Renal Function Test
Renal function tests are done with the following objectives
- To find probable renal damage.
- To assess the severity of renal damage.
- To diagnose renal disease.
- To monitor the progress of renal disease.
Indication of Renal function test
- Older age.
- Family history of Chronic Kidney disease (CKD).
- Decreased renal mass.
- Diabetes Mellitus (DM).
- Hypertension (HTN).
- Autoimmune disease.
- Systemic infections.
- Urinary tract infections (UTI).
- Nephrolithiasis.
- Obstruction to the lower urinary tract.
- Drug toxicity.
Renal Function Test can be divided in the following groups
- Urine analysis.
- Blood analysis.
- Renal Clearance test.
- Renal imaging.
- Renal biopsy.
Urine analysis
Urine analysis is done under following heading.
- Urine analysis Volume:
Normal volume is 800ml-2500ml/day
Anuria 0-50ml/day
Oliguria < 500ml/day
Polyuria > 3L - Urine analysis Color:
Normal:- light yellow (due to Urochrome pigment)
Brownish-yellow:- hepatic and post hepatic jaundice
Cloudy appearance:- precipitation of urate and calcium phosphate in strongly alkaline urine.
Frothy appearance: – Proteinuria
Red dark brown: – Porphyria - Urine analysis Specific gravity:
Normal: – 1.003- 1.030 - Urine analysis pH:
Normal: – 4.5-8 - Urine analysis Chemical examination:
- Proteinuria: – when > 150mg protein is excreted per day.
- Glycoseuria: – when glucose is present in urine.
- Ketoneuria: – when ketones are present in urine (acetone, acetoacetic acid, B-hydroxybutyric acid).
- Bilirubinuria: – when excess bilirubin is present in urine.
- Haemogobulinuria: – it seen in intravascular hemolysis, Hb appears in the urine.
- Haematuria: – presence of blood in urine.
- Urine analysis Microscopic examination:
- Cast:
- Urinary casts are formed in the distal convoluted tubule (DCT) or the collecting duct (distal nephron). Hyaline casts are formed by a mucoprotein (Tamm – Horsfall protein) which is secreted by tubule cells.
- Red blood cells may stick together and form red blood cell casts which indicates of glomerulonephritis or severe tubular damage.
- White blood cell casts indicate acute pyelonephritis. Their presence is a sign of inflammation of the kidney.
- When cellular casts stay in the nephron for some time, the cells may degenerate to form a coarsely granular cast later form a finely granular cast, and finally form a waxy cast.
- Crystals: Calcium oxalate, calcium phosphate, triple phosphate, and uric acid crystals are present normally in the kidney.
- Uric acid crystals are diamond or barrel-shaped crystals of yellow to orange-brown,
- Urate crystals are the salt arise of uric acid crystals and are composed of uric acid plus calcium or sodium. Urate crystals are needle-shaped and may be associated with gout.
- Triple phosphate crystals (struvite crystals) consist of magnesium ammonium phosphate. These are colorless 3- to 6-sided rectangular prisms (“coffin-lid”-shaped appearance). They are formed in neutral to alkaline pH urine.
- Calcium oxalate crystals are colorless square envelopes or octahedron crystals. They are common at any pH. These are also related to the presence of kidney stones and ingestion of ethylene glycol.
- Cysteine crystals are flat, colorless, hexagonal crystals that resemble stop signs. They indicate cystinuria
- “Amorphous” crystals appear as aggregates of finely granular material of any shape. They can be composed of urates, phosphates or xanthine.
- Cells:- microscopic examination may show RBC, WBC, Pus cells, epithelial cells.
- Cast:
- Urine analysis Bacteriological examination: –
- The presence of bacteria indicates a urinary tract infection.
Urine analysis Blood analysis
- Blood urea Nitrogen (BUN):- It is a byproduct of protein metabolism. Its normal level is between 7 and 20 mg/dL. Rise in BUN level, indicates a decrease of kidney function. The real urea concentration is BLN x 2.14.
- Serum creatinine-creatinine is a waste product of muscle breakdown. Its levels in the blood vary depending on age, race and body size’ Normal range is 0.6-1.3 mg/dL. A creatinine level of greater than 1.2 for women and greater than 1.4 for men may be an early sign of a decrease of kidney function.
- Serum protein levels – they are decreased if there is significant proteinuria with renal failure.
- Serum electrolytes – sr. Na+, K+, ca+, PO43-, Mg2+ levels are deranged.
- Indices
- GFR is calculated from the serum creatinine level using age and gender with adjustment for ethnic groups. Normal GFR varies according to age. The normal value for GFR is > 90. GFR <60 is a sign of decrease of kidney function. It can be calculated by the Cockcroft-Gault Equation (Adults).
females multiply by 0.85
- GFR is calculated from the serum creatinine level using age and gender with adjustment for ethnic groups. Normal GFR varies according to age. The normal value for GFR is > 90. GFR <60 is a sign of decrease of kidney function. It can be calculated by the Cockcroft-Gault Equation (Adults).
-
- Fractional excretion of sodium
-
- Excretion of Urea
FEUrea: (ULIN ÷ BUN) X (Serum Creat. ÷ Urine Creat.) X l00% - Renal Failure Index
RFI = Urine sodium X Plasma creatinine Urine creatinine
- Excretion of Urea
Renal Clearance test
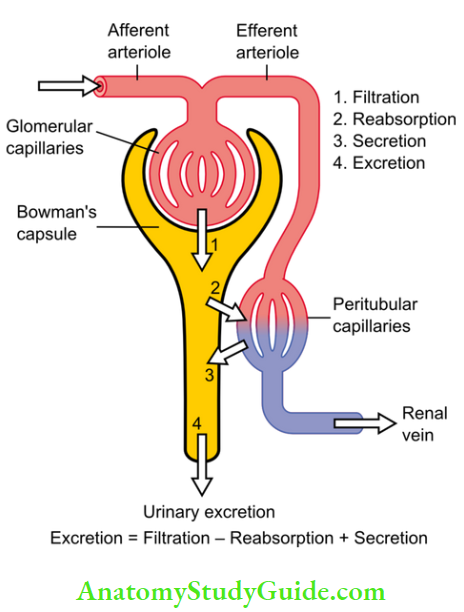
To understand the concept of clearance we should understand some basic renal processes.
Glomerular filtration is the passive filtration of the blood through the glomerulus.
Tubular reabsorption is the process that moves solutes and water out of the ultra-filtrate and back into your bloodstream.
Tubular secretion is the process that moves substances from peritubular capillaries to the renal tubular lumen; this process is opposite of reabsorption.
Urinary excretion: Filtration – absorption+ secretion
Renal clearance
It is the volume of plasma from which a substance is completely removed per unit of time; the usual units are ml/min. it reflects the rate at which a particular substance is removed from plasma into the urine by the kidneys. It is a “virtual” volume that depends on two major factors.
- Renal extraction ratio: It is the fraction of substance entering the kidney that was removed in a single pass into the urine.
Extraction ratio: (Pa-Pv)/Pa
e. g. para aminohippuric acid (PAH) is almost completely excreted from the kidney in in a single pass to urine, and thus almost none is found in the venous return (Pv – 0). Therefore, the extraction ratio of PAH -1. - Blood /plasma flow to the organ: If i.e., ER: l’0, then changes in blood flow is the rate-limiting factor. Conversely, if ER is very low, changes in blood flow are less important.
Clearance is calculated as
Clearance of substance X plasma concentration of substance = Urinary concentration of substance (US) X Urine flow rate (V) i.e.
(CS) x (PS) = (us) x (v)
Clearance of substance (CS) = (US) X (V) / (PS)
General properties of a substance that can be used to measure clearance:
- Its arterial and venous concentration should be measurable.
- It should not be metabolized.
- It should not be stored.
- It should not be synthesized by the kidney.
- It should not affect renal blood flow.
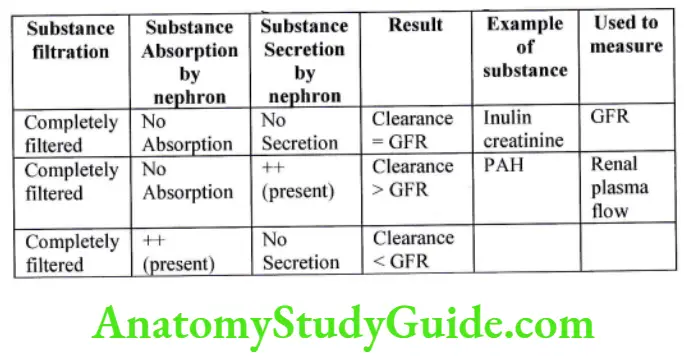
Measurement of Glomerular Filtration Rate
In addition to the above 5 properties, substance that can be used to measure GFR should have the following properties.
- It should be completely filtered.
- It should not be reabsorbed.
- It should not be secreted.
These properties are demonstrated by
- Inulin
- Creatinine
- Urea
Inulin clearance test
- Inulin is a dye, fructopoly sachharide extracted from roots of plants
- It does not exist naturally in body
- It is biologically inert / nontoxic
- It is neither stored nor metabolized in the body
- Its concentration can be easily measured
- It is freely filtered neither reabsorbed nor secreted
Cinulin = Uinuln X V / Pinurin
If Uinulin = 125 mg/ml
V = lml/min
Pinlin = lmg/ml
Then 125 ml/min; thus GFR = 125 ml/min
Urine analysis Clinical significance:
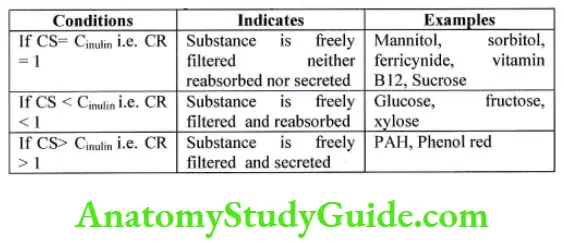
The Inulin clearance test is used as an indicator of the plasma clearance mechanism. Clearance ratio (CR) = clearance of substance (CS)/ clearance of inulin (Cinulin)
Creatinine clearance test:-
- Creatinine is a byproduct of muscle metabolism so not a perfect marker.
- It is freely filtered and a small amount is secreted so less accurate than the inulin clearance test.
- A slight error in measuring plasma creatinine leads to an overestimated plasma creatinine value.
- The above two effects cancel each other.
- As it does not require intravenous infusion it is widely used.
- Plasma creatinine concentration is 0.6-l.5mg/dl.
- Creatinine clearance is 80-l l0 mg/min.
Urea clearance test:-
It is the end product of protein metabolism.
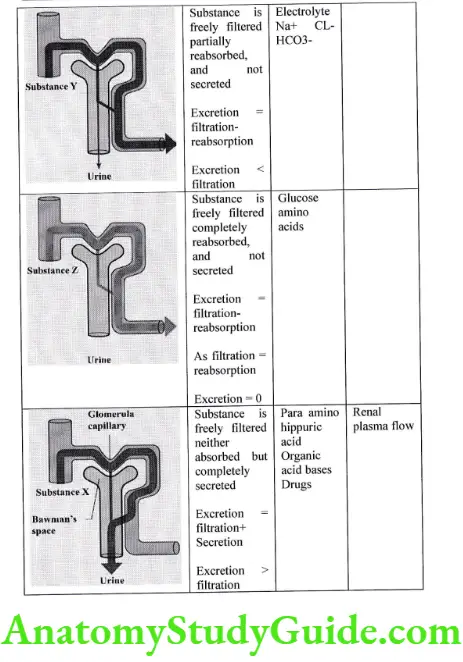
It is freely filtered and a small amount is reabsorbed (Clearance < GFR) so less sensitive.
Method
- At the beginning of test, the patient is asked to empty the bladder. After t hour collect t hr. urine sample. Measure urinary urea levels and serum urea level.
- If urinary output > 2ml/min, maximal urea clearance test is used Curea = Uurea X V/Purea.
- If urinary output < 2ml/min, a standard urea clearance test is used. Curea = Uurea X√V/Purea.
- Normal values of Curea by maximal urea clearance test = 75ml/min.
- Normal values of Curea by standard urea clearance test = 54 ml/min.
Measurement of renal plasma flow
Clearance method
Fick’s principle
Para amino hippuric acid (PAH) clearance test
- PAH is an amide derivative of the amino acid glycine and para-aminobenzoic acid.
- It is not naturally found in humans; so need to be infused intravenously for diagnostic use.
- It is freely filtered, and secreted in urine.
- Its extraction ratio is 0.9 i.e. 90% of PAH is removed in single circulation, venous concentration is nearly zero.
- So it is used to measure renal plasma flow.
- Rsenal Plasma Flow = CPAH = UPAH X V/PPAH.
Ficks principle
It states that the amount of substance excreted by the kidney per unit of time is equal to its arterio-venous difference across kidney times the blood flow
Amount of substance excreted by kidney = arterio-venous difference across kidney (A-V) X Renal Blood flow (RBF)
RBF = Amount of substance excreted by kidney / (A-V)
As kidney filters plasma, we can replace RBF by Renal Plasma Flow (RPF)
So RPF = substance excreted by kidney / (A-V)
We know that substance excreted by kidney b= Urinary concentration of substance (Us) X Urinary Flow rate (V)
RPF = Us X V / (A(PAH)-V(PAH))
PAH is used to measure RPF. Its extraction ratio is 0.9, i.e. 90% PAH is removed from the kidney in a single pass from kidney so we can consider V(PAH) = 0
If we consider V(PAH) = 0, we denote RPF as Effective Renal Plasma Flow (ERPF)
Also, the Kidney arterial plasma concentration of PAH is equal to the Peripheral Venous plasma concentration of PAH i.e. we can replace A(PAH) in the equation by P(PAH)
Thus the ERPF = Us X V / P(PAH)
eg P(PAH) = 0.0lmg/ml, Us = 7mg/ml, V = 0.9ml/min
ERPF: (7 mg/ml X 0.9ml/min) /0.01 mg/ml = 630 ml/min
So, after doing cross multiplication, RPF = (ERPF X 1)0.9 = 630/09 = 730 ml/min
As blood consists of plasma and Haematocrit, we can write the following equation
Blood = Plasma (P) + Haematocrit (H)
If we consider blood as I then we can write (1 = P+H) —– {1}
We can rewrite the equation as P : l-H —- {2}
Considering equation 1 and 2
RBF = 1 X RPF/ l-H
= 7OO/1-0.45 = 700/0.55, Renal Blood Flow = 1273 ml/min
Free Water clearance
For assessing urinary dilution or concentration, urinary Osmolarity, and volume must be measured. Urinary Osmolarity ranges from 50mOsm/1 to l200mOsm/kg H20 which corresponds to urinary volume of 18 I to 0.51.
The critical basic process of dilution or concentration of urine is the separation of solute from H2O
If more solute is separated then urine becomes concentrated, and if solute is not separated then urine becomes dilute. Kidney produces a quantity of water which is “free of all solutes”. When it is excreted from the body urine becomes dilute, when it is not excreted from the body urine becomes concentrated. Free water clearance quantifies the kidney’s capability to generate solute-free water.
The kidney produces urine composed of solute and solute-free water. The amount of solute cleared from plasma is “Osmolur clearance”. The amount of solute-free water cleared from plasma is “Free water clearance”. “Free water clearance” represents the volume of clean water that must be added to or removed from urine to make it iso-osmotic with plasma.
Urine flow: Osmolar clearance + Free water clearances
V = Cosm + CH2O
CH2O = V- Cosm U = urinary concentration of substance
We know Cosm = U X V/P V = urinary flow rate
CH2o = V- {(U X V) / P} P = plasma concentration of substance
CH2o = V {l-(U/P)}
Interpretation
CH2o= 0, urine is iso-osmolar with plasma
CH2o > 0 urine is dilute than Plasma
CH2o < 0 urine is more concentrated than plasma
CH2o depends on
- ADH
- Water intake
Applied:
Renal imaging
- Plain X-ray of Abdomen: It gives a rough idea about the size shape position of the kidney. It helps to detect radiopaque renal stones.
- Intravenous pyelography: An intravenous pyelogram (IVP) is an x-ray examination of the kidneys, ureters and urinary bladder which uses iodinated contrast material injected into veins. contrast material collects in the kidneys and urinary tract, focusing these areas bright white on x-ray images. An IVP allows to view and assess the anatomy and function of the kidneys ureters and bladder.
- Ultrasonography: It may be used to look for abnormalities in the size or position of the kidneys or for obstructions such as stones or tumors.
- Computed Tomography scan: It may also be used to look for structural abnormalities and the presence of obstructions. This test requires the use of intravenous contrast dye for those with kidney disease.
Renal biopsy
It is a histological examination of tissue removed from a living body to discover the presence, cause, or extent of a disease. A kidney biopsy is done by using a thin needle having a sharp cutting edge to cut small pieces of kidney tissue for examination under a microscope.
Indication for renal biopsy:
- To identify a specific disease process.
- To evaluate the amount of damage to the kidney.
- When acute or chronic renal allograft rejection is suspected.
Leave a Reply