Thyroid Gland Introduction
- Thyroid gland is an endocrinal gland present in the neck secreting T3 and T4 hormones. It is richly vascular and highly functional.
- Effects of hormonal changes affect every part of the body such as central nervous system, cardiovascular system, gastrointestinal system and reproductive system.
Describe the applied anatomy and physiology of thyroid.
Table of Contents
Read And Learn More: General Surgery Notes
- It is also the site of various diseases—a simple enlargement, toxicity and malignant transformation.
Surgical Anatomy Of Thyroid Gland
Development and Anatomy:
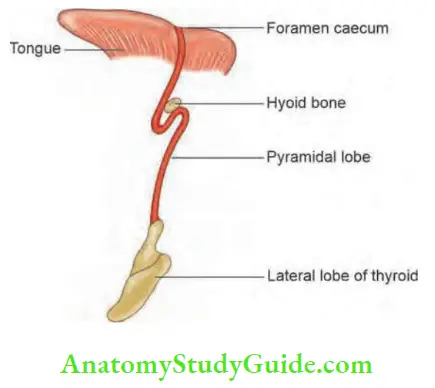
- It develops from median downgrowth (midline diverticulum) of a column of cells from the pharyngeal floor between first and second pharyngeal pouches. • The descent is anterior to structures that form hyoid bone and larynx.
- By 6 weeks of intrauterine life, the central column, which becomes the thyroglossal duct, gets reabsorbed.
- The duct bifurcates to form thyroid lobes.
Tubercle of Zuckerkandl: It is a posterolateral extension of thyroid gland. Incidence—30–40%. Arises from lateral anlage.
It is closely related to recurrent laryngeal nerve at surgery. Tubercle points to the intersection between the nerve and inferior thyroid artery. It should be removed, if present specially in thyroidectomy for malignancies.
- Pyramidal lobe is formed by a portion of the duct.
- Calcitonin producing parafollicular cells or C cells originate from the fourth branchial pouch.
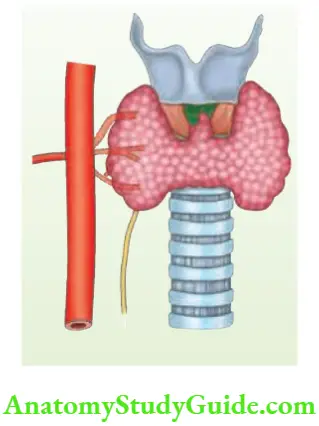
- Thyroid gland is present in the neck, enclosed by pretracheal fascia which is a part of deep cervical fascia. It has a right and left lobe joined by the isthmus in front of 2nd, 3rd and 4th tracheal rings. It weighs about 20–25 g. A projection from the isthmus usually on the left side is called pyramidal lobe. It is attached to the hyoid bone by a fibrous band or muscle fibres called levator glandulae thyroideae.
- Thyroid is covered by true capsule which cannot be separated. However, another layer (false capsule) which is surrounding thyroid gland can be separated.
- Suspensory ligament of Berry: This pair of strong condensed connective tissue binds the gland firmly to each side of cricoid cartilage and upper tracheal rings.
- Pretracheal fascia, which is part of deep cervical fascia splits to invest the gland. These structures (ligament of Berry and pretracheal fascia) are responsible for thyroid gland moving with deglutition.
Arterial Supply:
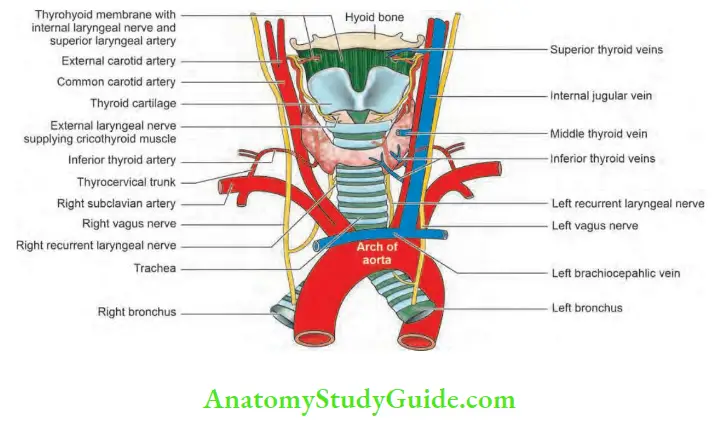
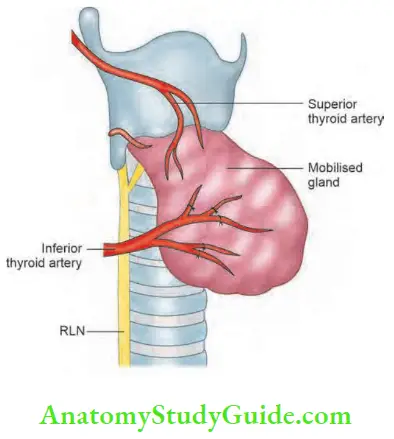
- Superior thyroid artery, a branch of the external carotid artery, enters the upper pole of the gland, divides into anterior and posterior branches and anastomoses with ascending branch of inferior thyroid artery. Since the upper pole is narrow, ligation is easy.
- Inferior thyroid artery is a branch of thyrocervical trunk1 and enters the posterior aspect of the gland. It supplies the gland by dividing into 4 to 5 branches which enter the gland at various levels (not truly lower pole).
- Inferior thyroid artery used to be ligated well away from the gland to avoid damage to RLN. However, ligation of these arteries on both sides will cause permanent hypoparathyroidism.
- Hence, the current practice is to identify and ligate the branches of inferior thyroid artery (3–4) separately.
- Thyroidea ima artery is a branch of either brachiocephalic trunk or direct branch of arch of aorta and enters the lower part of the isthmus in about 2 to 3% of the cases.
Venous Drainage:
- Superior thyroid vein2 drains the upper pole and enters the internal jugular vein. The vein follows the artery.
- Middle thyroid vein is single3, short and wide and drains into internal jugular vein.
- Inferior thyroid veins form a plexus which drain into innominate vein. They do not accompany the artery.
- Kocher’s vein is rarely found (vein in between middle and inferior thyroid veins)
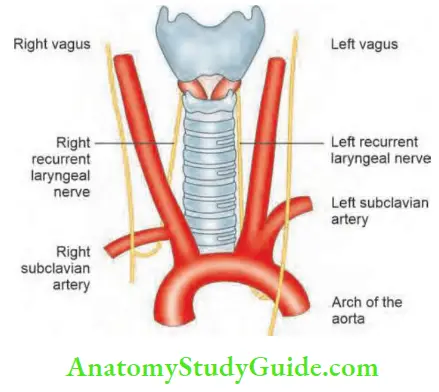
Nerves in Relationship with Thyroid Gland:
Superior laryngeal nerve S(LN): The vagus nerve gives rise to superior laryngeal nerve, which separates from it at skull base and divides into two branches. The larger internal laryngeal nerve is sensory to the supraglottic larynx. The smaller external laryngeal nerve runs close to the superior thyroid vessels and supplies cricothyroid. This nerve has been called as Amelita Galli-Curci nerve1.
- This nerve is away from the vessels near the upper pole. Hence, during thyroidectomy, the upper pedicle should be ligated as close to the thyroid as possible.
- Cricothyroid space of Reeves: It lies between the cricothyroid muscle medially and upper pole of the thyroid lobe laterally. When we hold the upper pole of the thyroid gland with Babcock’s forceps and retract the lobe infero-laterally, it opens up the space and SLN will be visible.
Recurrent laryngeal nerve (RLN) is a branch of vagus, hooks around ligamentum arteriosum on the left and subclavian artery on the right and runs in the tracheoesophageal groove near the posteromedial surface.
- Close to the gland, the nerve lies in between (anterior or posterior) branches of inferior thyroid artery.
- On the right side, it is 1 cm within the tracheoesophageal groove.
Recurrent Laryngeal Nerve at Surgery:
- Lack of colour—white in colour
- Lack of elasticity
- Lack of pulsation
- Longitudinal vein on the surface
- Longitudinal course
- Location—Riddle’s triangle—it is between inferior thyroid artery superiorly, carotid artery laterally and trachea medially. From here RLN runs upwards to enter larynx at greater cornu of thyroid cartilage, Riddle’s triangle is also called Beahrs triangle.
Recurrent Laryngeal Nerve Anomalies:
- The nerve traverses through the gland in about 5–8% of cases.
- The nerve may be very closely adherent to the posteromedial aspect of the gland.
- Nerve not seen—may be far away in the tracheooesophageal groove.
- Nonrecurrent, recurrent laryngeal nerve is found in about 1 in 1,000 cases. The nerve has a horizontal course.
- In 25% of the cases, it is within the ligament of Berry.
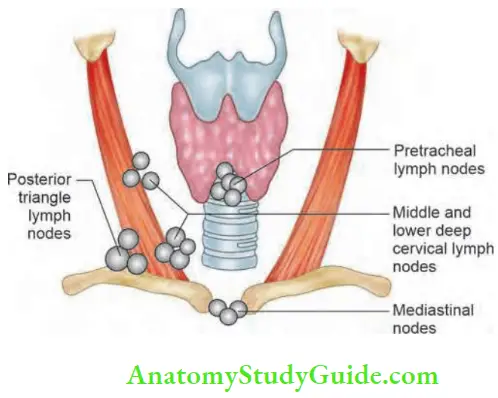
Lymphatic Drainage of Thyroid:
- Subcapsular lymphatic plexus drains into pretracheal nodes (Delphic nodes means uncertain) and prelaryngeal nodes which ultimately drain into lower deep cervical nodes and mediastinal nodes.
- The chief lymph nodes are middle and lower deep cervical lymph nodes (Levels 3 and 4).
- Supraclavicular nodes and nodes in the posterior triangle can also be involved in malignancies of the thyroid gland, especially papillary carcinoma thyroid.
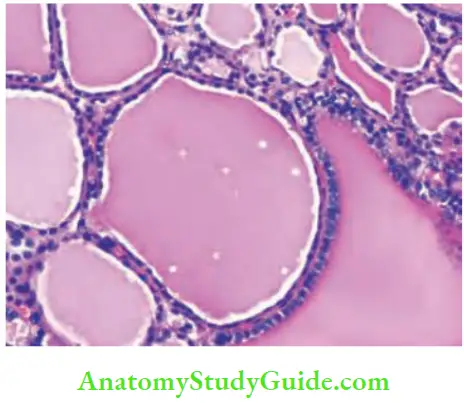
Surgical Anatomy Of Thyroid Gland Histology:
- Microscopically, it is divided into lobules.
- Each lobule has 20–40 follicles.
- Each follicle is lined by cuboidal epithelial cells.
- In the centre, colloid is present which is secreted from epithelial cells in response to calcitonin.
- Parafollicular cells are present in the interfollicular stroma.
Physiology
Tri-iodothyronine (T3) and thyroxine (T4) are the hormones secreted by the thyroid gland. Dietary requirement of iodine per day is 100–200 mg or 0.1 mg. Sources of iodine are milk, dairy products and sea food including fish.
Steps involved in the synthesis of these hormones:
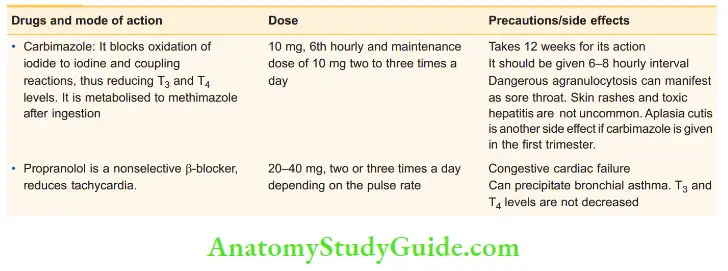
- Iodide trapping from the blood into the thyrocyte is the first step in the formation of T3 and T4 . Thiocyanates and perchlorates block this step.
- Oxidation of iodide to inorganic iodine: This step needs the enzyme peroxidase.
- Drugs which block this stage (thioamides) are sulfonamide, PAS (para-amino-salicylic acid), carbimazole and propylthiouracil.
- Formation of iodotyrosines:
- Iodine + Tyrosine = MIT (monoiodotyrosine) and diiodotyrosine (DIT)
- This step is inhibited by thiourea group of drugs, i.e. carbimazole.
- Coupling reactions:
- Coupling of two molecules of DIT results in T4 and one molecule of DIT and MIT results in T3.
- This stage is blocked by carbimazole.
- Hydrolysis:
-
- The hormones combine with globulin to form a colloid-thyroglobulin. They are stored in the thyroid gland and released as required by process of hydrolysis.
- T3 is an important physiological hormone and is fast-acting (few hours). T4 is a slow-acting hormone and takes about 4–14 days to act.
Thyroid Function Tests
Serum T3 and T4 estimation is most commonly performed. Other tests are not commonly done and some of them are obsolete.
1. Serum T3: Normal levels—1.5–3.5 nmol/L
- Most (80%) T3 is produced by deiodination of T4 in the liver, muscle, kidney and anterior pituitary.
- T3 is 3 to 4 times more potent than T4 .
- The half-life of T3 is approximately 24 hours, whereas half-life of T4 is about 7 days.
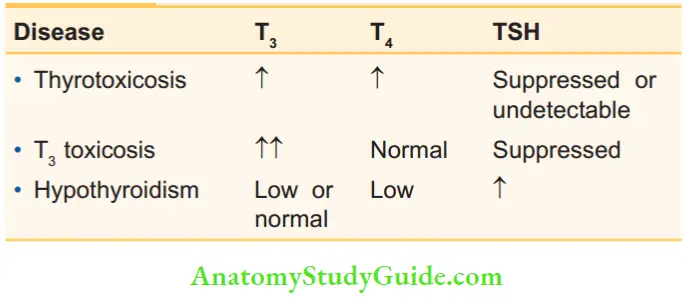
Levels of T3, T4 and TSH in some common conditions:
- Free T3 (3 to 9 pmol/L) is most useful in confirming the diagnosis of early hyperthyroidism, especially in pregnancy wherein levels of free T4 and free T3 rise before total T4 and T3 .
2. Serum T4 : Normal levels—55 to 150 nmol/L
- They are measured by radioimmunoassay.
- In euthyroid state, T4 is the predominant hormone produced by the thyroid.
- Total T4 levels reflect output from the thyroid gland. Both T3 and T4 increase cell metabolism, normal growth, facilitate normal mental development and increase local effects of catecholamines.
- Free T3 (ref range 12–28 pmol/L) and free T4 (3–9 pmol/L). Free T4 estimates are not performed as a routine screening in thyroid disease.
- Use of this test is confined to cases of early hyperthyroidism Graves’ disease where T4 total may be normal but free T4 is raised. In patients with end organ resistance to T4, T4 levels are raised but TSH is normal.
- Free T4 is useful to confirm cases of early hyperthyroidism in which levels of both free T3 and T3 rise before total T3 and T4 .
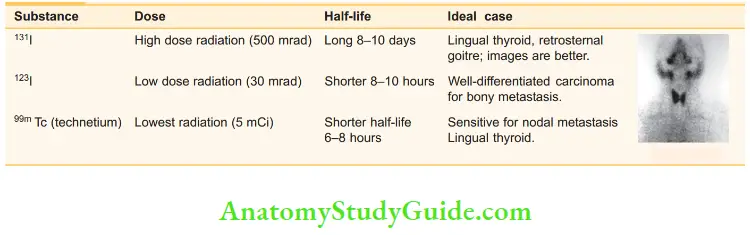
3. Serum TSH (thyroid-stimulating hormone): 0.3–5 IU/ml of plasma. Table 37.1 shows the levels of T3 , T4 and TSH in a few common conditions.
4. Serum thyroglobulin (TG):
- It is produced by thyroid tissue only. Hence, the levels should be low after total thyroidectomy.
- The most important use of this test is to monitor patients after total thyroidectomy for welldifferentiated carcinoma.
- It is not normally released into circulation in large amount but increases suddenly in thyroiditis, Graves’ disease or toxic multinodular goitre (MNG).
5. Serum cholesterol: It is increased in hypothyroidism and decreased in hyperthyroidism.
6. Thyroid autoantibody levels: More than 90% of the patients with Hashimoto’s thyroiditis and 80% of patients with Graves’ disease have antibodies which are called ‘LATS’ (long-acting thyroid stimulator).
- The detection of these antibodies helps in the diagnosis of such cases and also to suspect these diseases before clinical manifestation.
- These include anti-TG, antithyroid peroxidase and thyroidstimulating immunoglobulin.
- Anti-TPO levels >25 µ/ml and anti-thyroglobulin titres more than 1:100 are considered significant.
- TSH receptor antibodies are also present in Graves’ disease. They are largely produced within the thyroid itself.
7. Thyroid scintigraphy: Uptake by both lobes.
8. Serum calcitonin: It is a sensitive marker for medullary carcinoma thyroid. (0–4 pg/ml basal) CEA may also be used as an alternate screening test for medullary carcinoma thyroid.
Thyroid scintigraphy:
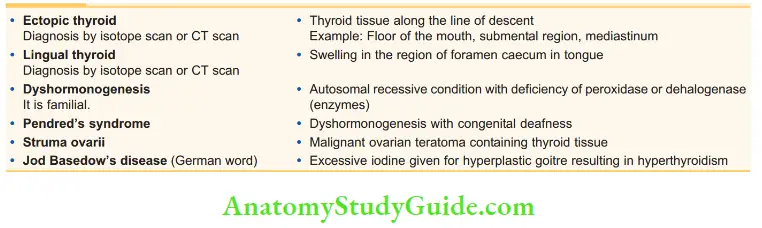
Nomenclature of certain thyroid diseases:
Clinical Examination Of Thyroid Swelling
- Diseases of the thyroid are very common and thyroid swellings are very often common cases in an undergraduate and postgraduate clinical examination.
- Hence, before discussing the various diseases of the thyroid gland, various aspects of the “CLINICS” are discussed in detail below.
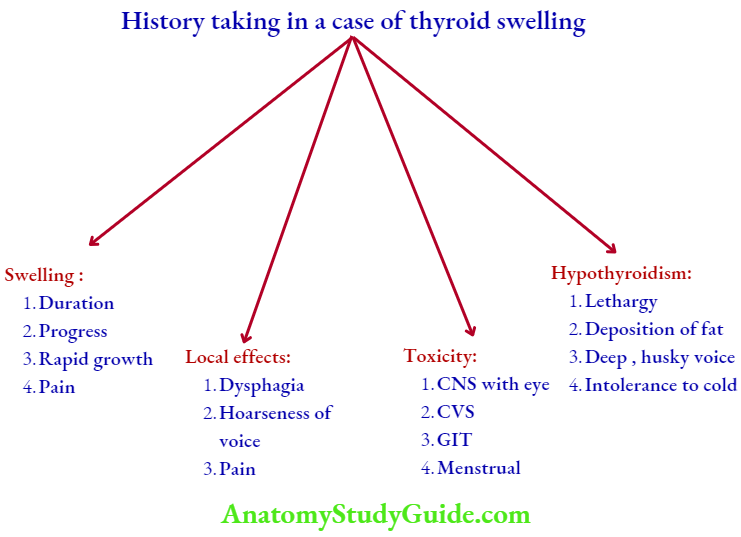
Complaints History Taking
1. Swelling: Long duration of thyroid swelling indicates benign condition, e.g. multinodular goiter (MNG), colloid goitre. Short duration with rapid growth indicates malignancy, such as anaplastic carcinoma. Majority of thyroid swellings do not produce pain.
2. Rate of growth: Usually slow-growing in benign disease. If it is a rapid growth, it can be ‘de novo’ malignancy or malignancy developing in a benign lesion, e.g. follicular carcinoma in MNG. Sudden increase in the size of swelling with pain indicates haemorrhage in the MNG (multinodular goitre).
3. Dyspnoea: Difficulty in breathing in a patient with goiter can be due to the following reasons.
- Small goitre, rapid growth—anaplastic carcinoma infiltrating the trachea.
- When lower border is not seen, retrosternal goitre.
- Hyperthyroidism causing arrhythmias leading to congestive cardiac failure can cause dyspnoea and orthopnoea.
- Long-standing MNG compresses on the tracheal cartilages and produces pressure atrophy of tracheal cartilages. This is called tracheomalacia.
Dyspnoea in Goitre—Causes:
- Infiltration of trachea -Anaplastic carcinoma
- Lower border not seen – Retrosternal goitre
- Tracheomalacia – Long-standing MNG
- Cardiac failure – Secondary thyrotoxicosis
4. Dysphagia is relatively uncommon because oesophagus is a posterior structure and it is a fibromuscular tube.
5. Hoarseness of voice indicates malignancy. It always occurs in carcinoma thyroid infiltrating the recurrent laryngeal nerve (never in benign diseases of thyroid).
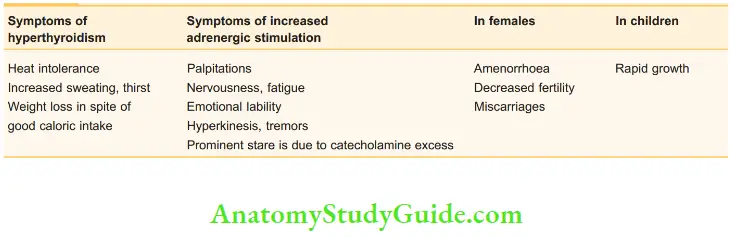
6. Toxic features suggestive of hyperthyroidism.
CNS symptoms are predominantly seen in Graves’ disease.
- Tremors of the hand
- Sweating
- Intolerance to heat
- Preference to cold
- Excitability
- Irritability
- Prominent eyes are observed by other persons. Double vision, oedema of the conjunctiva can be the presenting complaints in late cases.
Graves’ Disease:
- Goitre
- Ophthalmic symptoms
- Irritability
- Tremors
- Restlessness
- Excitability Remember as GOITRE.
Cardiovascular symptoms (CVS) are predominantly seen in secondary thyrotoxicosis. Even though both forms of thyrotoxicosis produce palpitations, it is a significant complaint in multinodular goitre with thyrotoxicosis (secondary thyrotoxicosis). Precordial chest pain and dyspnoea on exertion are late manifestations of secondary thyrotoxicosis.
On Examination
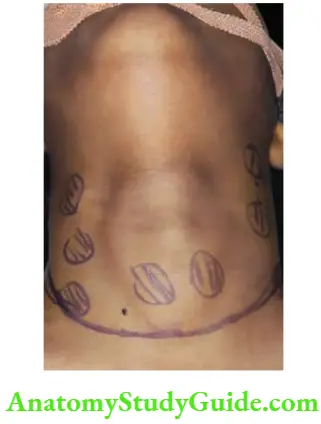
Inspection:
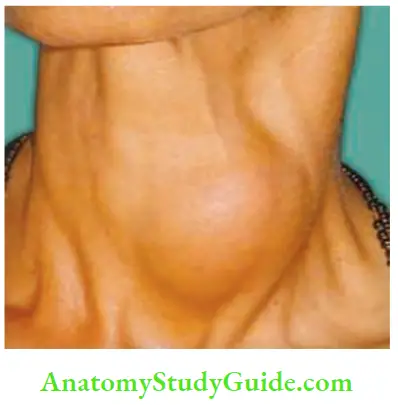
1. The location of the swelling is in front of the neck, extending from one sternomastoid to the other sternomastoid, vertically from suprasternal notch to the thyroid cartilage.
2. The size and shape have to be mentioned.
3. Surface: Thyroid swellings can have the following types of surfaces:
- Smooth—adenoma, puberty goitre, Graves’ disease
- Irregular—carcinoma of the thyroid
- Nodular—multinodular thyroid
4. Borders are usually round.
5. Swelling moves up with deglutition because of the following reasons:
- Thyroid is enclosed by pretracheal fascia which is condensed to form a ligament posteromedially called ligament of Berry.
- These are pairs of ligaments attached above to cricoid cartilage. During deglutition, the cricoid cartilage moves upwards and with it, the thyroid gland (give the patient a glass of water and check for movement with deglutition). This action is by inferior constrictors.
- These muscles mainly do the function of swallowing when food enters from pharynx to upper oesophagus.
- It has two parts—thyropharyngeus arises from thyroid cartilage and cricopharyngeus arises from cricoid cartilage.
- When these muscles act, thyroid and cricoid cartilage moves upwards. Thus, thyroid gland also moves upwards.
- Inferior constrictors are supplied by vagus nerve. These are thickest constrictor muscles.
If there is restriction of movement, it can be due to:
-
- Malignancy with fixity to the trachea
- Retrosternal goitre
- Large goitre because of the size
- Previous surgery
Swellings which Move Upwards with Deglutition:
- Thyroid swellings
- Subhyoid bursitis
- Pretracheal and prelaryngeal lymph nodes
- Thyroglossal cyst
- Laryngocele
6. Movement on protrusion of the tongue suggests thyroglossal cyst. This test should be done when there is a nodule or a cyst in the region of isthmus of the thyroid gland. This test has no relevance in cases of MNG or other thyroid swellings.
Clinical Examination Of Thyroid Swelling Palpation:
It should be done from behind. First mention what parts of thyroid gland are palpable.
- Size, shape, surface and border should be confirmed. Local rise of temperature is a feature of toxic goitres. Very large nodular surface is described as bosselated surface.
- Consistency:
- Soft: Graves’ disease, colloid goitre.
- Firm: Adenoma, multinodular goitre.
- Hard: Carcinoma, calcification in the MNG.
- Confirm the movement with deglutition by holding the thyroid gland.
- Intrinsic mobility of the gland is very much restricted in carcinoma because of infiltration into prevertebral fascia behind or a malignant nodule which starts infiltrating trachea. Otherwise, thyroid gland has hardly any intrinsic mobility. When you try to move it moves with the trachea.
- Sternomastoid contraction test is done when only one lobe is enlarged. In this situation, the examiner keeps the hand on the side of the chin, opposite the side of the lesion and asks the patient to push his hand against resistance. If the gland becomes less prominent (as with thyroid swellings), it indicates the swelling is deep to the sternomastoid muscle.
6. Chin test (neck fixation test) is classically done in multinodular goitre, wherein both lobes are enlarged. The patient is asked to bend the chin downwards against resistance. This produces contraction of both sternomastoids and strap muscles and the gland becomes less prominent.
7. Special tests or methods of examination of thyroid gland:
- Crile’s method is indicated when there is a doubtful nodule. Keep the thumb over the suspected area of the nodule and ask the patient to swallow. The nodularity is appreciated better with this test.
- Lahey’s method of examination of thyroid can be done from front as well as behind. In order to palpate the right lobe, push the gland to the right side and feel the nodules in the posteromedial aspect of the gland. The lobe becomes more prominent and thus nodules are appreciated better.
- Pizzillo’s method is indicated in obese patients especially short-necked individuals. The patient is asked to clasp her hands and press against her occiput with head extended. Thyroid gland becomes more prominent and thus, palpation becomes better.
- Kocher’s test: If gentle compression on lateral lobes produces stridor, it is described as positive. This is due to scabbard1 trachea. Long-standing multinodular goitres causing tracheomalacia and collapse after thyroidectomy resulting in stridor.
8. Position of trachea: In cases of solitary nodule confined to one lobe, trachea is deviated to the opposite side. However, in cases of multinodular goitres, trachea need not be deviated because of symmetrical enlargement of both lobes.
9. Palpation of lymph nodes in the neck. If lymph nodes are significant, it indicates papillary carcinoma of the thyroid.
10. Palpation of common carotid artery: Draw a line from mastoid process to sternoclavicular joint. Then draw a horizontal line from upper border of thyroid cartilage. The point where these two lines meet is the site of bifurcation of common carotid artery.
- This artery should be palpated below this point, against tubercle on the transverse process of cervical 6th vertebra—called carotid tubercle or Chassaignac tubercle.
- The carotid artery can be massaged against this tubercle to relieve the symptoms of supraventricular tachycardia.
- In large multinodular goitres, the artery may be pushed laterally. Hence, pulsations are felt in the posterior triangle.
- Carcinoma of the thyroid engulfs the carotid sheath. Consequently, pulsations may be absent.
- Absent carotid artery pulsation is called Berry sign positive. Since the lumen is not narrowed, superficial temporal artery pulsations are felt normally.
Percussion:
Percussion over the sternum gives a resonant note in normal cases. In retrosternal goitres, it gives a dull note.
Auscultation:
- It should be done in the upper pole because of following reasons: Superior thyroid artery is a direct branch of external carotid artery. It is more superficial than inferior thyroid artery.
- Presence of thrill and bruit are the features of toxic goitre.
Systemic Examination:
- This includes CNS and eye signs, as in Graves’ disease, examination of skeletal system to rule out metastasis as in carcinoma of the thyroid, and examination of cardiovascular system in cases of toxic goitre.
- These have been dealt with in detail in the corresponding topics. Deep tendon reflexes also have to be elicited— there is a slow relaxation phase in hypothyroidism.
Clinical Examination Of Thyroid Swelling Diagnosis:
You need to confirm it is thyroid gland and to mention the disease and functional status. It should be noted that the neural tumours arising from vagus nerve can present in the same location, but it will not move with deglutition.
Anatomical Features of the Thyroid Gland:
- Thyroid gland is in front of the neck
- Deep to pretracheal fascia
- Moves up with deglutition
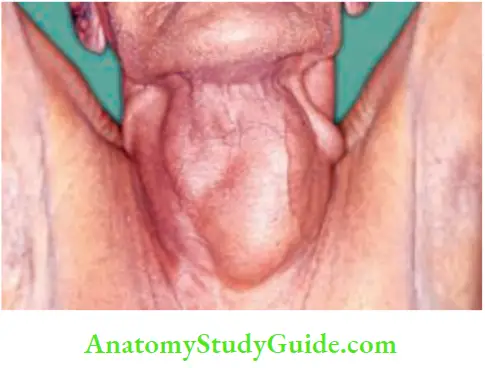
- Butterfly-shaped when whole gland is enlarged
Goitre
Goitre Definition:
Diffuse enlargement of the thyroid gland is described as goitre. (It is derived from the Latin word, Guttur = the throat.)
Classification of Goitre:
1. Simple goitre:
- Puberty goitre
- Colloid goitre, iodine deficiency goitre
- Multinodular goitre
2. Toxic goitre:
- Graves’ disease; diffuse toxic goitre
- Secondary thyrotoxicosis in multinodular goitre
- Toxic nodule; other causes.
3. Neoplastic goitre:
- Benign adenoma (follicular adenoma)
- Malignant tumours: They are further classified as follows:
Primary:
- Well-differentiated carcinoma
- Papillary carcinoma, follicular carcinoma
- Poorly differentiated carcinoma
- Anaplastic carcinoma
- Arising from parafollicular cells
- Medullary carcinoma
- Arising from lymphatic tissue
- Non-Hodgkin’s lymphoma
Secondary (Metastasis):
- Malignant melanoma, renal cell carcinoma, breast carcinoma produce secondaries in the thyroid, due to blood spread.
Thyroiditis:
- Granulomatous thyroiditis
- Autoimmune thyroiditis
- Riedel’s thyroiditis.
Other rare causes of goitre:
- Acute bacterial thyroiditis
- Thyroid cyst
- Thyroid abscess
- Amyloid goitres
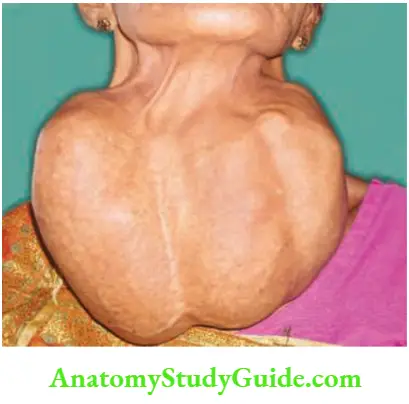
Multinodular Goitre
- A multinodular goitre is the end-stage result of diffuse hyperplastic goitre. Excessive metabolic demands cause an excessive enlargement of the thyroid. Therefore, it is common in women.
- Metabolic demands increase during puberty. A goiter appearing during that period is called puberty goitre.
- A goitre can develop during pregnancy and is called pregnancy goitre. Both of them are physiological but may eventually develop into multinodular goiter (MNG).
Describe the etiopathogenesis of thyroidal swellings.
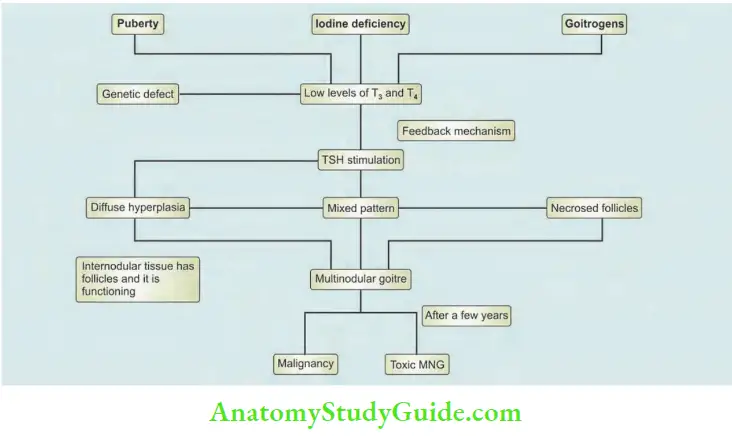
Aetiopathogenesis:
Multinodular goitre occurs due to continuous stimulation by TSH secreted from the anterior pituitary.

1. Puberty goitre, pregnancy goitre:
- It is seen in girls at puberty or during pregnancy when the metabolic demands are high and the production of T3 , T4 are comparatively normal.
- Due to feedback mechanism, TSH levels increase, which stimulates thyroid gland and causes diffuse hypertrophy and hyperplasia.
- This is also called physiological goitre and can be treated by giving tablet thyroxine (T4) 50 to 100 micrograms/day to suppress TSH.
- Goitre may disappear, if treatment is given in the stage of diffuse hypertrophy.
2. Iodine deficiency goitre:
- Daily iodine requirement is about 100–125 μg.
- Common in hilly/mountainous or low-lying areas because of decreased iodide content of water. This causes iodine deficiency goitre mediated by the same feedback mechanism.
- This is treated with iodised salt (which is used in food) and iodine—containing preparations.
- If the iodine deficiency status continues for a long time, it results in accumulation of colloid material in the gland and causes colloid goitre.
- All these three types of goitre, if left untreated, will change to multinodular goitre.
- Stage 1: Stage of diffuse hypertrophy and hyperplasia of thyroid.
- Stage 2: Due to fluctuating levels of TSH because of pregnancy, lactation, menstruation, etc. Some areas in thyroid are overstimulated and are converted to active follicles.
- Stage 3: The active follicle ultimately undergoes necrosis and many such necrosed follicles join to form a nodule. Many such nodules form a multinodular goitre. Nodules contain necrosed tissue, i.e. inactive tissue. The internodular tissue is active.
3. Goitrogens such as cabbage (contains thiocyanates), drugs such as amiodarone and sulfonamides, cause goiter by preventing oxidation of iodide to iodine. Excess iodides inhibit organic binding of iodine and produce goitre.
4. Dyshormonogenesis
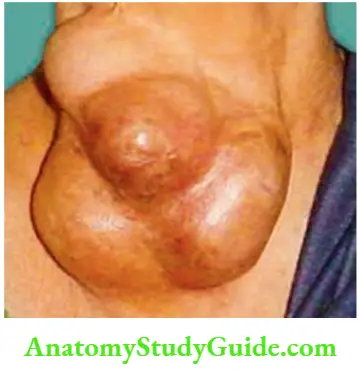
Multinodular Goitre Clinical Features:
- Common in females. Female: male ratio is 10: 1. Seen in the age group of 20–40 years.
- Long duration of swelling in front of the neck, dyspnoea due to tracheomalacia and dysphagia are the presenting features.
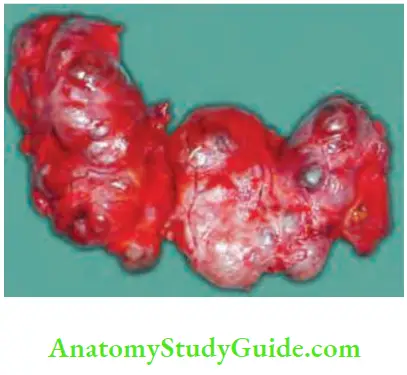
- The gland is nodular, firm in consistency and both the lobes are enlarged. Hard areas may suggest calcification and soft areas, necrosis.
- Sudden increase in size with pain is mainly due to haemorrhage in a nodule.
Complications of Multinodular Goitre:
- Calcification in long-standing MNG.
- Sudden haemorrhage in one of the nodules causes dyspnoea.
- In 10–20% of cases, patients can develop secondary thyrotoxicosis with CVS involvement. Palpitation is the predominant symptom. Toxic multinodular goitre is also called Plummer’s disease.
Tachycardia can be graded as follows—Crile’s grading:
Grade 1 – <90/min—mild
Grade 2 – 90 to 100/min—moderate
Grade 3 – >110/min—severe
4. Follicular carcinoma in a long-standing goitre 8 to 15%.
Management of Multinodular Goitre:
Investigations:
- Complete blood picture (CBP), and a few investigations for fitness including baseline ECG and echo cardiography more so in toxic goitres.
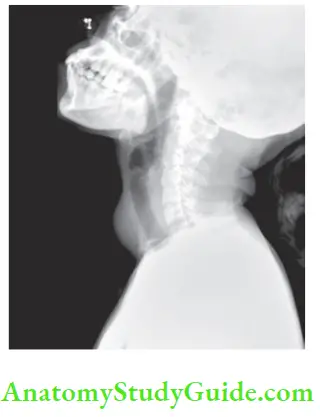
- X-ray of the neck: Anteroposterior and lateral view.
- To look for compression of trachea—to check feasibility of intubation during anaesthesia.
- To rule out retrosternal extension—soft tissue shadow seen.
- Calcification in long-standing MNG.
- Flexible laryngoscopy is done to see vocal cord mobility (this has replaced indirect laryngoscopy).
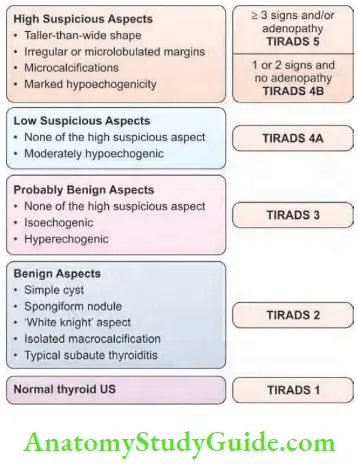
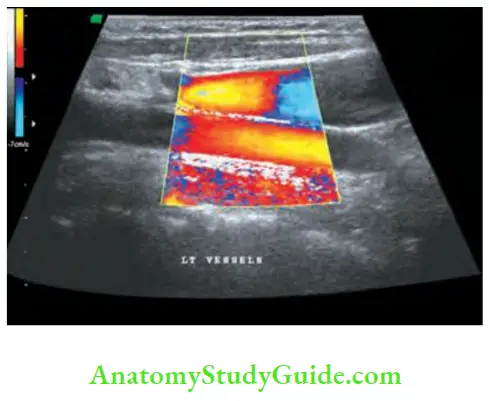
- Ultrasonography: High frequency ultrasound (7– 15 MHz) is the first investigation in thyroid swellings.
- (TIRADS—More details are given on page 417). In multinodular goitres, ultrasound guided FNAC can be done. It can also detect clinically impalpable lymph nodes in the neck (suggest malignancy).
- Like in the breast, ultrasound examination of the thyroid gland has been categorised into TIRADS—Thyroid Imaging Reporting and Data Systems. 5 categories have been identified. It is applicable in all nodules more than 1 cm or more in diameter.
- Ultrasound examination is inexpensive, easily done and has more advantages than disadvantages. Thus, it is often the first investigation in thyroid swellings (Refer to clinical notes).
Ultrasound:
- It can distinguish solid from cystic lesions.
- It can measure the size of the nodule.
- It can reveal multicentric nature of the goitre.
- It can detect lymphadenopathy and can guide FNAC.
- It can detect microcalcification—a feature of malignancy-peripheral punctate calcification in the cervical nodes.
- ↑ echogenicity means ↑ chances of tumour/malignancy.
- ↑ sonolucent means ↑ chances of cyst (benign).
5. Fine needle aspiration cytology (FNAC): It can be done in suspected hard nodule of multinodular goitre. It is a simple and useful investigation which can detect malignancy. Since the treatment of MNG is often total thyroidectomy and an ultrasonogram can also help to rule out malignancy, FNAC is done only in suspicious cases of MNG.
6. CT scan is done when you suspect retrosternal extension, doubtful resectability in cases of carotid pulses are not palpable or large lymph nodes in the neck. They may also have intrathoracic lymph nodes.
Classification of Investigations:
Investigations—Goitre:
- Simple goitres
- Routine—blood tests, chest X-ray, flexible laryngoscopy, ultrasound
- Toxic goitres
- Routine and T3 , T4 , TSH
- Malignant goitre
- Routine and CT scan of the neck—optional
- FNAC: Ultrasound-guided is a must
Clinical Notes:
- A 22-year-old lady was referred to us for a nodule in the right side of neck in the thyroid region that was moving with deglutition. She also had epigastric pain since 6 months. Clinical diagnosis of solitary thyroid nodule with hyperacidity was made. An ultrasound examination of the neck was requested and the report was a surprise. She was having a parathyroid adenoma with calcific pancreatitis and nephrocalcinosis. You know the diagnosis now—a case of hyperparathyroidism.
- We sent a case of MNG to thyroid scan. The scan detected jugular lymphadenopathy on both sides. The diagnosis changed from MNG (benign) to malignancy (papillary carcinoma because of lymph nodes). Lymph nodes were not palpable on clinical examination in this patient.
- A 21-year-old lady had a multinodular goitre with the entire gland replaced by nodules. Case was posted for a total/near total thyroidectomy. A senior experienced Professor asked one question, ‘what is the duration of this swelling?’ It was 10 years. He said postpone the surgery, and do FNAC. As per his advice, FNAC was done. FNAC report was lymphocytic thyroiditis. Surgery was cancelled. She was put on T-Eltroxin 0.1 mg, 2 tablets/day. She is on follow-up now. Gland size is reduced to 30% in the last 2 years.
Prevention of MNG:
Prevention is mainly important in endemic area and is done by supplementing iodine.
Prevention of MNG:
- Puberty goitre: 0.1 g to 0.2 mg of thyroxine.
- Iodine deficiency goitre: Use iodised salt, seafood, milk, egg, etc.
- Goitrogens: Avoid cabbage, drugs.
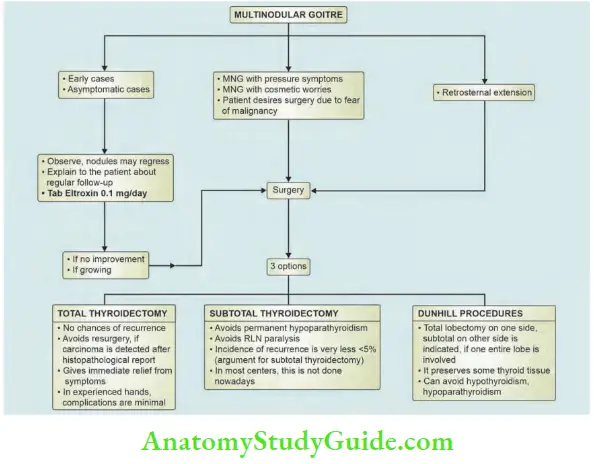
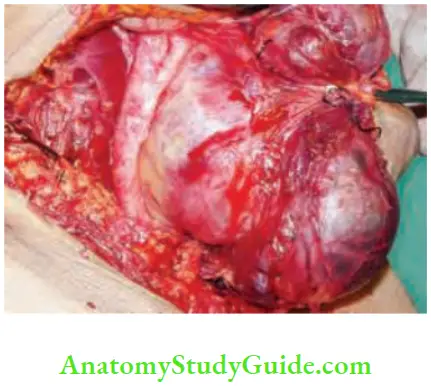
Multinodular Goitre Treatment:
Three choices are given to patients.
1. Total thyroidectomy is the choice today provided complications such as recurrent laryngeal nerve, paralysis and hypocalcaemia due to removal of parathyroid glands can be avoided. Thus, it is desirable to do a total thyroidectomy, if experience of the surgeon is good and in a high volume centre. It gives permanent quick cure to the patient.
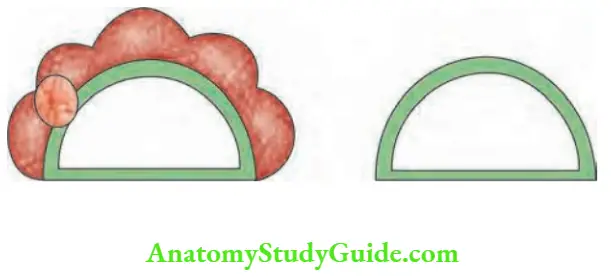
2. Subtotal thyroidectomy: In this operation, parts of right and left lobes and entire isthmus are removed in flush with tracheal surface leaving behind a small amount of tissue in the tracheoesophageal groove to protect recurrent laryngeal nerve and parathyroid gland.
Subtotal thyroidectomy is not done nowadays. Students should study first. Details of management of MNG are given.
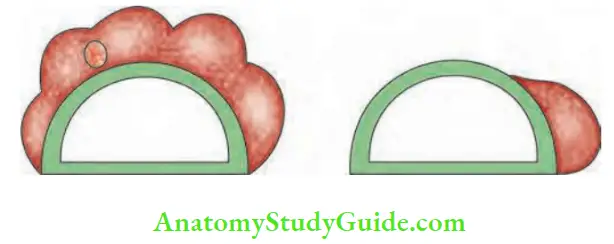
3. Dunhill procedure: In a few cases, one lobe is completely replaced with nodules and a few nodules on the other side. In such cases total lobectomy on one side and subtotal lobectomy on the other side can be done.
- Some surgeons treat these patients with 0.1 mg of thyroxine to suppress the TSH stimulation in the postoperative period, for a period of 2–5 years.
- However, it should be remembered that risk of osteoporosis, atrial fibrillation and increased morbidity and mortality from cardiovascular disease can occur. Hence, patients should be told about these complications.
Retrosternal Goitre
Retrosternal Goitre Definition:
When more than 50% of goitre is below suprasternal notch, it is called retrosternal goitre. Very often, it is a multinodular goitre that develops in the neck and is slowly pulled down behind the sternum due to the following reasons.
- Negative intrathoracic pressure
- Pretracheal muscles are strong in men
- Short neck, obesity Rarely, it arises from an ectopic thyroid tissue.
Retrosternal Goitre Classification:
- Primary: It arises from ectopic thyroid tissue in the mediastinum. It also derives blood supply from mediastinum. It is rare (1%).
- Secondary: It is the common variety—it is MNG which gets pulled down into thorax.
Retrosternal Goitre Clinical Types:
- Substernal: The most common type where the lower border of the gland is behind the sternum.
- Intrathoracic: No thyroid is seen in the neck, diagnosed by radio-iodine scan.
- Plunging goitre: When patient is asked to cough, intrathoracic pressure increases. As the thyroid plunges out, the lower border of gland is clearly seen in the neck.
Retrosternal Goitre Clinical Features:
- It can be suspected when the lower border of the swelling is not seen.
- Most of the patients have difficulty in breathing or even stridor.
- Dysphagia is more common.
- Engorgement of neck veins and superficial veins. These become more prominent when the hands are raised above the head, and the arms touch the ears with congestion and cyanosis of the face— Pemberton’s sign.
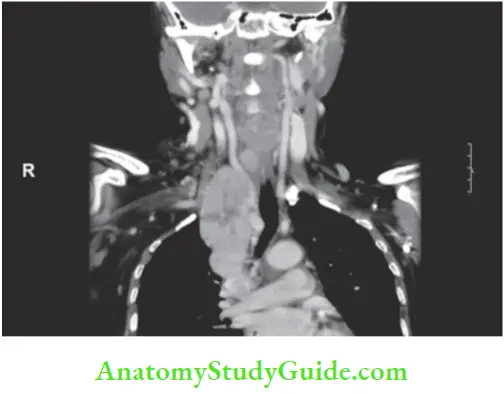
Retrosternal Goitre Investigations:
- They are similar to MNG. However, isotope scan is very useful in the diagnosis of intrathoracic goitres.
- CT scan to localise and to know the size and extent.
- CT scan classification of retrosternal goitre is important because depending upon the extent of intra-thoracic extension, treatment is planned.
Retrosternal Goitre Treatment:
- No conservative line of treatment.
- It can be easily explored through the neck incision and removed, with gentle dissection with the finger specially when the intra-thoracic part has narrow apex.
- Very rarely, a sternal split may be necessary.
Retrosternal Goitre:
- Very often, it is an MNG with the lower border unseen
- Rarely from ectopic thyroid tissue
- Severe breathlessness even though small
- Drugs should not be given, if it is toxic
- Pressure effects diagnosed by Pemberton’s sign
- Excision is the treatment
- No radioiodine therapy
Toxic Goitre—Thyrotoxicosis
It is a complex disorder which occurs due to increased levels of thyroid hormones (hyperthyroidism) and manifests clinically with various signs and symptoms involving many body systems. Following are the causes of thyrotoxicosis.
- Primary thyrotoxicosis (Graves’ disease, exophthalmic goitre, diffuse goitre).
- Secondary thyrotoxicosis: Secondary to nodular goitre (multinodular) (Plummer’s disease).
- Solitary toxic nodule: Autonomous nodule which is not under the influence of TSH but occurs due to hypertrophy and hyperplasia of gland (tertiary thyrotoxicosis).
- Other causes of thyrotoxicosis:
- Thyrotoxicosis factitia: False thyrotoxicosis occurs due to overdosage of thyroxine, given for puberty goitre.
- Jod-Basedow’s thyrotoxicosis: Jod means iodine in the German language, Basedow means toxic goitre. Iodine-induced thyrotoxicosis (iodine given for hyperplastic endemic goitres).
- Initial stage of thyroiditis: Hashimoto’s thyroiditis, viral thyroiditis can produce temporary thyrotoxicosis features.
- Very rarely, malignant goitres can be toxic (differentiated carcinoma).
- Neonatal thyrotoxicosis occurs in babies born to thyrotoxic mothers.
- TSH-secreting tumours of pituitary
- Struma ovarii
- Drugs: Amiodarone is an iodine-containing preparation given as antiarrhythmic drug.
Graves’ Disease
Also called diffuse toxic goitre.
Aetiopathogenesis:
The exact aetiological factors responsible for the disease are not clear. Following are considered as possible aetiological factors:
- Autoimmune disorder is the first possible cause due to the demonstration of autoantibodies in the circulation. Example: TSH receptor antibodies. It can be associated with other autoimmune disorders like vitiligo, type 1 diabetes mellitus, Addison’s disease, myasthenia gravis and pernicious anaemia.
- Familial/genetic: The disease can run in families. Familial/genetic Graves’ disease has been documented in identical twins.
- Graves’ disease is associated with certain HLA haplotypes, like HLA-B8, DR3, DQA1. Here a few triggering factors can result in Graves’ disease.
- HLA-DRB1*0701 is protective against Graves’ disease.
- Polymorphism of cytotoxic T lymphocyte antigen-4 (CTLA-4) is also associated with Graves’ disease.
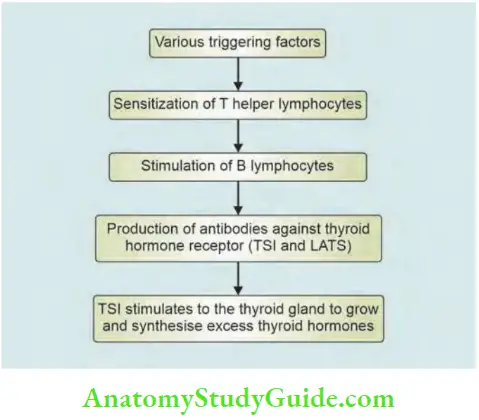
- Thyroid-stimulating immunoglobulins (TSI) and long-acting thyroid stimulator (LATS) are responsible for pathological changes in the thyroid gland in Graves’ disease. They stimulate thyrocytes to grow and synthesize excess thyroid hormones.
- Exophthalmos producing substance (EPS) is responsible for ‘ophthalmopathy’ seen in Graves’ disease.
- Female sex, emotions, stress, young age also have been considered as other factors responsible for the disease.
Triggering Factors for Graves’ Disease:
- Postpartum state
- Iodine excess
- Lithium therapy
- Infection—bacterial and viral
Graves’ Disease Pathology:
- As a result of continuous stimulation, acinar hypertrophy and hyperplasia take place. The acinar cells which are normally flat, become tall columnar.
- The normal colloid disappears and the cells are empty. However, rich vascularity is seen. Thus, small follicles with hyperplastic columnar epithelium is characteristic.
Graves’ Disease Clinical Features:
- Primary thyrotoxicosis is 8 times more common in females than in males, especially in the age group of 15–25 years.
- Thyroid swelling, features of thyrotoxicosis and exophthalmos are considered as triad of Graves’ disease. Symptoms, signs and swelling appear simultaneously.
- Very often young women present with unexplained loss of weight in spite of good appetite and insomnia is brought with diarrhoea.
- Diarrhoea occurs due to increased smooth muscle activity of small intestines. Intolerance to heat, preference to cold, fine tremors, excitability, hyperkinetic movements, excessive sweating are the other features.
- Free steroid hormone levels decrease Graves’ disease.
- This results in decreased effective oestrogen at the cell level which in turn causes oligomenorrhoea.
- Never forget to examine pulse rate specially in young patients who are losing weight unintentionally. Tachycardia is a feature.
Clinical Notes:
- Following are three case reports which highlight the clinical symptomatology of primary thyrotoxicosis.
- An 18-year-old girl visited many doctors for her complaint of loss of weight. She was investigated for tuberculosis (common disease in India), malignancy, etc.
- She was given unnecessary tonics. After nearly 6 months, when eye-signs started developing, it was proved to be Graves’ disease.
- A bank clerk’s only complaint was that he could not sign the cheque because of excessive sweating.
- Thyroid gland was not palpable. His pulse rate was very high, investigations revealed that it was a case of primary thyrotoxicosis. On careful questioning, he admitted that he was a “nervous character”.
- A 24-year-old lady was being asked by her friends every day why her eyes were prominent. Her only complaint was prominent eyes.
- On careful questioning, she admitted having anxiety, tension, excitability.
Signs of Primary Thyrotoxicosis
1. Signs of Thyroid Gland in Graves’ Disease
- Uniformly enlarged (mild degree)
- Smooth surface—no nodules (treated cases may have nodularity)
- Gland is soft or firm in consistency.
- It is warm—highly vascular and can be pulsatile
- Auscultation—a bruit can be heard.
2. Central Nervous System (CNS) Signs:
- Tremors of the tongue when the tongue is within the oral cavity and tremors of the outstretched hands are characteristics.
- A piece of paper may be placed on the fingers in doubtful cases for demonstrating the tremors of the hand. Extensor surface of the hand is used because extensors are weak when compared to flexors.
- Hyperkinetic movements
- Always a moist, warm hand (shake hands with the patient).
3. Cardiovascular System (CVS) Signs:
- Pulse rate is always raised and rapid indicating tachycardia. Depending upon the pulse rate, thyrotoxicosis can be classified as follows: Mild—90– 100/min, moderate—100–110/min, severe—more than 110/min.
- Palpitation and extrasystoles can also be found in primary thyrotoxicosis even though other cardiac features, such as fibrillation and cardiac failure, are rare.
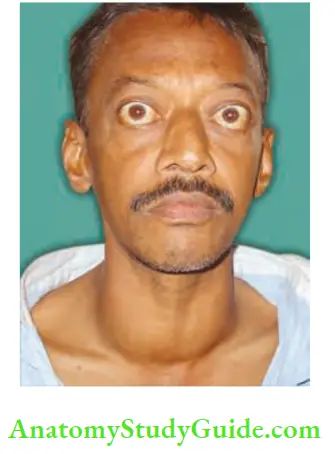
4. Eye Signs:
- Prominent eyeballs and retraction of the eyelid result in thyrotoxic exophthalmos. This is due to retrobulbar deposition of inflammatory cells and round cells with venous congestion resulting in oedema.

- Levator palpebrae superioris muscle is innervated by oculomotor nerve which also carries sympathetic fibres derived from cavernous plexus for the smooth muscle part of the levator. Contraction of this muscle produces lid spasm.
- This is aided by spasm of Müller’s muscle, a sympathetic muscle which lies adjoining the levator palpebrae superioris muscle. This is responsible for keeping the eyeball forward. All these factors together produce a classical stare.
- Assessment of exophthalmos:
- Upper sclera is seen above the limbus (upper margin of the cornea and conjunctiva—Dalrymple’s sign.
- Naffziger’s method: Stand behind the patient and look at the supraciliary arch, by tilting the patient’s head backwards. In normal cases, eyeball is not seen. In cases of exophthalmos, eyeball is protruded outside and hence it is seen.
- Moebius’ sign: Loss of convergence of eyeball occurs due to muscle paresis as a part of thyrotoxic ophthalmoplegia. Diplopia is due to weakness of extraocular muscles (inferior oblique-elevators).
- Stellwag’s sign: Infrequent blinking and widening of palpebral fissure is due to spasm of sympathetic fibres in the levator palpebrae superioris.
- Joffroy’s sign: Absence of wrinkling of the forehead when the patient is asked to look upwards. This occurs due to increase in the field of vision due to exophthalmos.
- von Graefe’s sign (lid-lag sign): When the patient is asked to look up and down, upper eyelid cannot cope up with the speed of movement of the finger because of the lid spasm. Hence, the lid lags behind.
- Enroth sign: Oedema of eyelids and conjunctiva.
- Gifford’s sign: Difficulty in everting the upper eyelid.
- Kocher’s sign: When an attempt is made to lift the eyes higher, upper eyelid springs up more quickly than the eyebrows.
Thyrotoxic Exophthalmos:
- Proptosis and lid retraction result in exophthalmos
- Sclera is visible beyond limbus
- Naffziger’s method to examine
- Staring look
- Typically seen in Graves’ disease
- Rarely seen in secondary thyrotoxicosis
Interesting 6 Ps of Graves’ Ophthalmopathy:
- Prominent eyes
- Periorbital oedema
- Papilloedema
- Proptosis
- Palpebral fissure widening
- Progression to blindness
Symptoms of thyrotoxicosis:
Grading of Thyroid Eye Diseases:
- Grade 0 No signs or symptoms
- Grade 1 Only signs, no symptoms
- Grade 2 Both signs and symptoms
- Grade 3 Proptosis
- Grade 4 Extraocular muscle involvement
- Grade 5 Corneal involvement
- Grade 6 Loss of vision with optic nerve atrophy
Malignant Exophthalmos:
- This occurs in untreated cases of Graves’ disease.
- If the disease continues, infrequent blinking secondary to exophthalmos results in constant exposure of the cornea to the atmosphere.
- This results in keratitis, corneal ulcer, conjunctivitis, chemosis and may even lead to blindness. This is called malignant exophthalmos.
- Malignant exophthalmos is probably due to autoimmune disease.
- In late stages, optic nerve damage and blindness can occur.
Treatment of thyrotoxic ophthalmopathy:
- Massive doses of steroids—methylprednisolone and metronidazole
- Lateral tarsorrhaphy
- Orbital decompression may be necessary in late cases.
- Guanethidine eyedrops are useful to decrease lid spasm and lid retraction.
- Head end elevation and disease control.
- Dark spectacles, 7% methylcellulose eye drops.
Important causes of exophthalmos:
- Thyrotoxicosis
- Primary CNS tumours: Meningioma, optic nerve glioma, haemangioma, lymphoma, etc.
- Metastatic tumours: Neuroblastoma, central carcinoma.
- Vascular: Cavernous sinus thrombosis—aneurysm of ophthalmic artery.
Causes of pulsating exophthalmos:
- Cavernous sinus thrombosis
- Carotid—cavernous sinus, A-V fistula
- Orbital vascular tumour
- Ophthalmic artery aneurysm
Thyrotoxic Myopathy:
- Mild weakness of proximal limb muscles, ocular and frontalis muscles is not uncommon. On careful questioning, patient may admit difficulty in climbing steps.
- Weakness of extraocular muscles results in double vision (diplopia).
- Features suggestive of myasthenia gravis, periodic paralysis can be found.
- Myopathy improves with treatment.
Thyrotoxic Dermopathy:
- Popularly called pretibial myxoedema—is seen in thyrotoxicosis patients treated with surgery or antithyroid drugs. It is always associated with exophthalmos. It is seen in 1–2% of patients.
- Bilateral symmetrical deposition of myxomatous tissue (glycosaminoglycans) mainly in the pretibial region, may also affect the foot and ankle, sometimes the entire leg below knee.
- Skin is dry and coarse (thickening of skin by mucin—like deposits). Swelling is due to the obliteration of initial lymphatics by mucin.
- Pretibial myxoedema (misnomer) is nonpitting in nature and may be associated with clubbing of fingers and toes called thyroid acropachy. Responds to topical steroids and thyroid disorder treatment.
- Interestingly following 4 important features are seen only in primary thyrotoxicosis, not in secondary thyrotoxicosis.
Skin Changes:
- Pretibial myxoedema
- Pruritis
- Palmar erythema
- Thinning of hair
- Dupuytren’s contracture
Pretibial Myxoedema—Misnomer:
- Acropachy—clubbing of fingers and toes
- Coarse hair
- Red shiny skin
- Obliteration of initial lymphatics by mucin, oedema non-pitting
- Pretibial region, foot and ankle
- After a few years of toxicosis, it develops
- Cyanotic when cold
- H Hyaluronic acid deposition in dermis
- Y Bilateral and symmetrical Remember as ACROPACHY
Some Misnomers:
- Pretibial myxoedema – Not seen in myxoedema
- Mycosis fungoides – Not a fungal infection
- White bile – Not white, not bile
- Adenolymphoma – Not a lymphoma
- Sternomastoid tumour – Not a tumour
- Malignant hydatid – Not malignant
Extrathyroidal Manifestations of Graves’ Disease:
- Pretibial myxoedema
- Proximal myopathy
- Pachy (acropachy)
- Progressive ophthalmoplegia
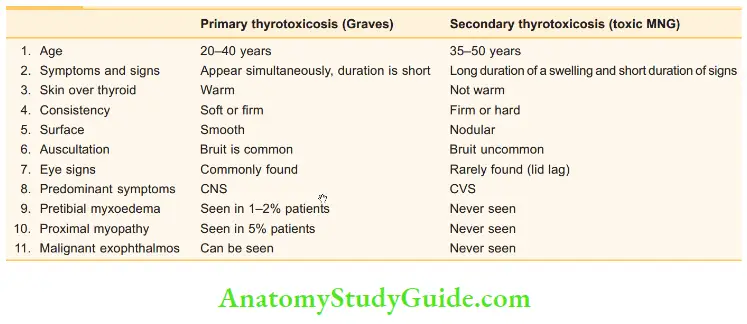
At the end of clinical examination, commonly asked question is, how will you differentiate primary thyrotoxicosis from secondary thyrotoxicosis.
Management of Primary Thyrotoxicosis:
Routine isotope scanning has been abandoned in toxic goitres except when toxicity is associated with nodularity.
Investigations:
- Routine investigations such as complete blood picture, flexible laryngoscopy and X rays are done.
- Serum T3 , T4 and TSH are measured. T3 or T4 levels are high and TSH levels are low in thyrotoxicosis. The normal level of T3 is 1.3–3.5 nmol/L and normal level of T 4 is 55–150 nmol/L.
- Thyroid stimulating antibodies are elevated (TSHRAbs). Measurement of IgG immunoglobulins (TSHRAbs) is not essential to make the diagnosis of thyrotoxicosis.
- As a first-line investigation, ultrasound is done to rule out nodularity (seconadry thyrotoxicosis).
Treatment of Primary Thyrotoxicosis:
Aim of treatment:
- To restore patient to euthyroid state
- To reduce the functioning thyroid mass to a very critical level (about 6–8 g of thyroid tissue)
- To minimise complications
1. To Restore the Patient to Euthyroid State:
- Other drugs such as potassium perchlorate are given in the dose of 200 to 400 mg daily. Propylthiouracil in the dose of 200 mg three times a day can also be given in patients who develop neutropaenia due to carbimazole.
- Propranolol inhibits peripheral conversion of T4 to T3 . This results in rapid control of tachycardia and surgery can be scheduled in a few days (within one week). It should be continued for one week after surgery because it does not interfere with synthesis of hormones.
Please note:
- Iodine containing antiarrhythmic drug amiodarone may worsen thyrotoxicosis.
- Propyl thiouracil is safe in pregnancy with Graves’ disease.
- Role of Lugol’s iodine is doubtful.
- Antithyroid drugs will not cure the disease. In selected patients (30–40%), remission is possible with regular intake of drugs.
- They may be continued for a maximum period of 2 years. If toxicity persists or recurs on stopping drugs, surgery is recommended.+ However, majority of the patients ultimately require surgery or radioiodine.
Differences between primary and secondary thyrotoxicosis:
Antithyroid drugs: Routine preoperative preparation:
Corticosteroids:
- They can be used as reserve drugs in severe, uncontrolled or resistant hyperthyroidism cases.
- They act by two ways—one by suppressing pituitary thyroid axis and another by inhibiting peripheral conversion of T4 to T3 .
- Action is rapid
- They are used along with other antithyroid drugs.
Block and replace treatment:
- If a small dose of T3 (20 mg up to 4 times/day) or T4 (0.1 mg/day) is given along with antithyroid drugs, there is less incidence of development of hypothyroidism and increase in the size of goitre.
2. To Reduce the Functioning Thyroid Mass:
- Total thyroidectomy can be offered to young patients with a small-sized gland. This is the choice of treatment today. It controls the toxicity very faster. Hypothyroidism occurs but it is easy to treat. However, it should be done by an experienced surgeon.
- Radioiodine therapy: This is a suitable alternative to surgery in cases of primary thyrotoxicosis in patients above the age of 30.
3. To Minimise Complications:
- Good preoperative preparation of the patient, good anaesthetic and surgical techniques, and good post operative care will reduce the complications of surgery.
- Thus, antithyroid drugs, subtotal thyroidectomy and radioiodine therapy are the three different modalities available for the treatment of primary thyrotoxicosis.
- The indications, merits and demerits of each treatment are given.
Radioiodine Therapy:
- Today there is ‘no restriction of age and gender’. (However, this is preferred in children only after completion of growth and in adults only after family is complete.)
- Absolute contraindication is pregnancy.
- Conception must be avoided for a period of 4 months after radioiodine therapy.
Treatment of Secondary Thyrotoxicosis (Plummer Disease):
- Patients with severe cardiac damage entirely or partly due to hyperthyroidism are middle-aged or elderly with secondary thyrotoxicosis and the hyperthyroidism is not very severe. These patients develop atrial fibrillation and cardiac failure if left untreated.
- In elderly patients, when the operative risk is unacceptable, radioiodine is given. Treatment with antithyroid drugs is started 48 hours later and continued until radioiodine has had its effect (6 weeks).
- If the cardiac symptoms are controlled well and anaesthesia risk is acceptable, subtotal thyroidectomy/total thyroidectomy is done. However, the gland that is left behind should be equal to the distal phalanx of the thumb of the patient.
Secondary Thyrotoxicosis Effects on CVS:
- Tachycardia
- Wide pulse pressure
- Systolic scratch (Means-Lerman scratch)*
- Extrasystoles
- Atrial fibrillation
- Cardiac failure
Solitary Toxic Nodule
Solitary Toxic Nodule Treatment:
- This is not under control of TSH. It is an autonomous nodule.
- The control of toxicity is in the usual manner— carbimazole and propranolol.
- This is an indication to do I131 scan or preferably 99mTc scan. Hot nodule takes up isotope (also in carcinoma). Rest of the gland does not.
- Treatment is either by hemithyroidectomy or radioactive iodine therapy—I131 (details will be given later).
- More details about solitary thyroid nodule and how to evaluate has been given later.
A Few Specific Thyroid Conditions Causing Thyrotoxicosis:
- Thyrotoxicosis in children: Initially antithyroid drugs are given for 10–15 years followed by surgery.
- Radioiodine is absolutely contraindicated as there is a fear of carcinoma and growth retardation.
- Thyrocardiac: It refers to a condition wherein cardiac damage has resulted due to hyperthyroidism.
- Classically, it happens in secondary thyrotoxicosis.
- It is usually seen in middle-aged or old-aged patients. Propranolol controls the disease very well. Radioiodine therapy is the treatment of choice.
- Hyperthyroidism in pregnancy: Invariably, it occurs in Graves’ disease. In the first trimester, surgery and radioiodine are contraindicated. Carbimazole and propylthiouracil cross the placenta. Surgery, if necessary, can be done in 2nd trimester.
- Apathetic thyrotoxicosis: Thyrotoxicosis in elderly wherein pulse rate is low, they appear to be hypothyroid rather than hyperthyroid. Thyroid gland is rarely palpable. Lethargy and behaviour changes.
- Graves’ disease in postpartum period: Postpartum thyroiditis with transient thyrotoxicosis due to thyroid cell dysfunction may occur in 5 to 10% patients during the first 4 to 12 months after delivery.
- Struma ovarii: Thyroid tissue is present in 5 to 10% of teratomas and occasionally such foci are hyper functional.
- About 5–10% of these tumours are bilateral and thyrotoxicosis may occur in 8 to 10% of patients. Patients present with variable degree of thyrotoxicosis and have lower abdominal pain or mass.
- Treatment—patient to be rendered euthyroid followed by removal of involved ovary. Therapeutic radioiodine may be required for metastatic disease.
- Trophoblastic thyrotoxicosis: HCG secreted by vesicular mole, choriocarcinoma or metastatic embryonal carcinoma act like TsAb causing thyrotoxicosis.
- Hamburger thyrotoxicosis: It is an unusual and rare form of epidemic exogenic thyrotoxicosis. One such incidence was reported in United States in 1984–85 due to inclusion of large quantities of bovine thyroid in beef preparations.
Neoplastic Goitre
Adenoma:
- The benign tumours of the thyroid gland are not uncommon. They present as a solitary nodule, thus causing a worry to the clinician. Adenomas are of follicular type.
- The diagnosis is established by histological examination.
- Adenomas are treated by hemithyroidectomy/ lobectomy.
- However, FNAC cannot distinguish between a follicular adenoma and follicular carcinoma. Hence, a frozen section can be done.
Describe the clinical features, classification and principles of management of thyroid cancer.
Malignant Tumours
- Thyroid is the only endocrine gland wherein malignant tumours are easily accessible to clinical examination.
- Thyroid is the only endocrine gland wherein malignant tumours occur in children, young age, middle age, old age, and in both sexes.
- Thyroid is the only endocrine gland wherein malignant tumours spread by all possible routes—local, lymphatic and blood spread.
- Thyroid is the only endocrine gland wherein malignant tumours are usually nonfunctional. Malignant tumours of the thyroid are common.
- They are interesting tumours, having good prognosis, if diagnosed early.
- Papillary and follicular carcinomas are well differentiated, medullary carcinoma is poorly differentiated.
Papillary Carcinoma Thyroid (Pct)
Thyroid Oncogenesis:
- Mutations in oncogenesis will result in malignancies.
- In case of thyroid, rearrangement of RET (rearranged during transfection) and NTRKI tyrosine kinase result in sporadic papillary carcinoma (neurotrophic receptor, tyrosine kinase receptor)
- Specially in papillary carcinoma thyroid RET protooncogene is predominantly found in malignant tissue.
- RAS, kinase and 13 type (BRAF) are result of downstream pathway of RET and NTRKI mutations. BRAF mutations can result in poorly differentiated cancer.
- 40% of thyroid tumour including follicular adenoma will have RAS gene point mutations.
- K-RAS mutations more often found in radiation induced-papillary thyroid carcinomas
- Radiation damages p53 tumour suppressive gene. p53 gene plays an important role in cell cycle progression. p53 gene has been found in anaplastic thyroid cancer.
Radiation and Thyroid Cancer:
- Neoplastic nodules are much more common when thyroid gland is exposed to long-term ionising radiation.
- High amount of radiation causes increased incidence of thyroid cancers.
- Risk of cancers in adults is high when they had contacted low or moderate doses of irradiation during childhood as found in survivors of Hiroshima and Nagasaki.
- Generally after 5 years of radiation exposure (radiation to head and neck for childhood lymphoma or too many CT scans for head and neck malignancy), papillary carcinoma thyroid can occur.
Aetiology:
- Irradiation to the neck during childhood: In olden days, radiotherapy was given for benign conditions such as acne in teenagers or enlarged tonsils or thymus gland. Those children had increased risk ofpapillary carcinoma thyroid.
- These indications are obsolete now. However, accidental radiation to the neck or radiation given to Hodgkin’s lymphoma can precipitate the development of papillary carcinoma thyroid.
- It can be a complication of Hashimoto’s thyroiditis.
- Papillary cancer of thyroid occurs more often in patients with Cowden’s syndrome, Gardner’s syndrome or Carney’s syndrome.
- Associated mutations: Chromosomal translocation involving RET proto-oncogene (tyrosine kinase) chromosome 10q11.
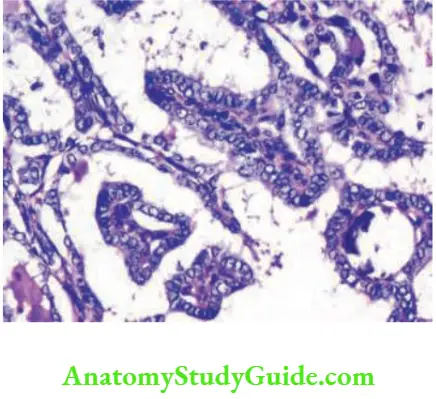
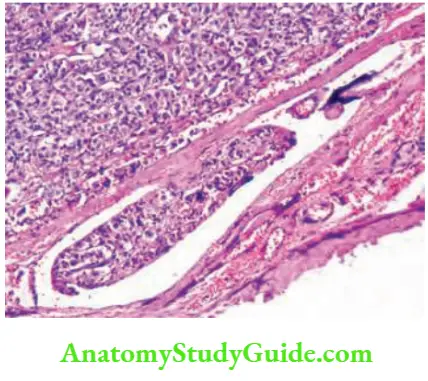
Pathology:
- It is made up of colloid-filled follicles with papillary projections. In some cases, concentric, lamellated calcific structures are found which are called psammoma bodies. (Psammoma bodies are also found in meningioma, and papillary serous cystadenoma of the ovary.) These are suggestive of papillary carcinoma of thyroid.
- Nuclear grooving and intranuclear cytoplasmic inclusion (INCI) are diagnostic of papillary carcinoma thyroid.
- Characteristic pale, empty, nuclei are present in a few cases which are described as Orphan Annie-eye nuclei.
- Thyroid gland has very rich intrathyroidal lymphatic plexus. Papillary carcinoma can be unifocal or multifocal.
- Papillary microcarcinoma: They measure 1 cm or less in diameter. Distant metastasis is extremely rare. Hence, a simple hemithyroidectomy is the treatment of choice.
- Follicular variant of papillary cancer: This is a mixed lesion with a predominance of follicles over papillae. These are treated by total thyroidectomy. It is called Lindsay tumour.
- Tall cell papillary cancer: This is an aggressive and rapidly growing tumour. It occurs in elderly patients and should be treated by total thyroidectomy.
- Other details are given.
Pathology of Papillary Carcinoma Microscopy:
- Calcification
- Cystic changes/necrosis
- Cuboidal pale cell with grooving
- Crowded nuclei
- Cytoplasmic inclusions—intranuclear
- Cartoon character—Orphan Annie
- Calcified laminated, basophilic, spherical concretions— Psammoma bodies Observe 7 Cs
Types—Woolner classification:
- Minimal/occult/microcarcinoma: Tumour of 1 cm or less in size with no invasion/no lymph node metastasis
- Intrathyroidal: Confined to thyroid gland
- Extrathyroidal: Invasion of adjacent structures.
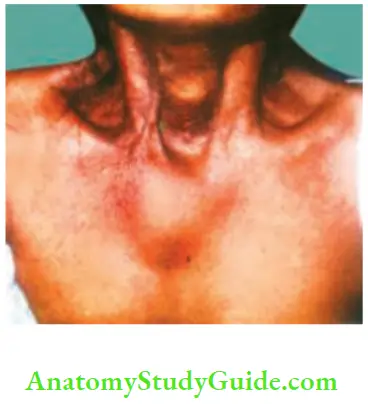
Papillary Carcinoma Thyroid Clinical Presentation:
- As solitary nodule: Young females are commonly affected (in the age of 20–40 years). It can present as a solitary nodule Nodule can be firm or hard.
- Unlike a nodule of anaplastic malignancy, nodule of papillary carcinoma is usually mobile in vast majority of cases.
- However, when it occurs in elderly patients, it can be rapidly growing. Ulceration and fungation is rare but can occur only in neglected cases.
- As enlarged lymph node: Very often, the lymph nodes in the lower deep cervical region—level 3 and level 4 are involved and they can be huge size.
- As occult primary with palpable nodes: In these cases thyroid gland may or may not be palpable. When thyroid gland is not palpable, it is called occult (hidden). However, papillary carcinoma less than 1.5 cm in diameter is also called ‘occult’.
- Interestingly a few patients present as lateral aberrant thyroid or even a cystic swelling which is misdiagnosed as even a lymphatic cyst.
- Tracheal fixity, common carotid artery engulfment and recurrent laryngeal nerve infiltration are very uncommon features of papillary carcinoma thyroid. But can occur in advanced cases more so in elderly patients.

Papillary Carcinoma—Lymph Node Metastasis—Peculiarities:
- They may be palpable even when thyroid gland is not palpable—occult primary
- Very slow growing
- Very often, they are intracapsular
- They need not be hard, are often cystic and firm in consistency
- At operation, they are bluish in colour because of rupture of the papillae
- Presence of lymph node metastasis does not affect the prognosis
- Mostly central neck nodes and jugular chain of lymph nodes are cleared. Dissection of posterior triangle and suprahyoid dissection is not necessary.
Prognostic Criteria:
There are many prognostic criteria that have been used in cases of well-differentiated carcinoma. Various scoring systems are available for well-differentiated carcinomas. Some examples are given below.
AMES scoring:
A: Age less than 40 years—better prognosis
M: Distant metastasis—poor prognosis
E: Extent of tumour extracapsular spread—poor prognosis
S: Size less than 4 cm, good prognosis
AGES scoring
A: Age less than 40 years—better prognosis
G: Grade of the tumour—high grade—poor prognosis
E: Extracapsular spread—poor prognosis
S: Size less than 4 cm—good prognosis
MACIS scoring
M: Metastasis
A: Age
C: Completeness of resection
I: Invasion
S: Size
Histological Surprise:
- If a patient undergoes hemithyroidectomy for suspicious adenoma and histopathology reported is papillary carcinoma, dilemma exists as to how to proceed. Straightaway, one can advise the patient for completion (total) thyroidectomy.
- According to another school of thought, if the patient is in low-risk category with intrathyroidal malignancy and other factors favoring good prognosis, then ‘wait and watch’ policy can be undertaken.
Investigations:
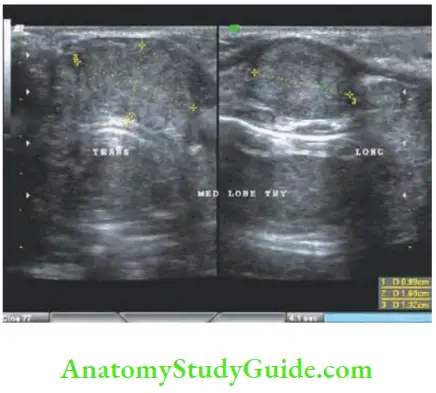
- Ultrasound imaging and image guided FNAC: It is the first investigation of choice. As in breast imaging (BIRADS) in thyroid diseases also various findings have been classified depending upon composition, echogenecity, shape, margin and echogenic focus.
- Imaging by ultrasound has been described as TIRADS. Hypoechoic lesion with solid components, taller than wide, richly vascular/microcalcification and with or without jugular lymphadenopathy are suggestive of malignancy.
- In all such cases, ultrasound guided FNAC is done. Intranuclear inclusion bodies and nuclear grooving confirm diagnosis of papillary carcinoma thyroid.
Image-guided FNAC:
Hemithyroidectomy (if done for solitary nodule) may reveal histological surprise with orphan Annie eyed nuclear and psammoma bodies (calcified clumps of cells with the papillary projections).
CECT scan: It is routinely not done. Indications are: Advanced lesions to know the distorted anatomy of neck, infiltration into carotid sheath, retrosternal extension/doubtful fixity.
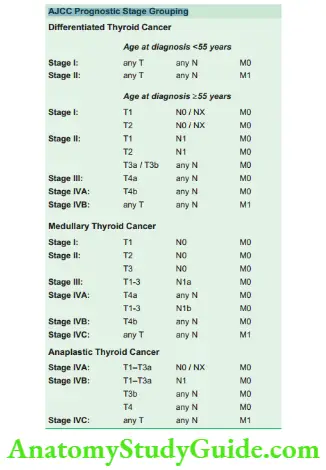
Staging Ajcc, 8th edition, 2018, TNM definitions
Primary tumour (pT) for papillary, follicular, poorly differentiated, Hürthle cell and anaplastic thyroid carcinomas:
- TX: Primary tumour cannot be assessed
- T0: No evidence of primary tumour
- T1: Tumour <2 cm in greatest dimension limited to the thyroid
- T2: Tumour >2 cm but <4 cm in greatest dimension limited to the thyroid
- T3: Tumour >4 cm limited to the thyroid or gross extrathyroidal extension invading only strap muscles
- T3a: Tumour >4 cm limited to the thyroid
- T3b: Gross extrathyroidal extension invading only strap muscles (sternohyoid, sternothyroid, thyrohyoid or omohyoid muscles) from a tumour of any size
- T4: Includes gross extrathyroidal extension into major neck structures
- T4a: Gross extrathyroidal extension invading subcutaneous soft tissues, larynx, trachea, oesophagus or recurrent laryngeal nerve from a tumour of any size
- T4b: Gross extrathyroidal extension invading prevertebral fascia or encasing carotid artery or mediastinal vessels from a tumour of any size
Primary tumour (pT) for medullary thyroid carcinomas:
- TX–T3: Definitions are similar to the above
- T4: Advanced disease
- T4b: G
- T4a: Moderately advanced disease; tumour of any size with gross extrathyroidal extension into the nearby tissues of the neck, including subcutaneous soft tissue, larynx, trachea, oesophagus or recurrent laryngeal nerve
- T4b: Very advanced disease; tumour of any size with extension toward the spine or into nearby large blood vessels, invading the prevertebral fascia or encasing the carotid artery or mediastinal vessels
Regional Lymph Node (pN):
- NX: Regional lymph nodes cannot be assessed
- N0: No evidence of regional lymph node metastasis
- N1: Metastasis to regional nodes
- N1a: Metastasis to level 6 or 7 (pretracheal, paratracheal, prelaryngeal/Delphian or upper mediastinal) lymph nodes; this can be unilateral or bilateral disease
- N1b: Metastasis to unilateral, bilateral or contralateral lateral neck lymph nodes (levels 1, 2, 3, 4 or 5) or retropharyngeal lymph nodes
Distant Metastasis (M):
- M0: No distant metastasis
- M1: Distant metastasis
Aims or Goals of Treatment of Papillary Carcinoma Thyroid:
- Excise primary tumour → Total thyroidectomy
- Remove clinically significant/palpable lymph node → Functional neck dissection (no prophylactic neck dissection)
- Minimal complications of surgery—preserve internal jugular vein, accessory nerve.
- Once surgery is done—stage the disease
- Postoperative radioablation for residual thyroid tissue (usually it is present).
- Long-term follow-up with ultrasound of the neck and thyroglobulin for recurrence.
- Postoperative supplementary and suppressive dose of thyroxine.
- Look for metastasis.
Papillary Carcinoma Thyroid Treatment:
It can be discussed under three headings. Treatment of the primary, treatment of the secondaries in the lymph nodes and suppression of TSH.
Treatment of the Primary: Papillary Carcinoma Thyroid without Lymph Nodes. Stage 1:
- Total thyroidectomy,
- Lobectomy and
- Radioremnant ablation.
Indications for total thyroidectomy:
- Age older than 45 years
- Contralateral nodules
- Prior irradiation
- Familial—differentiated thyroid carcinoma (DTC)
- DTC >1 cm in size
- Extra thyroidal extension
- Regional/local metastasis
1. Total thyroidectomy is the treatment of choice. It means removal of the entire thyroid gland. No role for prophylactic lymph node dissection of central compartmental nodes—level 6.
Papillary Carcinoma Thyroid Advantages:
- Easy to detect and treat residual or metastatic disease—Dose of radioiodine 30–100 mCi.
- Easy to assess recurrence by thyroglobulin level estimation.
- Eliminates contralateral occult cancer (multifocal in 80% patients).
- Eliminates re-surgery.
- Eliminates risk of recurrence, thus improving survival.
- TSH suppression can be done.
Papillary Carcinoma Thyroid Disadvantages:
- Total thyroidectomy has high complication rates such as RLN paralysis, permanent hypothyroidism, permanent hypoparathyroidism, etc.
- Recurrence in opposite lobe is only 5% which means in 95% of the cases, removal of the opposite lobe is unnecessary.
- Even if it occurs later, since it is not dissected at the time of initial surgery, the lobe can be removed easily.
- Tumour multicentricity has a little prognostic significance. Thus in a few selected cases, lobectomy can be done.
2. Lobectomy (hemithyroidectomy) means removal of one lobe and entire isthmus.
Indications for lobectomy:
- Papillary carcinoma thyroid (PCT) less than 1 cm (called microcarcinoma)—no clinically palpable nodes, no extrathyroid extensions.
Advantages of lobectomy:
- No hormone replacement
- No hypoparathyroidism
- Need not test thyroid function regularly.
Treatment of Papillary Carcinoma Thyroid with Secondaries in the Lymph Nodes:
- This is therapeutic not prophylactic lymph nodes dissections. At surgery, one has to carefully look for central compartment nodes—for enlargement. If palpable and enlarged, they should be removed.
- If nodes are enlarged in the anterior triangle, they are dissected and removed en bloc along with fat and fascia. This is called functional block dissection (Berry picking means removal of enlarged lymph nodes only. It is no longer followed).
- Level 2, 3, 4 and 5 nodes are removed when they are enlarged.
- Structures, such as internal jugular vein, sternomastoid muscle, accessory nerve are not removed because lymph nodes are slow growing and they rarely spread/outside the capsule of the lymph node.
- However, in exceptional cases of papillary carcinoma with infiltration to these structures, there should not be hesitation to remove these structures, this is called lateral neck dissection. In children, prophylactic/ direct lymph node dissection is done.
3. Radio remnant ablation: After surgery, thyroxine is not given for a period of 4 weeks. Patient should be hypothyroid and TSH is around 30 mU/L.
- At this stage, radioisotope scan is done to look for residual thyroid gland. Even after total thyroidectomy, it is possible that some part of thyroid tissue may be present near the trachea esophageal groove or Berry ligament area. This needs to be ablated with 50 to 150 mCi of radioiodine.
- To avoid hypothyroidism for 4 weeks, patients can be given T3 because it acts quickly and it can be stopped and restarted quickly. Dose of T3 is 40–60 mg/day. It is very costly; not freely available.

Suppression of the TSH:
- This is an important aspect in the postoperative period because papillary carcinoma is a TSH dependent tumour. To prevent the patient developing hypothyroidism in the postoperative period and to suppress TSH, thyrotoxine (T4) 100 to 200 micrograms are given. This need to be monitored—increase or decrease depending upon the levels of TSH and toxicity.
- Failure of suppression of TSH to a level <0.1 mU/L suggests inadequate dose of thyroxine or noncompliance. Summary of papillary carcinoma thyroid.
Summary of Papillary Carcinoma Thyroid:
- Most common histological type of thyroid cancer (60 to 65%).
- Most often it is multifocal (80%).
- Commonly it spreads by lymphatic spread.
- Psammoma bodies are suggestive and nuclear grooving is diagnostic of papillary carcinoma of thyroid.
- Most often it presents as solitary nodule and with or without lymph node metastasis.
- Most commonly done procedure for papillary carcinoma thyroid is total thyroidectomy with or without functional neck dissection.
- Radioactive iodine ablation and thyroxine 0.2 mg are important post-operative.
- Most of the patients (>95%) have 10-year survival rate.
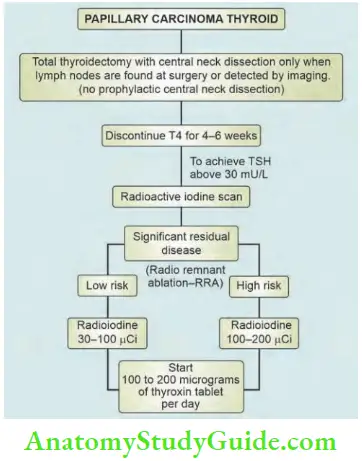
Management Protocol of Papillary Carcinoma of the Thyroid:
Depicts management protocol of papillary carcinoma of the thyroid.
Follicular Carcinoma
- Incidence: Constitutes 17% of cases.
- Follicular adenoma 20% are malignant and 80% are benign.
Follicular Carcinoma Aetiology:
Follicular carcinoma usually arises in a multinodular goitre, especially in cases of endemic goitre. It should be suspected when MNG starts growing rapidly.
Incidence of Thyroid Malignancy:
- Papillary carcinoma – 60–65%
- Follicular carcinoma – 15–20%
- Anaplastic carcinoma – 10–12%
- Medullary carcinoma – 5–10%
- Others – 10%

Pathology:
Depending upon the property of invasion, it is classified into:
- Non-invasive which means minimal invasion.
- Invasive refers to angioinvasion and capsular invasion, necessary for the diagnosis of follicular carcinoma of thyroid. The tumour cells line the blood vessels and get dislodged into the systemic circulation producing secondaries in the bones. Microscopically, most of the tumours are well encapsulated.
Follicular Carcinoma Clinical Presentation:
- It can present as a solitary nodule. The diagnosis is considered only after an ultrasound scan reveals some features of malignancy, such as microcalcification. Peak age group is around 40 years.
- In case of long-standing multinodular goitres, if the goitre is rapidly growing, hard or has restricted mobility, follicular carcinoma can be considered.
- Metastasis in the flat bones: The only clinical situation wherein a follicular carcinoma can be considered as the diagnosis is when a patient with a thyroid swelling presents with metastasis in the bone in the form of bony swelling or pathological fractures.
- Commonly, secondaries develop in the flat bones such as skull, ribs, sternum, vertebral column because the flat bones retain red marrow for a longer time.
- When bony swelling is obvious and thyroid is not palpable clinically, it is called occult primary site.
- The clinical features of secondary in the skull are:
- They are rapidly growing.
- They are warm.

-
- Vascular and pulsatile
- Underlying bony erosion may be present.


Reasons why Bone Metastasis Grow Rapidly from Follicular Carcinoma Thyroid—Seed and Soil Hypothesis:
- Tumour cells secrete angiogenesis compounds
- Tumour cells secrete factors which enhance bone resorption
- Increase production of IL-1, IL-6 which increase osteolytic activity
- Maliganant cells synthesise adhesive molecules because of which they get attached to bone matrix
Investigations:
- High frequency ultrasound scan is done to demonstrate nature of the nodule, whether solid or cystic and to guide FNAC.
- It should be remembered that FNAC cannot differentiate a follicular adenoma from follicular carcinoma. Hence, if FNAC reports as follicular cells, overtreat the patient by total thyroidectomy.
- Some follow with frozen section and proceed. If frozen section is follicular carcinoma, total thyroidectomy is done. No role for open biopsy except in inoperable advanced carcinoma thyroids specially anaplastic carcinoma thyroid.
- Plain X-ray of the involved bone can reveal osteolytic lesions

- Whole body bone scan-I131 is done to rule out multiple osseous metastasis. Flat bones are commonly involved.
- They retain the red marrow for a longer period. Because of increased angiogenesis, secondaries grow more rapidly than primary tumors in follicular carcinoma thyroid.
- A few differential diagnoses of secondaries in the skull bones are given below. Whole-body MRI (91% diagnostic accuracy) to be superior to PET-CT (78% diagnostic accuracy) in detecting bone metastases.
- MRI is excellent in detecting marrow component and osseous and extra skeletal extent of the disease.
Causes of Secondary in the Skull:
- Follicular carcinoma of thyroid
- Renal cell carcinoma
- Hepatocellular carcinoma
- Prostatic carcinoma
- Bronchogenic carcinoma
- CT scan in appropriate cases such as very large tumours adherent to trachea, vessels in the neck and mediastinal extension.
- When primary is not found, bone biopsy is required to find out the site of the primary.
Clinical Notes:
- A patient with a diagnosis of ‘lipoma of the scalp’ was posted for excision in the prone position. As the chief surgeon scrubbed and was about to paint the part, he could see the pulsatile nature of the swelling, which he had missed in the outpatient department.
- Fortunately, it was not excised. A needle was introduced and frank blood was aspirated. Surgery was cancelled. X-ray skull showed osteolytic lesion. She had a small thyroid nodule.
Treatment Of Follicular Carcinoma Of Thyroid
1. Treatment of the Primary:
- Situation 1: When a patient has enlarged thyroid gland and scalp swelling, total thyroidectomy is the treatment of choice. Secondaries do not take up the radioisotope (131I) in the presence of primary tumour. Hence, lobectomy or hemithyroidectomy should not be done.
- Situation 2: A patient undergoes subtotal thyroidectomy for MNG and final report is follicular carcinoma thyroid. In such cases, it is better to do completion thyroidectomy within 7 days or after 4 weeks.
- If done, within 7 days, or after 4 weeks, it is relatively easy to do. Between 7 days and 4 weeks, the inflammatory process would have produced dense fibrosis, chances of injuring RLN, parathyroids are high.
- Situation 3: A patient with solitary nodule—high suspicion of malignancy after sonography and FNAC reported as follicular cells, it is better to go ahead with total thyroidectomy.
2. Treatment of the Metastasis:
- After total thyroidectomy, a whole body bone scan is done to look for metastasis in the bone. Bone metastasis occur in about 15% of patients with follicular carcinoma thyroid. A single secondary can be treated by oral radioiodine therapy, followed if necessary by external radiotherapy depending upon the response of the tumour.
- Multiple secondaries, if present, can best be detected by CT-PET scan and are treated by oral radioiodine therapy. Dose may be around 100 to 200 micro Ci.
3. Postoperative Thyroxine:
- In the postoperative period, patients should receive thyroxine 100 to 200 mg/day to suppress TSH and to supplement thyroxine. The dose may have to be adjusted based on toxicity (tachycardia) and level of TSH.
Prognosis: 15% mortality in 10 years.
Hurthle Cell Carcinoma
- Hurthle cell carcinoma is a variant of follicular carcinoma. It is more aggressive than follicular carcinoma.
- These tumours are defined by the presence of more than 75% of follicular cells having oncocytic features.
- Tumour contains sheets of eosinophilic cells packed with mitochondria.
Hurthle Cell Carcinoma:
-
- More aggressive follicular carcinoma
- More than 75% malignant cells
- More chances of lymphatic spread
- More chances of distant spread
- More chances of mortality
- They secrete thyroglobulin.
- Even if Hürthle cell adenoma is well encapsulated, it is potentially malignant.
- It does not take up 131I. Hence, it is less likely to respond to 131I ablation.
- Higher mortality (20% at 10 years).
- 99mTc—sestamibi scan can detect Hrthle cell carcinoma.
Criteria to Diagnose Hrthle Cell Carcinoma:
- Capsular/vascular invasion, distant metastasis.
- Higher chance of spread to lymph nodes compared to follicular thyroid carcinoma.
- Higher chances of spread to distant sites also.
Follicular Carcinoma Treatment:
- Total thyroidectomy is the treatment of choice. In many cases of Hrthle cell carcinoma, lymph nodes are enlarged. Hence, modified radical neck dissection is done (MRND).
- TSH suppression and follow-up are regularly required.
Follow-up of patients with papillary and follicular carcinoma thyroid—differentiated thyroid cancer
- Serum thyroglobulin (Tg): Thyroid is the only organ which produces thyroglobulin. Levels greater than 10 ng/ml in patients receiving replacement thyroxine therapy indicates presence of metastasis. Hence, assess the serum Tg response to injected recombinant human TSH every year. In thyrotoxicosis and thyroiditis, thyroglobulin levels may be increased.
- Ultrasonography or MRI scans of the neck for localisation of residual or recurrent tumour.
Serum Thyroglobulin:
- Normal value: The normal value for thyroglobulin is 3 to 40 nanograms per milliliter.
- Above 50 nanogram/ml suggests malignancy.
- Above 100 nanogram/ml suggests pulmonary or skeletal metastasis.
- It is produced by follicular cells of the thyroid. Hence elevated in well-differentiated carcinoma. Not in medullary carcinoma thyroid.
- Hence, it is a tumour marker of well-differentiated carcinoma.
- Anti-thyroglobulin antibodies (ATA-TgAb) are found in Hashimoto’s thyroiditis and in Graves’ disease.
Anaplastic Carcinoma
Incidence: 10–12% of cases.
Anaplastic Carcinoma Clinical Features:
Anaplastic Carcinoma Thyroid:
-
- The most rapidly growing thyroid malignancy
- Advanced age group at presentation
- Advanced nature of presentation
- Gross local infiltration—Berry’s sign positive
- No form of treatment is successful.
- Intrinsic carcinoma of larynx spreading outside and infiltrating the skin should be considered as a differential diagnosis.
- Common in elderly women around 60–70 years of age.
- Majority of the patients present with rapidly growing thyroid swelling of short duration. The surface is irregular, and consistency is hard.
- Early infiltration of the trachea results in stridor (scabbard trachea).
- Infiltration of carotid sheath: In such cases, common carotid artery pulsation will not be palpable. This is described as ‘Berry sign positive’. However, superficial temporal artery pulsations will be palpable. It means the lumen is not blocked but common carotid artery is engulfed.
- Early fixity is characteristic. Thus, the respectability rate is almost nil.
- Pathologically highly pleomorphic malignant cells are seen.
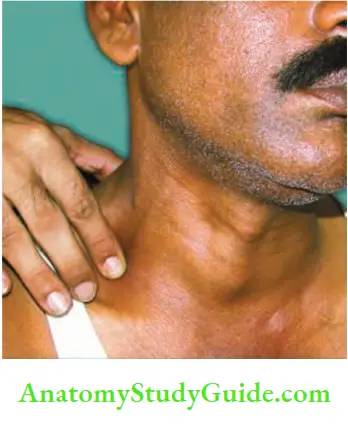
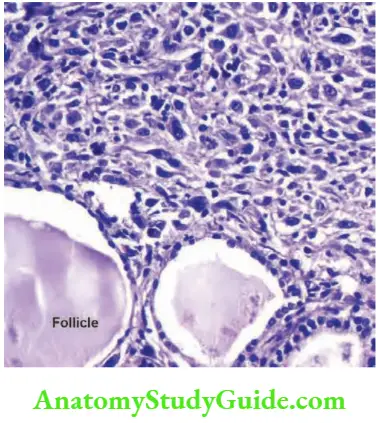
Anaplastic Carcinoma Diagnosis:
It is established by FNAC, other investigation being CT scan.
Anaplastic Carcinoma Treatment:
- Due to the gross local infiltration into the vital structures in the neck, such as common carotid artery and trachea, the respectability rate is low.
- However, very rarely, a surgeon will get an opportunity to excise isthmus so as to relieve compression of the trachea.
- Postoperative radiotherapy is given as a palliative treatment.
- In many cases, death occurs within 6 to 8 months.
Medullary Carcinoma Of The Thyroid
- These tumors arise from parafollicular ‘C’ cells which are derived from ultimobranchial bodies and not from thyroid follicle. Parafollicular cells are pale-staining cells found in the thyroid gland. They are always situated within the basement membrane, which surrounds the entire follicle.
- These tumors present in two different ways.
- Sporadic is common, seen in about 80–90% of cases.
- Familial variety presents as a part of multiple endocrine neoplasia (MEN).
MEN Type I
- Pituitary adenoma
- Parathyroid adenoma
- Pancreatic adenoma
MEN Type 2a
- Parathyroid adenoma
- Phaeochromocytoma
- Medullary carcinoma of thyroid
- When it is associated with mucocutaneous neuromas involving lips, tongue, eyelids, it is called Sipple syndrome, with an occasional marfanoid habitus.
Pathology: It has got a characteristic amyloid stroma.
- These tumours are not TSH-dependent and do not take up radioactive iodine.
Hormones Produced by MCT:
- Calcitonin
- Prostaglandins
- Serotonin (5-HT), ACTH
Medullary Carcinoma Of The Thyroid (Mct) Spread:
- Both by lymphatics and blood, thus worsening the prognosis.
Calcitonin and Medullary Carcinoma Thyroid:
- Not measurable in normal persons
- MCT produces very high levels
- It is the tumour marker of MCT
- Level decreases after thyroidectomy
- Level increases in case of recurrence
- Prophylactic thyroidectomy in relatives, if calcitonin levels are high
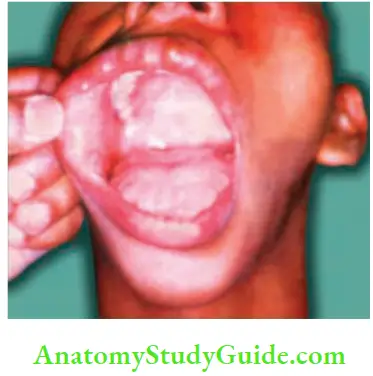
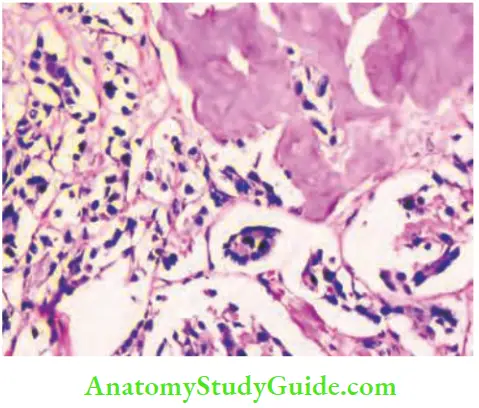
Medullary Carcinoma Of The Thyroid (Mct) Treatment:
- Total thyroidectomy with modified radical dissection
- Before proceeding with surgery, look for an associated phaeochromocytoma.
- The lymph nodes are treated by radical block dissection because they are fast-growing, when compared to papillary carcinoma.
Clinical Criteria for the Diagnosis of Carcinoma of Thyroid: Summary:
- A thyroid swelling which is rapidly growing.
- Thyroid swelling with lower deep cervical lymph nodes and lymph nodes in the posterior triangle (papillary carcinoma thyroid) involved.
- Hard gland, fixed to the trachea—anaplastic carcinoma of the thyroid.
- Thyroid swelling with a rapidly growing, vascular, pulsatile swelling, commonly in the skull (follicular carcinoma).
Summary of the malignant tumours of thyroid gland:
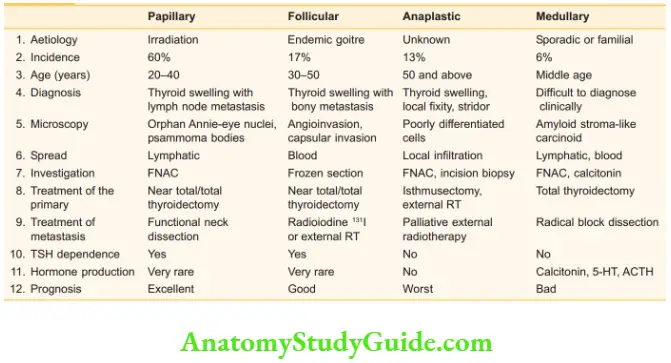
5. Thyroid swelling with hoarseness of the voice indicating infiltration of recurrent laryngeal nerve is a feature of malignancy.
6. Thyroid swelling with Berry sign positive (anaplastic carcinoma of the thyroid).
7. Kocher’s test positive may be an indication of infiltration into trachea. Summary of the malignant tumours of the thyroid gland.
Lymphoma
- It is rare. Hashimoto’s thyroiditis can predispose to lymphoma.
- Older patients are commonly affected.
- The tumour can present as rapidly-growing, large thyroid swelling (primary lymphoma).
- Sometimes, it can appear as a part of generalized lymphoma (non-Hodgkin’s variety).
- FNAC may give the diagnosis—Tru-cut biopsy is ideal.
- It is interesting to note that lymphomas of the thyroid respond very well to chemotherapy and radiotherapy.
Solitary Nodule Of The Thyroid Gland
Definition: Solitary nodule (SN) is a clinical term denoting presence of a single palpable nodule in the thyroid gland (no other part of thyroid gland is palpable).
- Almost all the thyroid swellings initially can present as a solitary nodule. However, puberty goitres, colloid goitres, diffuse toxic goitres produce uniform enlargement of the thyroid gland. Multinodular goitre (MNG) presents as multiple nodules.
- However, very often a solitary nodule on clinical examination, may turn out to be a multinodular goitre at exploration.
- The solitary nodule has a higher incidence of malignancy when compared to MNG.
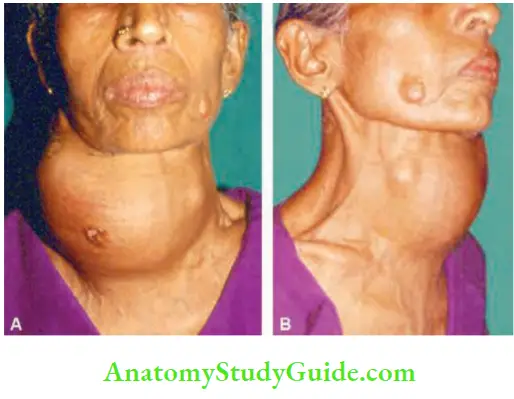
- It is a common surgical problem encountered by general surgeons. By definition, one can call it a solitary nodule when only the nodule is clinically palpable but rest of the gland is not palpable.
- However, when a nodule is palpable and the opposite lobe or any other part of the thyroid is palpable, it is a ‘dominant’ nodule. It may probably be a case of multinodular goitre.
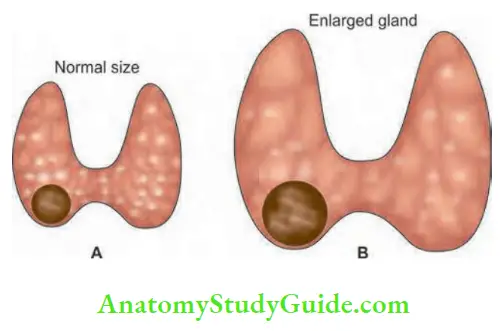
Solitary Nodule Of The Thyroid Gland Introduction:
- It is the most common surgical disease of the thyroid gland. Incidence is about 4%. It is 4 times more common in women than men. About 20 to 30% of patients may have nodules on the other side when detected by ultrasound, thus the diagnosis changes to multinodular goitre. Risk of malignancy is more in a solid nodule and in men. It is about 48%.
- However, in females it is about 12%. In general, incidence of malignancy is 8–10%. Ultrasonography followed by FNAC is the first line of investigations. Aim is to identify a solitary nodule which has high risk, e.g. male, solid, solitary nodule is a nodule which has features suggestive of malignancy.
High Risk Solitary Nodule:
- Male patients with ‘solid’ nodule
- Rapid growing nodule of short duration
- Nodule which has restricted mobility
- Nodule with jugular lymphadenopathy on ultrasound
- Nodule which is hard in consistency
- Nodule with hoarseness of voice
Causes of Solitary Nodule of the Thyroid Gland:

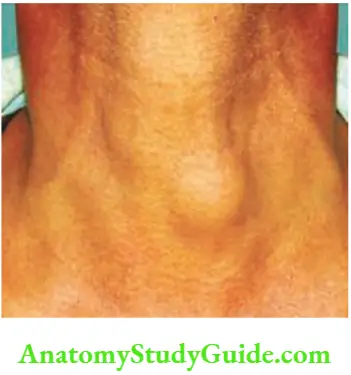
- In about 30 to 40% of the cases, a clinically palpable solitary nodule is a part of multinodular goitre
- Toxic autonomous nodule
- Adenoma
- Carcinoma
- Cysts
Indications for Surgery:
Malignant cytology: Refer to Bathesda Criteria for FNAC thyroid
- Suspicious cytology
- Large size
- Pressure effect, substernal extension
- Clinical suspicion of malignancy
- Cosmesis
- Male sex
- Cyst—recurs after aspiration and bloodstained fluid
Investigations:
1. Blood investigations:
- T3, T4 and TSH: Free thyroxine—better indicator of thyroid status than total T4 . T3is useful when T4 level is borderline (T3 toxicosis). TSH is needed when there is no clinical manifestation of hyper- (or) hypothyroidism.
- Thyroid autoantibodies—when Hashimoto’s thyroiditis is suspected.
- Serum thyroglobulin (STG)—tumour marker
- Normal value is <1–35 nanog/L
- STG level above 50 nanog/L—suggests residual (or) recurrent tumour
- STG level goes above 100 nanog/L suggests pulmonary (or skeletal metastasis)
- Increased in hyperthyroidism, thyroiditis and tumour
- Serum calcitonin—useful for screening medullary carcinoma when a patient has history of thyroid cancer and presents with a solitary nodule.
2. 24 hours collection of urine for catecholamine to exclude phaeochromocytoma (MEN II syndrome) because of association with medullary carcinoma (Rare).
3. Ultrasonography (USG): It is noninvasive, cheap and it has become the investigation of choice in solitary nodule.
- Totally sonolucent unilocular lesions, sonolucent cyst with internal echoes, septae, nodule with homogeneous echogenicity (hyper or hypo), mixed echogenicity and microcalcification enlargement of jugular lymphadenopathy are a few features suggestive of malignancy.
- With increasing use of high frequency ultrasound probe, radionuclide scan is rarely used or almost not used in the evaluation of solitary nodule thyroid gland.
4. Ultrasound-guided fine needle aspiration cytology (FNAC): Using a 22 or 23 gauze needle attached to a 10 ml syringe, under ultrasound guidance, needle is introduced within the gland while maintaining negative pressure and about 4 to 6 passes are done within the gland and syringe and needle are withdrawn.
- Contents are pushed into slides and about 6 slides are prepared and are air dried. Most popular criteria used for FNAC thyroid is Bathesda criteria. (Bathesda is name of the pool in Jerusalem and it is a City in central Maryland).
5. CT scan: Specific indications are: Doubt about the origin of the swelling, large lesion with local infiltration into vascular structures and intrathoracic extension.
6. Isotope scan (not routinely done nowdays): Most commonly used isotope—99mTc. 131I should not be used for evaluation of nodule.
- 123T will not detect nodules of 1 cm size. However, it is indicated in a ‘toxic nodule’ which is ‘hot’.
- Rest of the gland is suppressed, so that such patient can be managed easily by radioiodine. It can demonstrate three different patterns as follows.
Bathesda criteria for FNAC thyroid:
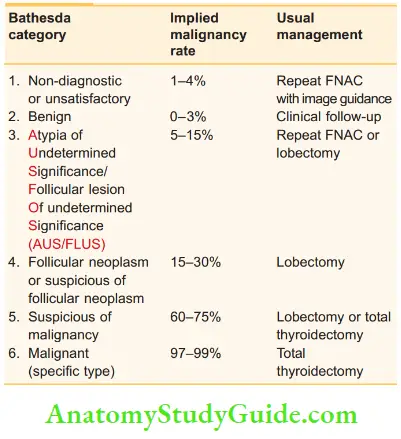
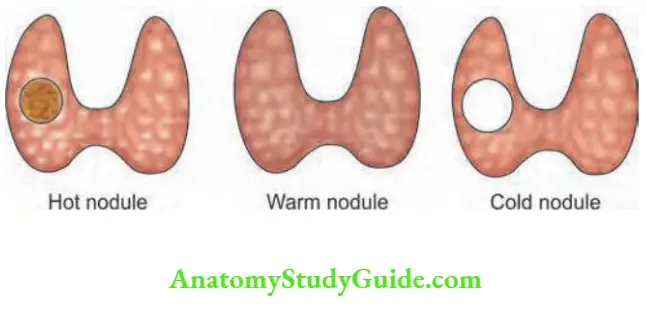
- Hot nodule: The gland does not take up isotope but the nodule takes it up, which is a feature of autonomous solitary toxic nodule.
- Here, the normal thyroid tissue is suppressed. Localisation of over activity in a nodule with suppression of remainder of the gland is characteristic of solitary toxic nodule. In toxic MNG, multiple areas show overactivity.
- Warm nodule: The entire gland takes up isotope. This is typical of Graves’ disease (primary thyrotoxicosis) wherein each cell is active and equally stimulated.
- Cold nodule is a nodule which does not take up isotope. It should be remembered that only 10% of the cold nodules are malignant.
- Keeping this in mind, surgeons do not investigate MNG with isotope scan. The assessment of malignancy is done clinically.
Cold Nodule—Differential Diagnosis:
- Haemorrhage
- Carcinoma
- Thyroiditis
- Thyroid cyst
Clinical Notes:
Case of Thyroid Swelling:
A 31-year-old female with solitary nodule (2 cm) underwent FNAC—reported as adenoma. She underwent hemithyroidectomy in a peripheral hospital which was reported as papillary carcinoma thyroid (PCT). It was a histological surprise. How to proceed now?
- At our hospital, ultrasound neck was done again which could not reveal any abnormality. She underwent completion thyroidectomy (of the opposite lobe) after 4 weeks (re-exploration is done within 7 days or after 4 weeks once tissue oedema subsides completely).
- Thus, the patient underwent total thyroidectomy. HPR of opposite lobe did not show papillary carcinoma. No lymph node dissection was done. The patient was not given T4 for 4 weeks.
- After 6 weeks, 131 I scan was done giving 1 mCi, residual thyroid tissue was found in neck. It was ablated with 100 mCi of 131 I.
- Even though the aim of surgery is to remove the entire thyroid gland (total thyroidectomy), some parts of gland might have been left behind by the surgeon, specially in the region of ligament of Berry. Hence, a routine postoperative radionuclide scan is advisable.
- After ablation, she was put on T4 0.3 mg/day to be taken in the morning on an empty stomach.
- She came after 6 months with pain in the neck for which ultrasound was done. It revealed suspicious residual thyroid tissue.
- What to do now?
- Serum thyroglobulin was estimated. It was <0.2 (almost undetectable limits; Normal 0.2–55). So, the suspicious lesion could have been some fibrous tissue due to surgery. As thyroglobulin was normal, we did not investigate her further.
- Now it is 3 years since completion of thyroidectomy and the patient has no disease but is on T4 0.3 mg/day. What are the annual tests to be done?
- Serum TSH, calcium, thyroglobulin, ultrasound, thyroglobulin antibody and, if necessary, nuclear scan of neck.
Comments:
I have heard in a few surgical meetings, the following statement made by a surgeon, ‘I have done total thyroidectomy, how can residual thyroid tissue be present in the neck?’ Remember, it is always possible that some thyroid tissue is left behind especially in the region of ligament of Berry, tracheoesophageal groove and posteromedially.
Solitary Nodule Of The Thyroid Gland Treatment:
The final decision about treatment of solitary nodule depends upon the clinical findings, sonography findings and FNA cytology results. Depends upon Bathesda criteria, decision is taken. A few examples of treatment when diagnosis is established are given below:
- Papillary carcinoma: Total thyroidectomy Follicular neoplasm: Bethesda 3 or 4: Lobectomy 5 or 6: total thyroidectomy
- Medullary carcinoma: Total thyroidectomy with the modified radical neck dissection
- Adenoma: Lobectomy (hemithyroidectomy)
- Toxic nodule in young: Lobectomy
- Toxic nodule in elderly: Lobectomy or 131I ablation
- Simple cyst: If it resolves after aspiration, wait and watch. If it recurs, do a lobectomy
‘Most Common’ for Solitary Nodule Thyroid:
- Most common surgical disease of thyroid gland is solitary nodule.
- Most of the thyroid diseases begin as solitary nodule.
- Most common investigation of choice for solitary nodule is ultrasonography.
- Most common cause of a solitary nodule is multinodular goitre.
- Most common cause for solid solitary nodule in a male is malignancy.
- Most commonly used investigation of choice for tissue diagnosis is FNAC.
What should not be Done in a Nodule:
- Nodule should never be enucleated.
- Male solitary solid nodule should never be left alone for observation.
- Suppression therapy should never be attempted for a solitary nodule without a definitive diagnosis.
- Radioablation/suppression therapy should never be given to a nodule causing compression on the trachea.
- FNAC should not generally be done to a nodule, if it is a post-irradiated gland or there is familial thyroid cancer.
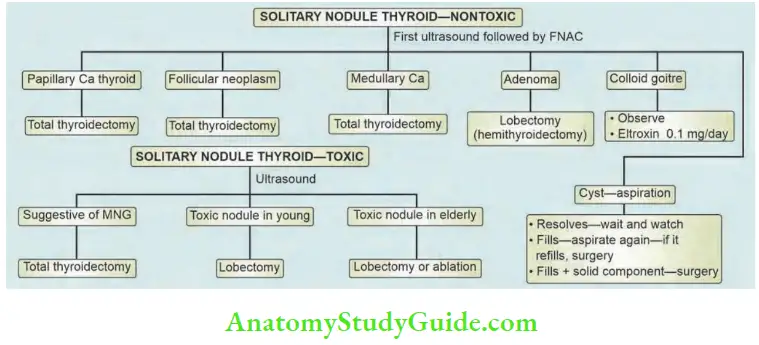
Thyroid Incidentaloma
- As the name suggests, these are incidentally detected during head and neck ultrasonography done for some other problems. I
- n western countries with increasing obesity, and short neck, it is not surprising to see many such cases of incidentaloma detected by ultrasound.
- In such situations, the management is similar to that of a solitary nodule.
- Any lesion more than 1 cm and lesion which is solid should be subjected to sonography-guided FNA.
- Depending on the results of the FNA, treatment is recommended.
- If it is <1 cm, just follow-up with annual sonogram.
Thyroiditis
- Viral and autoimmune thyroiditis are more common in the thyroid gland infection of thyroid is very rare because of its rich blood supply.
- Thyroiditis is broadly classified into granulomatous, autoimmune and Riedel’s thyroiditis.
Granulomatous Thyroiditis
- It is also called subacute thyroiditis or de Quervain’s disease.
- This occurs due to viral infection. It usually follows sore throat (mumps virus has been incriminated in a few cases).
- Patients present with fever, body ache and painful enlargement of thyroid gland. The gland is enlarged, tender to touch, soft to firm and a few symptoms of hyperthyroidism occur initially.
- ESR is increased.
Thyroiditis Treatment:
Majority of the patients respond to conservative treatment in the form of analgesics and a short course of prednisolone. There are no permanent sequelae of this condition.
Autoimmune Thyroiditis:
- Hashimoto’s thyroiditis is the main component of thyroiditis.
- Autoimmune aetiology is characterised by extensive lymphocytic infiltration resulting in destruction of thyroid follicles with variable degree of fibrosis.
- Females in perimenopausal group (40–50 years) are commonly affected. Initially, symptoms of mild hyperthyroidism (Hashitoxicosis) may be present.
- Later, extensive intrathyroidal fibrosis results in permanent hypothyroidism. Transient hyperthyroidism is due to destruction of cells resulting in thyrotoxicosis.
- The thyroid follicles are destroyed by significant fibrosis. The deep eosinophilic-staining thyroid follicular cell, Askanazy cell, is characteristic of Hashimoto’s thyroiditis.
- The gland can be firm to hard and sometimes rubbery in consistency, smooth or irregular and can involve a lobe or the entire gland.
- In many cases, thyroid antibodies are raised, suggesting an autoimmune disorder.
Thyroiditis Treatment:
- Thyroxine 0.2 mg/day is given as a supplementary dose.
- If there is compression on the trachea, isthmusectomy is done to relieve compression.
- If the goitre is big and causing discomfort, subtotal thyroidectomy can also be done.
Complications Of Hashimoto’s Thyroiditis
- Permanent hypothyroidism
- Papillary carcinoma of the thyroid
- Lymphoma
Riedel’S Thyroiditis
- This is a very very rare cause of a goitre which is supposed to be a collagen disorder.
- It can be associated with mediastinal fibrosis, retroperitoneal fibrosis and sclerosing cholangitis.
- In this condition, there is intrathyroidal fibrosis but extrathyroidal fibrosis is more.
- Involvement of trachea, oesophagus, internal jugular vein, carotid artery, etc. results in dysphagia and dyspnoea.
- As a result of fibrosis, all the thyroid follicles are replaced by fibrous tissue.
- By the time patients present to the hospital, it is an advanced stage and excision is very difficult.
Complications Of Hashimoto’s Thyroiditis Treatment:
- Treatment with thyroxine may be necessary to treat hypothyroidism.
- In selected difficult cases, isthmusectomy can be tried to relieve compression on the trachea. Three types of thyroiditis are compared.
Comparison of three forms of thyroiditis:
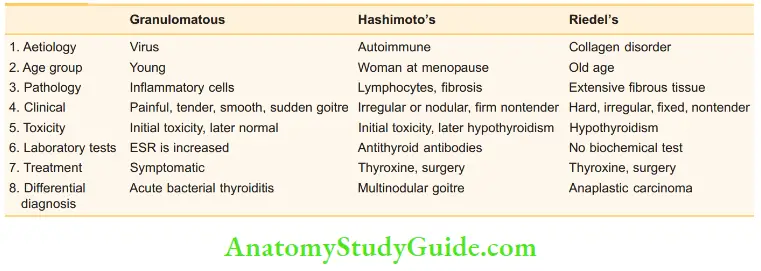
Complications Of Thyroidectomy
1. Haemorrhage can be a primary haemorrhage which occurs during surgery.
- Reactionary haemorrhage is more dangerous and occurs within 6–8 hours after surgery. This is due to slipping of ligature because of straining, coughing, hypertension, etc.
- It is a tension haematoma which develops deep to deep fascia, compressing the larynx. Reexploration of neck under GA, control of bleeding points and evacuation of haematoma should be done immediately.
- Without evacuating haematoma, an attempt to intubate the patient may result in cardiac arrest (as such patient will be struggling).
2. Respiratory obstruction can be due to tension haematoma resulting in compression of the larynx, collapse, tracheal cartilage softening (tracheomalacia).
Endotracheal intubation and a short course of steroid therapy is necessary.
3. Laryngeal nerve paralysis: Unilateral recurrent laryngeal nerve (RLN) palsy produces a whispering voice. The opposite vocal cord compensates. There will not be problems of aspiration or airway obstruction.
2. Bilateral recurrent laryngeal nerve palsy: It is also known as bilateral abductor paralysis. Both the vocal cords come to be in median or paramedian position, the airway is inadequate causing dyspnoea and stridor but the voice is good.
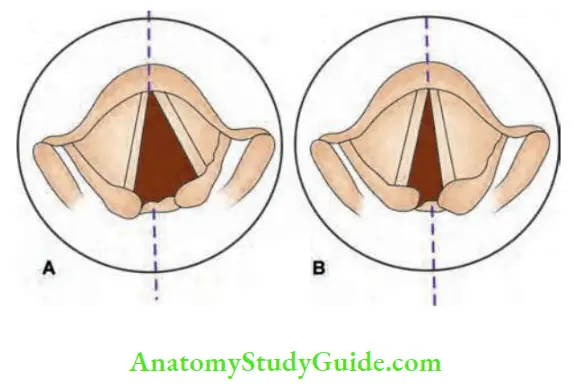
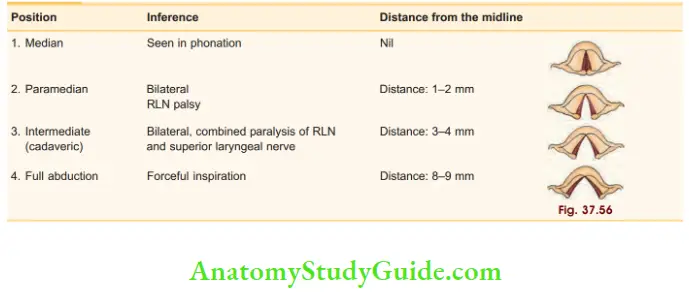
Causes of recurrent laryngeal nerve paralysis:
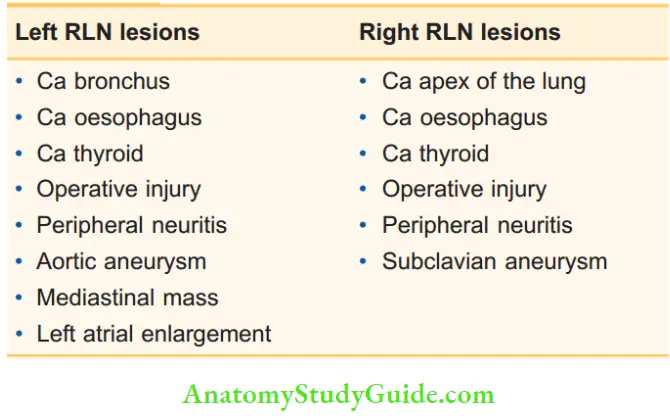
Complications Of Thyroidectomy Treatment:
- Tracheostomy is required as an emergency procedure. Following tracheostomy, the patient is followed up on an outpatient basis for a period of 8–9 months.
- This period is required for any spontaneous recovery. If no recovery occurs after this period, it requires a permanent solution.
- The choice is between a permanent tracheostomy with a speaking valve or a surgical procedure to lateralise the cord which can be done by endoscopic method.
- The former relieves stridor and preserves good voice but has the disadvantage of a tracheostomy hole in the neck.
- The latter relieves airway obstruction but at the expense of good voice. However, there is no tracheostomy hole in the neck.
Lateralisation of the cord:
- It means to move and fix the arytenoid, vocal process and vocal cord into an abducted position.
- Endoscopic lateralisation can be done by laser cordotomy.
- KTP-532 nm laser is used.
- It is minimally invasive, single procedure, quick recovery.
3. Superior laryngeal nerve (SLN): It is a branch of vagus, gives a ‘motor’ branch—external laryngeal nerve. Dissection and retraction of the upper pole of the right thyroid lobe to reveal the external branch of the superior laryngeal nerve in the cricothyroid space of Reeves. This nerve supplies cricothyroid which is adductor of the cord.
- Paralysis causes weak and husky voice and inability to raise the pitch of voice. This is of particular importance in singers. Amelita Galli Curci, an Italian opera singer lost her voice following thyroidectomy due to damage to SLN.
- Large internal laryngeal nerve supplies whole supraglottic larynx—sensory innervation to the epiglottis, pyriform sinus and larynx as far down as vocal folds.
4. Combined (complete paralysis):
Unilateral: This results in paralysis of all muscles of larynx on one side. Vocal cord will be in cadaveric position. The healthy cord is unable to approximate the paralysed cord, thus causing glottic incompetence. This results in hoarseness of voice and aspiration of liquids through glottis. Cough is ineffective due to air wastage. Treatment includes procedures to medialise the cord and speech therapy.
Bilateral: This is an uncommon condition. This results in paralysis of all the intrinsic muscles of the larynx. Both vocal cords assume cadaveric position. There is also a total anaesthesia of larynx.
4. Permanent hypothyroidism can develop slowly after thyroid surgery especially after subtotal thyroidectomy for Graves’ disease. It takes 2–3 years for manifestation of hypothyroidism to become apparent.
5. Permanent hypoparathyroidism is managed with calcium tablets or with 1, 25-dihydroxy cholecalciferol.
6. Thyrotoxic crisis (storm):
- Thyrotoxic storm occurs in patients with primary thyrotoxicosis who are improperly treated or prepared for surgery. At surgery, due to handling of the gland, sudden release of thyroxine into the systemic circulation results in thyrotoxic crisis.
- Hyperpyrexia—above 105°F, severe sweating, gross dehydration, hypovolaemic shock and tachycardia are the diagnostic features.
- It is treated by following measures:
- ICU admission and resuscitation: O 2, correction of dehydration by rapid IV fluids.
- Cold tepid sponging, to control the temperature.
- IV and oral propranolol 2–4 mg and as necessary.
Thyrotoxic Storm Prevention:
- Euthyroid before surgery
- β-blockers, carbimazole
- Lugol’s iodine
- Good anaesthesia
- Perfect haemostasis
- Gentle manipulation
- Hydrocortisone 100 mg, thrice daily.
- Carbimazole or propyl thiouracil
- In spite of the above treatment, mortality is high.
What is Wolff-Chaikoff effect?
- On ingestion of a large amount of iodine, there will be reduction of thyroid hormones.
- It is an autoregulatory mechanism which inhibits organification in the thyroid gland.
- This principle is used to treat hyperthyroidism (especially thyroid storm by infusion of iodine—large quantities).
7. Wound infection: It is not common to get wound infection after thyroid surgery. However, antibiotics are started, if there is evidence of local erythema, tenderness and if the patient has fever.
8. Scar hypertrophy and keloid.
9. Stitch granuloma: May occur with/without sinus formation and is seen after the use of nonabsorbable suture material. Absorbable ligatures and sutures (vicryl) can be used throughout thyroid surgery except for skin closure where silk is still appropriate.
Miscellaneous Lingual Thyroid
- Occasionally, a patient presents with a small swelling in the middle of the tongue at the junction of anterior 2/3rd and posterior 1/3rd of the tongue.
- It could be lingual thyroid—an aberrant thyroid tissue found in the region of foramen caecum on the tongue.
- Foramen caecum represents the junction of epithelial floor of the mouth with proximal portion of thyroglossal duct.
- Even though lingual thyroid is rare, it can give rise to significant complications.
Miscellaneous Clinical Features:
- Common in females (3:1)
- Swelling in the tongue in the classical location, firm in consistency, can be irregular. Impairment of speech, haemorrhage, dysphagia, airway obstruction may be the presenting features.
- Majority of patients have hypothyroidism (70%) and 10% are cretins.
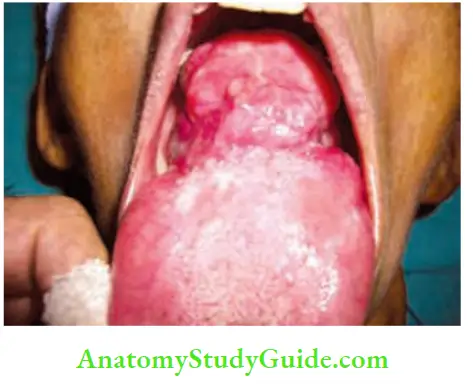
Miscellaneous Diagnosis:
- Usually made on clinical grounds.
- Thyroid scan—ultrasound of neck is done to find out whether thyroid tissue is present or not (often it is absent).
- 99mTc (technetium) scan will detect ectopic thyroid tissue.
Differential Diagnosis:
- Ectopic salivary gland tumour: Tongue is the commonest site. To begin with, mucosa is normal, starts as a submucosal swelling.
- Gumma: Rare nowadays. It is a midline, indurated, firm, smooth swelling, painless.
- Lymphangioma and haemangioma: These are present since birth, more diffuse, fluctuant cystic swellings. Haemangioma is compressible and lymphangioma is transilluminant.
Miscellaneous Treatment:
- Small dose of thyroxine may decrease the size of the swelling (similar to a puberty goitre) as a treatment of hypothyroidism or to suppress TSH
- Large swelling with significant symptoms needs to be excised. Laser excision is better.
- Radioactive iodine to suppress/destroy can be given.
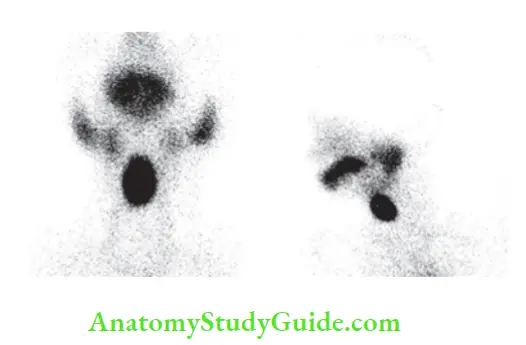
Ectopic Thyroid
- It occurs due to failure of median thyroid anlage to descend normally. Hence, thyroid tissue can be found anywhere from the tongue to mediastinum.
- Ectopic thyroid tissue can have the diseases similar to normal thyroid tissue, such as solitary nodule, multinodular goitre, malignancies, etc.
Ectopic Thyroid Tissue:
- Lingual thyroid
- Thyroglossal ectopic thyroid in the upper part of the neck
- Adjacent to aortic arch, aortopulmonary window, within upper pericardium, etc.
- Struma ovarii—malignant ovarian teratoma containing thyroid tissue.
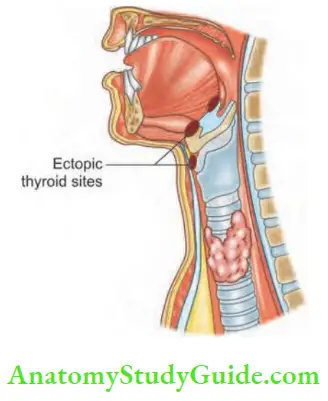
- Diagnosis is by ultrasound, CT scan. FNAC to confirm the diagnosis.
- Treatment depends upon the pathology.
Interesting ‘Most Common’ For Thyroid Gland:
- Most common surgical disease of the thyroid gland is solitary thyroid nodule.
- Most common site of thyroid nodule is at the junction of isthmus and lobe.
- Most commonly used drug for thyrotoxicosis is carbimazole.
- Most commonly used investigation for thyroid diseases is ultrasonogram.
- Most commonly done surgery for well-differentiated carcinoma thyroid is total thyroidectomy.
- Most common thyroid cancer in children is papillary carcinoma thyroid.
- Most common thyroid cancer following exposure to ionising radiation is papillary carcinoma thyroid.
- Most common solitary nodule of thyroid gland is multinodular goitre.
Most Diagnostic Features In Thyroid Gland:
- Most diagnostic feature of medullary carcinoma thyroid is amyloid stroma.
- Most diagnostic feature of papillary carcinoma thyroid is presence of psammoma bodies.
- Most diagnostic feature of Hashimoto’s thyroiditis is Askanazy cell.
- Most diagnostic investigation for lingual thyroid is 99mTc (technetium) scan.
- Most diagnostic feature of anaplastic carcinoma is early fixity
- Most diagnostic feature of Graves’ disease is exophthalmos
Thyroid Gland Multiple Choice Questions
Questions 1. Superior thyroid artery is a branch of:
- Common carotid artery
- Internal carotid artery
- External carotid artery
- Thyrocervical trunk
Answer: 3. External carotid artery
Questions 2. Following are true for T3 hormone except:
- It is more important physiologic hormone
- It can be produced by peripheral conversion of T4
- It is more quickly acting
- It is given once a day for suppressive dose
Answer: 4. It is given once a day for suppressive dose
Questions 3. Following are true for primary thyrotoxicosis except:
- 8 times more common in women than men
- Gland is vascular and smooth
- Cardiac failure is common
- Proptosis is a feature
Answer: 3. Cardiac failure is common
Questions 4. Replacement dose of thyroxin—T4 is:
- 0.1 mg
- 0.2 mg
- 0.3 mg
- 0.01 mg
Answer: 1. 0.1 mg
Questions 5. Papillary carcinoma thyroid spreads to which lymph nodes?
- Submental
- Submandibular lymph nodes
- Scalene nodes
- Jugular chain of lymph nodes
Answer: 4. Jugular chain of lymph nodes
Questions 6. Following is not the common sign of Graves’ disease:
- Proptosis
- Pretibial myxoedema
- Proximal myopathy
- Cardiac failure
Answer: 4. Cardiac failure
Questions 7. The widely used first investigation of choice in solitary nodule thyroid is:
- X-ray neck
- CT scan
- MRI
- Ultrasound
Answer: 4. Ultrasound
Questions 8. Which one of the following is not the treatment for Graves’ disease?
- Carbimazole
- Propranolol
- Massive doses of steroids in ophthalmopathy
- Digoxin
Answer: 4. Digoxin
Questions 9. Following are true for treatment options for toxic goitre except:
- Thyroidectomy
- Antithyroid drugs
- Radioiodine treatment
- Radiotherapy
Answer: 4. Radiotherapy
Questions 10. Which one of the following is the treatment of choice for toxic goitre in a child?
- Radioiodine
- Thyroidectomy
- Antithyroid drugs
- Radiotherapy
Answer: 3. Antithyroid drugs
Questions 11. Which is the most effective drug for thyrotoxic storm?
- Steroids
- Noradrenaline
- IV propranolol
- Carbimazole
Answer: 3. IV propranolol
Questions 12. Which one of these operative steps is not done routinely in thyroidectomy?
- Ligation of middle thyroid vein
- Ligation of superior thyroid artery
- Ligation of inferior thyroid artery
- Ligation of inferior thyroid veins
Answer: 3. Ligation of inferior thyroid artery
Questions 13. A few landmarks for identification of recurrent laryngeal nerve include following except:
- Parallel to tracheo-oesophageal groove on the left side
- Below the inferior thyroid artery on the right side
- Between branches of the inferior thyroid artery
- Between the branches of inferior thyroid veins
Answer: 4. Between the branches of inferior thyroid veins
Questions 14. Following are true for external branch of superior laryngeal nerve except:
- It is close to superior thyroid artery
- Paralysis of this nerve leads to loss of tension in the vocal cord
- Paralysis of this nerve diminishes power and range in the voice
- It supplies adductors of the vocal cord
Answer: 4. It supplies adductors of the vocal cord
Questions 15. Following are true for papillary carcinoma thyroid except:
- Childhood irradiation is an important cause
- Orphan Annie-eyed nuclei is characteristic
- Multiple foci are common in the same lobe
- It spreads predominantly by blood spread
Answer: 4. It spreads predominantly by blood spread
Questions 16. Single most important aetiological factor in papillary carcinoma is:
- Endemic goitre
- Childhood irradiation
- Autoimmune thyroiditis
- Multiple endocrine neoplasia syndromes
Answer: 2. Childhood irradiation
Questions 17. Following are the important steps of surgery for welldifferentiated thyroid cancers of more than 2 cm in size except:
- Lobectomy
- Total thyroidectomy
- Selective neck dissection
- Removal of all macroscopic diseases
Answer: 1. Lobectomy
Questions 18. Following are true after total thyroidectomy before radioiodine scan except:
- If T3 is given, only one week of stopping of hormone is enough
- Otherwise minimum 4 weeks stoppage of T4 is required
- Alternative to thyroxine withdrawal is to administer synthetic TSH over 48 hours
- TSH administration is not at all effective
Answer: 4. TSH administration is not at all effective
Questions 19. Following are true about thyroglobulin except:
- Normal levels are not detectable
- Increasing levels indicate metastasis in papillary carcinoma thyroid
- Increasing thyroglobulin prompts surgeon to get ultrasound of the neck
- Useful in medullary carcinoma thyroid
Answer: 4. Useful in medullary carcinoma thyroid
Questions 20. Following are true for medullary carcinoma thyroid except:
- Calcitonin is the tumour marker
- It arises from parafollicular cells
- It has amyloid stroma
- It can be treated by lobectomy
Answer: 4. It can be treated by lobectomy
Questions 21. Following is an indication for core needle biopsy of thyroid swellings:
- Lymphoma
- Papillary carcinoma thyroid
- Follicular carcinoma thyroid
- Medullary carcinoma thyroid
Answer: 1. Lymphoma
Questions 22. Following are pathological features of papillary carcinoma except:
- Microcarcinoma
- Orphan Annie-eyed nuclei
- Tall cell cancer
- Hürthle cell cancer
Answer: 4. Hürthle cell cancer
Questions 23. Following are true for medullary carcinoma thyroid except:
- It arises from parafollicular cells
- Cells are like carcinoid tumour
- Does not spread by lymphatics
- Tumours are not TSH dependent
Answer: 3. Does not spread by lymphatics
Questions 24. Follicular carcinoma thyroid is diagnosed by:
- Orphan Annie-eyed nuclei
- Askanazy cell
- Angioinvasion and capsular invasion
- Amyloid stroma
Answer: 3. Angioinvasion and capsular invasion
Questions 25. Non-operative treatment can be offered in a solitary nodule except:
- Cyst less than 1 cm size
- Colloid goitre less than 1 cm in size
- Retrosternal goitre
- Hashimoto’s thyroiditis
Answer: 3. Retrosternal goitre
Questions 26. Parafollicular cells are located in which part of thyroid gland?
- Upper pole
- Lower pole
- Isthmus
- Organ of Zuckerkandl
Answer: 1. Upper pole
Questions 27. About recurrent laryngeal nerve (RLN) following are true except:
- RLN crosses medial to inferior thyroid artery
- Superior parathyroid is posterior to RLN
- Inferior parathyroid is 1 cm away from RLN
- RLN passes immediately medial to tubercle of Zuckerkandl.
Answer: 3. Inferior parathyroid is 1 cm away from RLN
Leave a Reply