Access Flap
Open flap debridement offers visibility and accessibility into periodontal sites that are otherwise difficult to reach.
Question 1. Define periodontal flap. Write the classification.
Answer:
Classification Of Periodontal Flaps
Read And Learn More: Periodontology Important Question And Answers
- Based of Flap Thickness
- Full thickness flaps: These flops are mucoperiosteal in nature and result in exposure of bone and are usually used in osseous surgery.
- Partial thickness flops: The flip consists of epithelium and connective tissue- a mucosal or split-thickness flap. Here, the periosteum is left intact to protect the bone and it is usually used when tissue is to be repositioned.
- Based on Position
- Repositioned flops: The flap is repositioned in a postoperative position that is different to the preoperative one. On the basis of the direction in which the flap is repositioned, these flaps are further classified into apically, laterally, and coronally repositioned flaps.
- Un-repositioned flaps: These flaps are sutured back in the presurgical position. Examples the sulcular incision flap, the modified Widman flap, the papilla preservation flap, and the internal bevel gingivectomy.
- Based on the Papillary Incision
- Split papilla or conventional flaps: The interdental incision is placed as described later.
- Papilla preservation flap: The interdental papilla is completely preserved on either the facial or lingual/palatal flap. It is useful in the preservation of esthetics and in reconstructive osseous surgery.
- Based on Shape
- Envelope flap: Flap is elevated without a vertical incision.
- Triangular flap: One vertical incision is placed in addition to the horizontal incisions, which may be used for limited improvement in access.
- Trapezoidal flap: Vertical incisions are placed on either end of the horizontal incision(s) and ensures good surgical access to the underlying area.
Question 2. Write on indications of flap therapy in the treatment of periodontal disease.
Answer:
- Deep periodontal pockets measuring over 6 mm in depth
- Vertical osseous defects
- Pulpo-periodontal lesion
- Presence of sinus openings, mucogingival deficiencies, etc.
- Furcation involvement.
Question 3. Describe incisions in periodontal flap surgery.
Answer:
Incisions are primarily classified as horizontal and vertical incisions.
Horizontal Incisions Are Further Classified
- Internal bevel incision or primary incision. It is directed at an internal angle of 45° to the long axis of the tooth, begins apical to the gingival margin, and ends at the base of the bony defect.
- Advantages of this incision are the elimination of the soft tissue lining. The gingival margins are obtained and the uninvolved outer keratinized epithelium is preserved.
- Crevicular incision (sulcular incision): It is placed along the long axis of the tooth and a triangular wedge of tissue is created.
- Interdental incision: The facial and lingual papillae are separated and the flap is freed from the tooth.
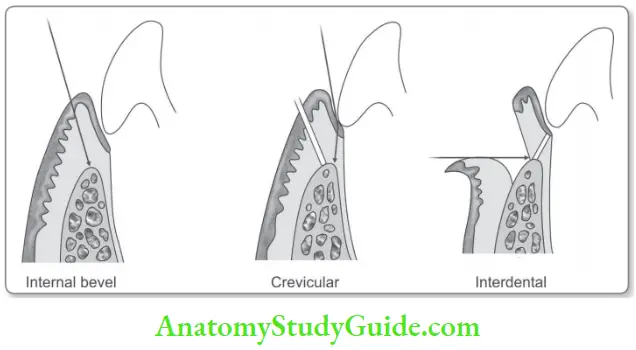
All these incisions when placed correctly, the scalloped outline of the gingiva is maintained along with treatment of the underlying disease.
Vertical Incisions
- This is placed when more accessibility is required than is provided by horizontal incisions alone, for example in repositioned flaps or pockets in isolated areas.
- Vertical incisions are placed either including or excluding the papilla completely, root prominences are avoided and are placed with a broader base than apex.
Question 4. What are the various pocket reduction/elimination flap procedures?
Answer:
Modified Widman Flap
- The flap is mobilized using the internal bevel incision, crevicular incision, and interdental incision.
- The internal bevel incision is made 0.5–1.0 mm apical to the gingival margin to the base of the pocket.
- It is indicated for pockets >6 mm deep where the gingival phenotype is thick without preexisting gingival recession.
Undisplaced Flap or Internal Bevel Gingivectomy: The internal bevel incision is made starting from the base of the pocket and is therefore a pocket elimination procedure. It is indicated in the combined pockets, where the attachment loss is mild to moderate.
Apically Repositioned Flap
- When the base of the pocket crosses the mucogingival junction apically repositioned flap is indicated.
- This procedure can reduce pocket depth and increase width of the attached gingival simultaneously.
- The disadvantages are anesthetic root exposure increasing predilection for hypersensitivity and root caries.
Question 5. Write a note on suturing techniques.
Answer:
- Interrupted sutures: Simple interrupted and the figure of eight sutures are its examples.
- Horizontal and vertical mattress sutures: These sutures involve taking 2 bites in the horizontal or vertical plane in both papillae, which may be used for closer adaptation in repositioned surgeries or graft-related procedures.
- Continuous sling sutures: They utilize support of teeth so that flaps are coapted in a position that will prevent them from collapsing into the dead space due to lack of support.
Question 6. Periodontal dressing/periodontal packs.
Answer:
After the surgery, the area is covered with a surgical pack. The dressing has no curative effects, they assist healing by protecting the tissues.
The pack serves the following functions:
- Controls minimal post-operative bleeding.
- Minimizes post-operative infection by isolating the surgical site from physical and chemical stimuli.
- Provides some splinting of mobile teeth.
Types of Pack: Numerous types of packs are available. The most common types are
- Zinc-oxide Eugenol Pack: Based on reaction of zinc oxide and eugenol applied since the time of inception as Wonder – pack. If eugenol acts on gingival tissues irritation may be produced.
- Non-eugenol Packs
- Coe-Pak: It is supplied as two tubes one of which contains zinc oxide, an oil (plasticity), a gum (for cohesiveness), and lorothidol (fungicide), and the other liquid coconut fatty acid thickened with colophony resin and chlorophyll.
Other packs are:
- Cyanoacrylates: Contains N-butyl cyanoacrylate that solidifies in 5–10 seconds.
- Light Cure-Based Packs:
- Commercially available as a system that hardens on the tooth surface on exposure to light cure.
- Tissue conditioners: Methacrylic with some modifications to increase their adhesion and rigidity.
Question 7. Describe healing after periodontal flap surgery.
Answer:
- Healing of flap occurs in 3 phases: The inflammatory phase, granulation tissue formation phase, and wound maturation phase.
- In the initial phase (24 hours), a blood clot is formed, the inflammatory cells such as neutrophils reach the area and remove the debris that is required to cleanse the wound area.
- During the next phase, the blood clot becomes organized into a granulation tissue that contains growth factors that are required for tissue healing.
- Subsequently in the final phase, there is strengthening of the wound through the formation of collagen fibers that ultimately provide the necessary strength to the healing site.
- Epithelization begins early in the wound site and as the epithelial cells are the fastest to reach the wound site, a long junctional epithelium is formed after conventional flap surgery. There is no formation of new cementum, PDL and alveolar bone.
Leave a Reply