Umbilical Hernia
It can be discussed under three headings:
Table of Contents
- Umbilical hernia of newborn
- Umbilical hernia of infants and children
- Umbilical hernia of adults.
Umbilical Hernia Of Newborn
- It is called omphalocele—exomphalos.
- It is found in 1 in 6000 live births.
- Failure of the midgut as a whole or part to return into the coelomic cavity during embryonic life results in exomphalos.
- It is also associated with weakness of abdominal musculature (a few fibers may be absent). Two types have been recognized.
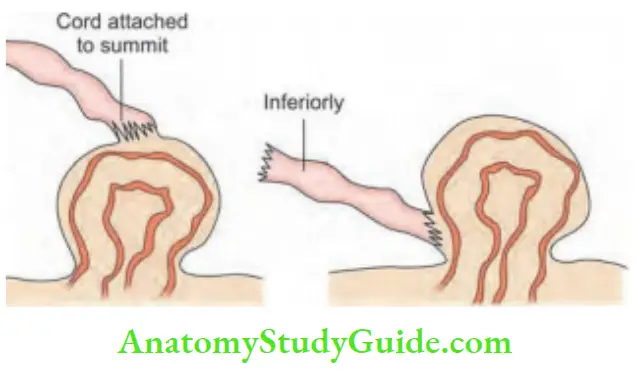
1. Exomphalos Minor
- In this condition, the umbilical cord is attached to the summit of the sac
- The sac is small and defects less than 5 cm. It is treated by twisting the cord and ligating the sa
- Care should be taken to avoid damage to the intestine. For example, nursing the child preoperatively in a prone position can damage the intestines.
2. Exomphalos Major
- In this condition, the umbilical cord is attached to the inferior aspect of the sac, containing intestines, and abdominal structures, e.g. liver, and bowel.
- Many children are stillborn. This type of hernia is usually associated with absent abdominal musculature.
- The operation should be done before the rupture of the sac as the morbidity increases greatly in the event of a rupture of the sa
- During the operation, skin flaps are raised on both sides to cover the defect. A true repair is necessary and is done at a later date.
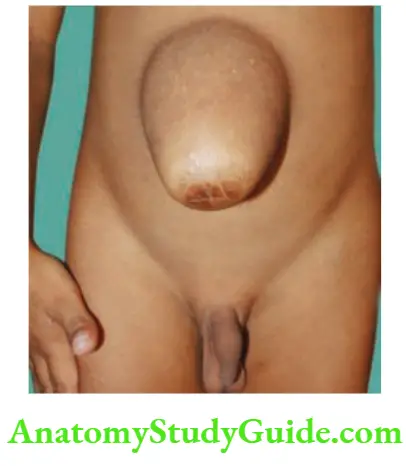
Umbilical Hernia Of Infants And Children
- It occurs as a complication of umbilical sepsis, which weakens the umbilical scar.
- It is a true umbilical hernia containing either omentum/intestines.
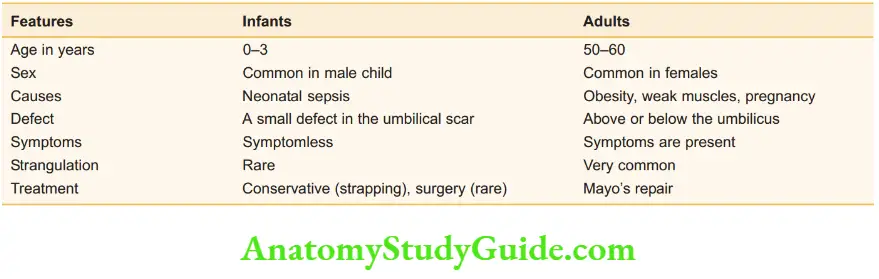
Umbilical Hernia Clinical Features
- Common in male children
- The child is brought with the complaint of swelling in the umbilical region whenever the child cries.
- Most of the cases are symptomless. Parents are anxious about the swelling.
- Strangulation is rare.
Umbilical Hernia Treatment
- Reassurance is the most important advice given to parents.
- No treatment is required other than strapping the abdominal wall by keeping a pad in front of the umbilicus.
- The majority of the hernias get corrected by 2 years of age (90%).
- If the hernia does not correct itself, repair is necessary to close the defect in the linea alba.
Umbilical Hernia Of Adults
- It is not a true umbilical hernia but it is a paraumbilical hernia in which the hernia occurs either above, below, or to the side of the umbilicus, through the linea all
- The contents are the greater omentum, transverse colon, or small bowel. Due to adhesion, it is often irreducible.

Umbilical Hernia Of Adults Aetiology
- Females in the 5th decade are commonly affected
- Male: female ratio is 1:5.
- Obesity with flabby abdominal muscle predisposes to paraumbilical hernia
- Repeated pregnancies also weaken the abdominal wall.
- Ascites may precipitate hernia, especially in cirrhotic patients.
Umbilical Hernia Of Adults Clinical Features
- The patient presents with a swelling in the umbilical region, which increases with straining or coughing.
- On asking the patient to cough, the expansile impulse is present. They may also have inguinal herniReducibility can be present.
- Dragging pain is usually due to omentum which is felt as a firm or granular mass. If gurgling is present, it is indicative of small intestines in the hernial sa
- After reducing the swelling, the defect can be felt in the linea alba.
- For comparison between umbilical hernia in infants and adults.
Umbilical Hernia Of Adults Complications
- Irreducibility is common due to adhesions between the omentum and the sa
- Obstruction presents with colicky abdominal pain and vomiting. Distension follows soon. Untreated cases develop strangulation. Very often, these patients present with incarcerated hernia due to the presence of a transverse colon in the They require urgent intervention, failing which gangrene will set in.
- As the sac enlarges, due to its weight and gravity, it sags down resulting in friction of the skin and this causes intertrigo.
Umbilical Hernia Of Adults Treatment
- Reduction of weight.
- Anatomical repair: Small defects can be closed with nonabsorbable sutures such as nylon or proline.
- The most favored surgery for umbilical hernia is laparoscopic mesh repair—IPOM (intraperitoneal onlay mesh repair).
- It is a tensionless repair. It can also be done by laparoscopic method which is popular today.
- However, the cost of the mesh and tackers for laparoscopic repair is a limiting factor, especially in unaffordable patients.
- Mayo’s repair. Not done nowadays. In case of obstruction or strangulation, some surgeons may do this whereas others prefer anatomical closure.
Mayo’s Umbilical Herniorrhaphy
- Excision of umbilicus
- Reduction of contents and excision of the sac
- Double breasting of the fibrous aponeurotic layer
- Hemostasis, suction, and obliteration of dead space
- Additional lipectomy and umbilicoplasty

Incisional Hernia
Describe the classification of ventral hernias and clinical presentation and indications for surgical management of various ventral hernias.
It is also called ventral hernia or postoperative hernia. It is a hernia that occurs through a weak scar. Very common in females.


Abdominal Wall—Surgical Anatomy
Ventral Hernias Contents
- It consists of skin, muscles, aponeurosis, linea alba, sheaths, ligaments, openings—rings, blood vessels, and nerves.
- Anatomically weak areas are the rings, junctions, empty spaces, and where blood vessels pierce the abdominal wall.
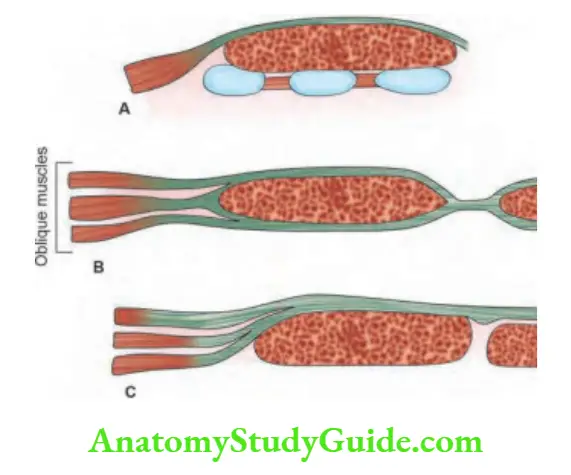
Formation of Rectus Sheath
- Above the costal margin, only the external oblique with aponeurosis contributes to the rectus sheath.
- Between the xiphisternum and umbilicus, the external oblique is in front. Internal oblique splits to enclose the rectus muscles. The transverse abdominis is behind the internal oblique. All fuse to form linea alba in the midline. Hence, this is the strong midline area.
Below the semilunar line: All 3 aponeuroses are anterior to the muscles and fuse in the midline to form the linea alba.
Ventral Hernias Significance
- Rectus sheath—posterior rectus sheath is absent below the semilunar line. Incisional hernia and spigelian hernia are common below the umbilicus.
- Linea alba—white, relatively avascular, broad above and narrow below. It is the strongest layer of the abdominal wall. Hence, during the closure of the midline incisions, it is important to include good bites through linea alb
- Umbilicus—strong fibrous ring. Umbilical hernias are common in children due to childhood umbilical infections, in obese patients due to weak muscles, and in multiparous women due to stretching of the muscles due to repeated pregnancies.
Leave a Reply