa.
- CECT was reported as intestinal obstruction secondary to internal herniation. An emergency exploratory laparotomy was done. A cocoon with matted loops were found in the right iliac fossa.
- An attempt to separate the cocoon resulted in multiple tears, it was not possible, hence resection and anastomosis of about 20 cm of the ileum followed by ileocolic anastomosis was done. The patient recovered completely from obstruction and was discharged.
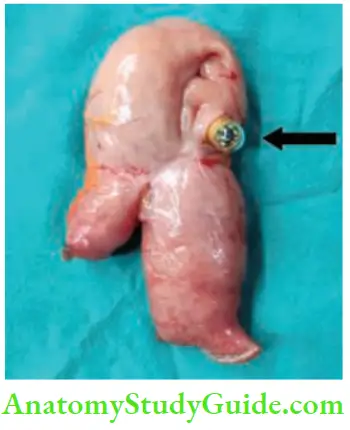
9. Capsule Obstruction
- Capsule endoscopy is done for evaluation of small intestines, major indication being occult bleeding or diarrhoea—causes can be tumours or tuberculosis or Crohn’s disease, etc.
- Capsule can get stuck at the site of ulcer or stricture or a bent intestinal loop due to adhesions. In such patients, it needs to be removed along with the intestine.
10. Acute Large Bowel Obstruction
Details about the causes of large bowel obstruction, however, a few important points have been given in Ten Commandments.
Ten Commandments While Treating Intestinal Obstruction:
- Should rule out pseudo-obstruction before exploring the abdomen.
- Should do limited contrast study or CT scan
- Should resuscitate the patient before surgery
- Should take into account, the general condition of the patient before resection anastomosis.
- Should consider right hemicolectomy or extended hemicolectomy for right-sided growth which is operable.
- Should consider single-stage resection anastomosis also for left-sided growth provided the general condition of the patient is good and on table lavage is given before the anastomosis.
- Should consider exteriorisation of gangrenous bowel in a very sick patient.
- Should consider a simple diversion colostomy in moribund patients in rectosigmoid obstructions (it is a common problem).
- Should not do anastomosis in cases with faecal contamination, peritonitis, haemodynamic instability or possible ischaemia of the remaining colonic segments.
- Should mark the probable stoma site.
Leave a Reply