Posterior Abdominal Wall Question And Answers
Posterior Abdominal Wall
Question – 1: Describe the Renal Artery under the following heads
1. Renal Artery Origin
2. Renal Artery Course and relations
3. Renal Artery Branches, and
4. Renal Artery Applied anatomy.
Table of Contents
Answer:
Posterior Abdominal Wall Introduction:
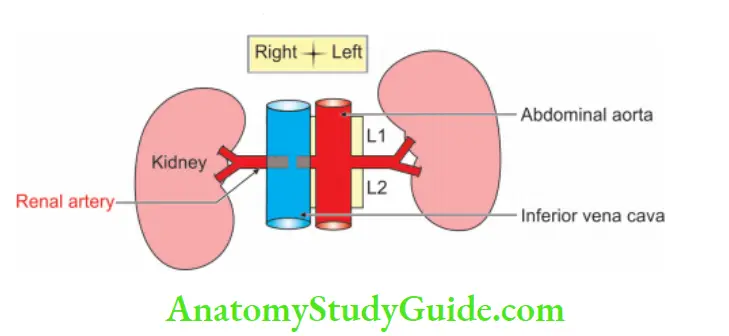
The renal arteries are the largest arteries of the abdominal aorta supplying kidneys, suprarenal glands and the ureters.
- They are one of the most important lateral branches.
- The renal arteries take about 20% of the cardiac output, which is approximately 1.2 litres/minute.
- They supply organs that represent 1/100th of the total body weight.
Read And Learn More: General Histology Question And Answers
1. Posterior Abdominal Wall Origin
They are direct branches of abdominal aorta; hence, they are high pressure arteries. They arise at right angle between L1 and L2 vertebrae. They lie below the origin of superior mesenteric artery and above the origin of gonadal arteries.
2. Posterior Abdominal Wall Course And Relations
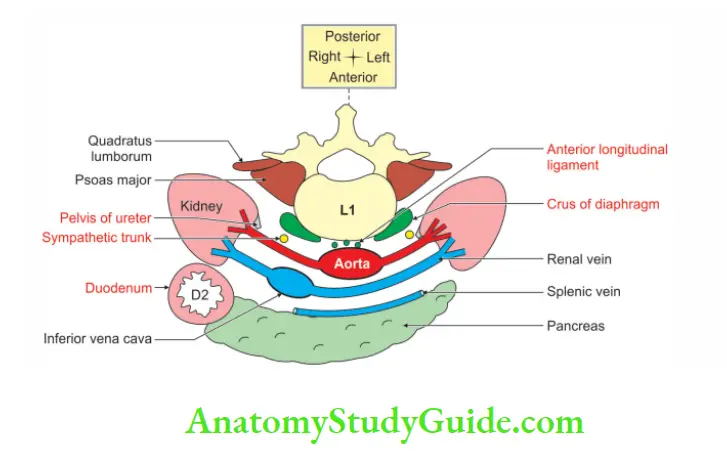
Relations at the hilum of kidney are VAU, i.e. renal Vein, renal Artery and pelvis of Ureter from the front backward.
1. The left renal artery is little shorter and little lower than the right. It passes behind the
- Left renal vein
- Body of the pancreas, and
- Splenic vein.
2. It may be crossed anteriorly by the inferior mesenteric vein.
3. It crosses the
- Left crus of diaphragm
- Left psoas major muscle and runs behind the left renal vein.
4. The renal vessels are covered by splenic vessels and the tail of pancreas. The right renal artery is longer, and little lower, than the left renal artery.
5. It is bedded by the right crus of diaphragm and right psoas major muscle. It is blanketed by the inferior vena cava and short renal vein.
6. The blankets, i.e. inferior vena cava and short renal vein are covered by the head of pancreas, bile duct, and 2nd part of duodenum.
3. Posterior Abdominal Wall Branches
1. Within the renal sinus, the renal arteries divide further into primary branches. They give rise to an anterior and a posterior division.
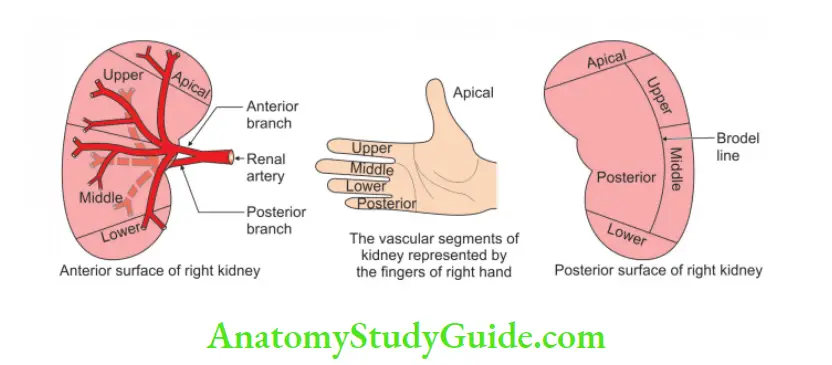
2. The anterior division gives branches that supply the apical, the upper, middle and lower segments.
3. The posterior division supplies posterior segment.
4. Each of them supplies a specific region of renal tissue, there being no anastomoses between arteries to adjoining regions.
5. These primary branches are called segmental arteries.
6. The kidney can be divided into five segments on the basis of their distribution.
7. Segmental arteries are the end arteries and supply renal vascular segments.
8. The anterior division passes in front of the renal pelvis.
9. They are distributed to different segments or areas of the kidney.
10. Lobar arteries arise from each segmental artery. Before entering the renal substance, each lobar artery gives off 2 or 3 interlobar arteries.
11. The interlobar arteries run toward the cortex on each side of the renal pyramid.
12. At the junction of the cortex and the medulla, the interlobar arteries give off the arcuate arteries, which arch over the bases of the pyramids.
13. The arcuate arteries give off several interlobular arteries that ascend in the cortex.
14. The afferent glomerular arterioles arise as branches of the interlobular arteries.
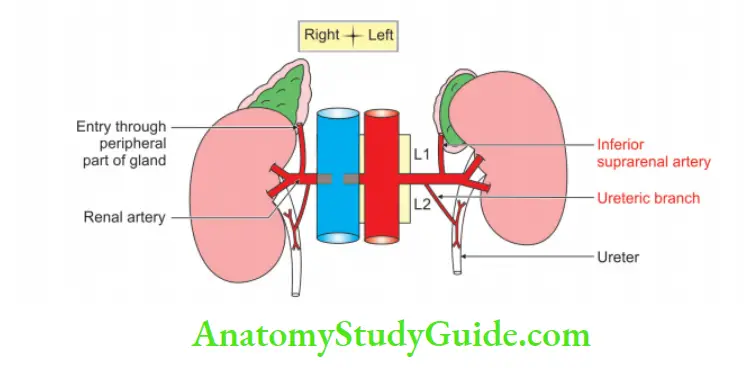
15. Other branches of renal artery: Each renal artery gives off
- Suprarenal branch to the suprarenal gland, and
- Ureteric branch to the upper end of ureter.
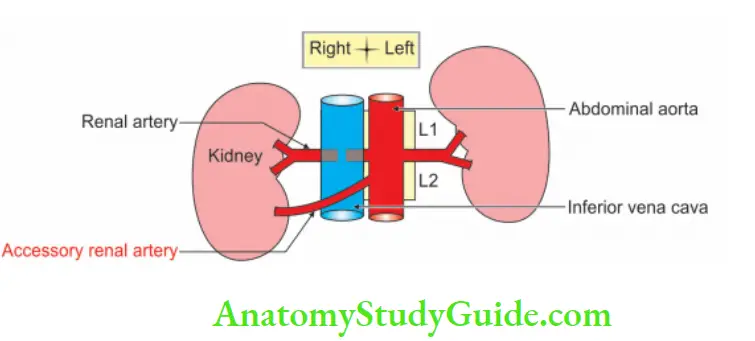
- 1 or 2 accessory renal arteries arise frequently from the aorta, above or below the main artery.
4. Posterior Abdominal Wall Applied Anatomy
1. The aberrant renal artery is usually due to failure to regress one of the arteries as the kidney ascends.
2. The aberrant artery entering the lower pole may cause compression of pelvic ureteric junction producing hydronephrosis.
3. Sometimes, the aberrant artery is the sole supply of one vascular segment of the kidney.
4. Ligature of a segmental or of an aberrant artery will cause ischemia and death of the corresponding segment of the kidney.
5. Sometimes an extra or ectopic renal artery may compress the superior end of the ureter, causing obstruction of urinary flow.
- As renal arteries are end arteries, the surgeon will 1st compress the anomalous artery before tying it.
- This is to assess whether such ligation will excessively impair circulation to the kidney.
- If so, an artificial arterial bypass graft may be attempted.
- Renal artery stenosis causes ischemia of the kidney which releases renin and cause hypertension.
6. For transplantation, the renal artery is anastomosed to the internal or external iliac artery and the renal vein to the external iliac vein.
7. The amount of blood circulating through the renal cortex is about 4 or 5 times more than that of the medulla.
8. But the blood flow may be reversed in crushing injuries due to the vasoconstriction of the interlobular arteries at the junction of the outer two-thirds and inner one-third of the cortex.
Middle Suprarenal Artery
Middle Suprarenal Artery Introduction:
It is a small artery of the suprarenal gland.
1. Middle Suprarenal Artery Origin
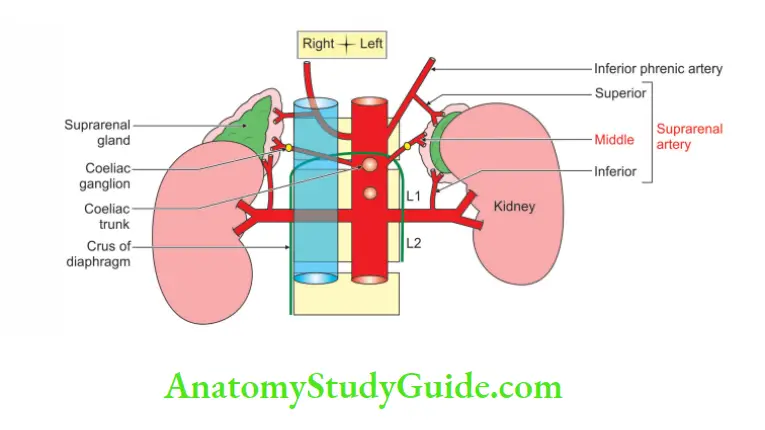
The paired suprarenal arteries arise from the abdominal aorta, between paired inferior phrenic and paired renal arteries at the level of the superior mesenteric artery.
2. Middle Suprarenal Artery Course And Relations
1. They run laterally across the crura of diaphragm to enter the suprarenal glands.
2. Here they anastomose with the suprarenal branches of the phrenic and renal arteries.
3. The right middle suprarenal artery passes behind the inferior vena cava, near the right coeliac ganglion.
4. Here it lies between the right crus of diaphragm and the inferior vena cava.
5. Right middle suprarenal artery is frequently multiple.
6. The left middle suprarenal artery passes close to the left coeliac ganglion, splenic artery and the superior border of the pancreas.
7. It lies behind the posterior wall of the lesser sac.
3. Middle Suprarenal Artery Applied Anatomy
1. Bilateral adrenalectomy was sometimes performed in certain inoperable mammary or prostatic cancer patients.
2. The right suprarenal gland is more difficult to explore because of its close proximity to the liver and its retro-vena caval position.
3. It is difficult to ligate right middle suprarenal artery as it courses behind the vena cava.
Testicular Artery
Testicular Artery Introduction:
Testicular arteries, as the name suggests, supply the testes. They are one of the most important of the lateral branches.
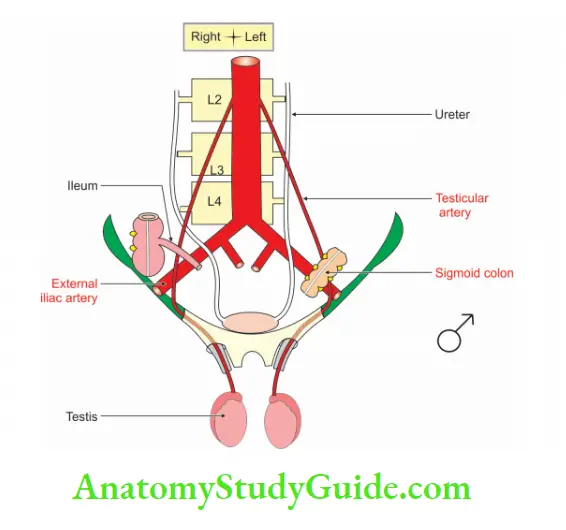
1. Testicular Artery Origin
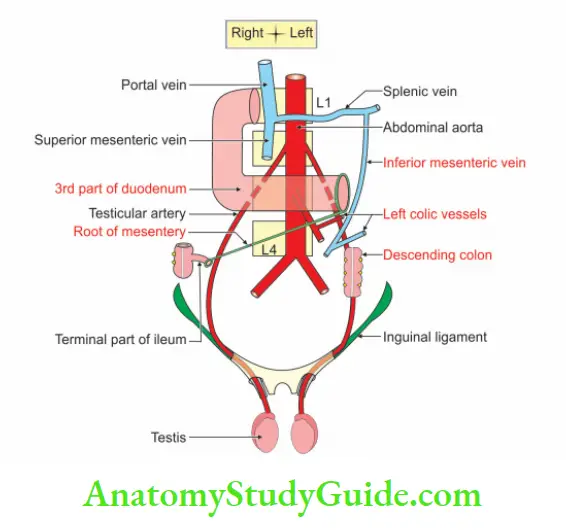
They are long and slender arteries, arising from the abdominal aorta just below the renal arteries and well above the inferior mesenteric artery.
2. Testicular Artery Courses and Relations
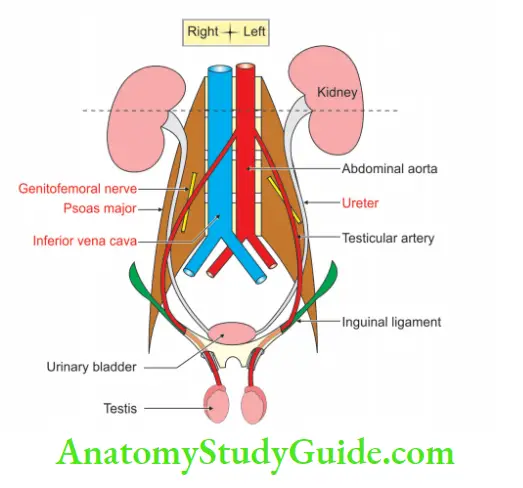
1. They have a long intra-abdominal course.
2. They course retroperitoneally.
3. They descend obliquely downwards and laterally.
4. They run lateral to the inferior epigastric vessels.
5. Traverse the deep inguinal canal and passes as one of the structures of spermatic cord.
6. Testicular arteries do not enter the pelvis.
7. Within the cord, testicular arteries lie anterior to the ductus deferens.
8. They reach the posterosuperior aspect of the testes and divide into
- Medial, and
- Lateral branch on the respective surfaces.
9. They pass through the tunica albuginea and ramify in the tunica vasculosa.
10. Terminal branches enter the testis over the surface.
11. Some pass into the mediastinum testis and loop back before reaching their distribution.
12 . In the abdomen, the testicular artery supplies
- Perirenal fat
- Ureter, and
- Iliac lymph nodes.
13. In inguinal canal, they supply cremaster.
14. In the epididymis, they anastomose with the artery to the vas, a branch of inferior vesical artery.
Relations of testicular artery:
3. Testicular Artery Applied anatomy
1. Torsion of the testis is a rotation of the testis and the spermatic cord within the scrotum.
2. Bell-clapper deformity is a predisposing factor in testicular torsion.
- In this condition, the tunica vaginalis joins high on the spermatic cord.
- It leaves the testis free to rotate.
3. Torsion commonly occurs in active young men and children and is accompanied by severe pain.
4. If not treated quickly, the testicular artery may be occluded. It is followed by necrosis of the testis.
5. Occlusion of the testicular artery within the abdomen usually does not affect blood supply to the organ.
6. Interruption of the artery in the inguinal or scrotal region causes infarction of the testis because of the involvement of both testicular arteries.
7. Compression of testicular vessels leads to ischaemic necrosis of the testis.
8. In about 80% of cases, failure to diagnose and intervene immediately can result in the loss of testis.
9. During the later decades of life, some of the scrotal vessels are seen to supply the testes; as a result, the spermatic cord may usually be divided without causing necrosis of testis.
10. In the region of the epididymis, there is an anastomosis between the testicular artery and the artery to the vas.
11. The artery to the vas is too small to sustain the testis, if the testicular artery is divided.
12. Treatment of varicocele is ligation of the veins of the pampiniform plexus above the inguinal ligament at the neck of the scrotum.
13. If the testicular artery is tied close to the testis, it will be completely devoid of the arterial supply.
14. There is communication between testicular artery and artery to vas and cremaster.
15. If the tie is away from the testis, then it will receive blood from artery of vas and cremaster.
Common Iliac Arteries
Common Iliac Arteries Introduction:
They are arteries of lower parts of the anterior abdominal wall, pelvis and lower limb. They are asymmetrical.
1. Common Iliac Arteries Origin
They are the two terminal branches arising from the abdominal aorta opposite the centre of the body of the 4th lumbar vertebra.
They are a finger’s breadth to the left of the middle line. Left common iliac artery is short. It is 4 cm long. However, the right common iliac artery is 5 cm long.
2. Common Iliac Arteries Course And Relations
1. Each common iliac artery at once diverges from the other and runs laterally downward.
2. The relations can be grouped as
- Anterior
- Posterior
- Lateral, and
- Medial.
Anterior relations: Anterior relations of the common iliac artery are covered anteriorly by peritoneum that separates them from the coils of small intestine.
1. Please note that ureters are the important anterior relations on the respective side of common iliac artery. They cross at the bifurcation of common iliac artery.
2. The other structures on anterior surface of both common iliac arteries are
- One-half of the aortic sympathetic plexus
- Coils of intestine
- Hypogastric nerves, and
- Lumbar splanchnic nerves.
3. It may be noted here that superior mesenteric vessels which continue as superior rectal vessels, and the apex of sigmoid mesocolon are structures related only to the left common iliac artery.
Posterior relations: Each artery rests upon the lower 1/2 of the body of the 4th and the whole of the 5th lumbar vertebra, as well as the disc above and below the latter, and the ganglionated sympathetic trunk.
The right common iliac artery has three posterior veins:
1. They are left and right common iliac veins and the inferior vena cava. However, the left common iliac artery has only left common iliac vein as posterior relation.
2. Lying deeply behind each artery in the lumbosacral are the obturator nerve, lumbosacral trunk, and between them lies the iliolumbar artery.
Lateral relations:
They are from above downwards.
- Inferior vena cava
- Right common iliac vein
- Psoas major, and
- Genitofemoral nerve.
Medial relations:
They are from below upwards
- Right common iliac vein
- Left common iliac vein, and
- Hypogastric sympathetic plexus.
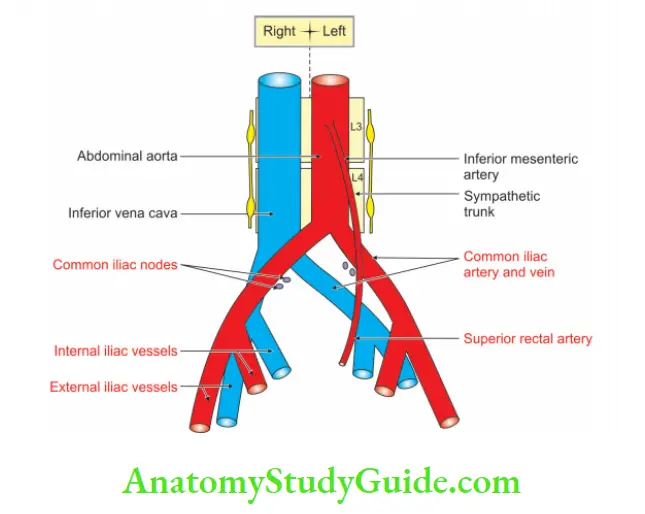
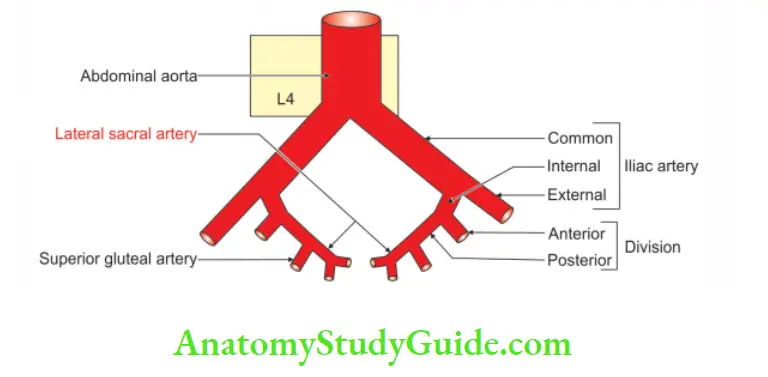
3. Common Iliac Arteries Branches
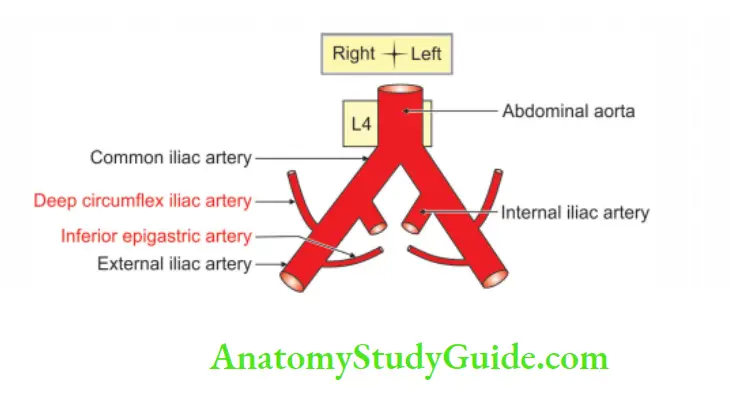
Each common iliac artery terminates by dividing into the larger external and smaller internal iliac arteries.
The division occurs at the level of L5 and S1 and in front of sacroiliac joint. It also gives small branches to the
- Peritoneum
- Psoas major
- Ureter
- Adjacent nerves, and
- Surrounding areolar tissue.
4. Common Iliac Arteries Applied Anatomy
1. Among all the structures, a surgeon needs to remember that ureters cross the common iliac artery from the front.
2. This piece of information helps the surgeon identify the ureter during the operation.
3. Pressure of right common iliac artery may bring partial obstruction to venous flow of left common iliac vein.
4. It results in varicosity of left leg.
5. We know that varicosity usually is a bilateral condition.
6. Hence, varicosity of left leg points the diagnosis of varicosity due to pressure of right common iliac artery.
7. In case of ligation of common iliac artery, blood supply to the lower limb of the respective side is maintained by anastomosis between superior and inferior epigastric artery.
External Lliac Artery
1. It is one of the two terminal branches of the common iliac artery, given at sacroiliac joint. It continues as a femoral artery at the mid-inguinal point deep into the inguinal ligament.
2. Peculiarities.
Descending colon ends and the sigmoid colon begins in front of the left external iliac artery at the level of pelvic brim.
The inferior epigastric artery, branch of the external iliac artery, is usually a significantly larger artery; it provides dominant blood supply to rectus abdominis.
It forms an important pathway for collateral circulation between vessels above and vessels below the diaphragm.
3. Termination: External iliac artery continues as femoral artery distal to inguinal ligament.
Relations of External Iliac Artery
1. Relations Of External Iliac Artery Anterior relations
1. The artery is covered by the parietal peritoneum and extraperitoneal areolar tissue.
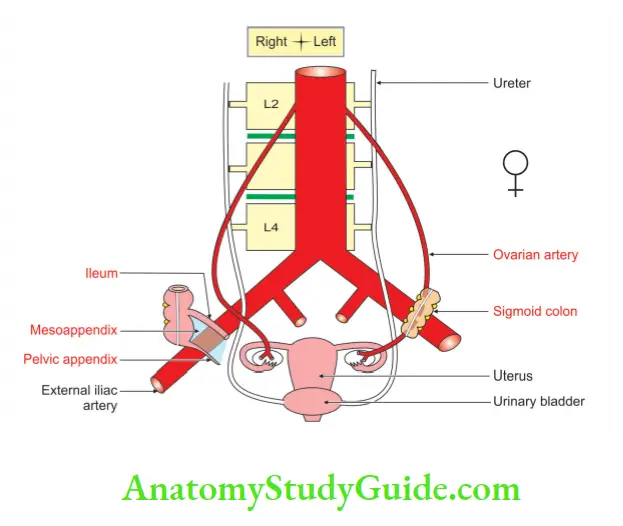
2. The right external iliac artery at its commencement is crossed by the terminal part of the ileum, and sometimes by the vermiform appendix.
3. The left external iliac artery at its commencement is crossed by the pelvic colon.
4. The left limb of the mesocolon of inverted V is attached along the upper half of the left external iliac artery.
5. Each external iliac artery may be crossed by the ureter, if it does not cross bifurcation of the common iliac artery.
6. Both arteries are crossed superiorly by the ovarian vessels in females ♀ and testicular vessels in males ♂.
7. The h as deferens’ in males ♂ and round ligament of uterus in females ♀ arch over external iliac artery from lateral to medial aspects.
8. Above the inguinal ligament, external iliac artery is crossed by genital branch of the genitofemoral nerve.
9. It is to be noted here that genitofemoral nerve and the femoral branch of genitofemoral nerve run along the lateral side of the external iliac artery.
10. Near the inguinal ligament, each vessel is crossed by deep circumflex iliac vein.
11. The external iliac lymph nodes lie along the artery.
2.Relations Of External Iliac Artery Posterior relations
1. The artery rests upon the iliac fascia at the pelvic brim, except for a little way above the inguinal ligament, where it lies upon the psoas muscle.
2. The right external iliac artery, at the commencement, has its external iliac vein behind it at a short distance.
Branches Of External Iliac Arteries
It gives two branches
- Inferior epigastric artery, and
- Deep circumflex iliac arteries.
Both are intimately related to the anterior abdominal wall.
Inferior Epigastric Artery
1. Inferior Epigastric Artery Origin
It is one of the two collateral branches of external iliac artery.
2. Inferior Epigastric Artery Course and Relations
- It lies medial to the deep inguinal ring and ascends medially upwards.
- Here it is hooked laterally by the ductus deferens in males ♂ and round ligament of uterus in females ♀.
- It crosses arcuate line, which is curved and sharp like a sickle and can injure itself.
- It pierces the transversalis fascia and enters rectus sheath.
- It anastomoses with the superior epigastric artery.
3. Inferior Epigastric Artery Branches
They are grouped inside and outside the rectus sheath
The branches inside the sheath are:
- Muscular supplying rectus abdominis, and
- Cutaneous supplying skin over the muscle.
The branches outside the sheath are:
- Cremasteric branch, and
- Pubic branch.
The cremasteric branch: Cremasteric branch enters through the deep inguinal ring and supplies the coverings of the spermatic cord in males ♂ and round ligament of uterus in females ♀.
Pubic branch: Pubic branch anastomoses with the pubic branch of the obturator artery. When the pubic branch of inferior epigastric artery is large, it is called abnormal obturator artery.
2. Deep circumflex iliac Artery
1. Deep circumflex iliac Artery Origin
It is a lateral branch of the two terminal branches of the external iliac artery.
2. Deep circumflex iliac Artery Course And Relations
1. It runs above the inguinal ligament, almost in the opposite direction.
2. It runs laterally and upwards along the back of inguinal ligament towards the anterior superior iliac spine.
3. It pierces the fascia transversalis, and continues along the iliac crest, up to its middle where it pierces the transversus abdominis.
4. It enters the interval between the transversus and the internal oblique muscles.
5. It supplies the muscles of lower abdomen.
6. At the anterior superior iliac spine, it anastomoses with the superior gluteal, the lateral circumflex femoral and superficial circumflex iliac arteries.
7. Just behind the anterior superior iliac spine, it gives off an ascending branch which runs upwards in the neurovascular plane.
3. Deep circumflex iliac Artery Applied Anatomy
1. The abnormal obturator artery is often called “artery of death” by surgeons.
2. During the operation for strangulated femoral hernia, it may be injured while cutting the lacunar ligament.
3. Inferior epigastric artery is a guide to identify the deep inguinal ring.
4. Inguinal hernia, medial to inferior epigastric artery, is direct inguinal hernia and lateral to it is indirect inguinal hernia.
5. The external iliac artery is intimately related to deep inguinal ring and may be damaged in the extensive medial dissection of the deep inguinal ring particularly during hernial repair.
6. This is very much true when the operation is performed in preperitoneal plane.
7. Disease of the right external iliac artery results in adhesion with the corresponding vein.
8. The walls of the vessels may get fused, making the dissection hazardous.
9. Rupture of the inferior epigastric artery occurs during a forceful bout of cough, a strong muscular contraction and a blow on the anterior abdominal wall in pregnant women.
10. It forms a tense painful swelling at the lateral border of the rectus abdominis muscle (rectus sheath haematoma).
11. It is important to remember that bleeding from the inferior epigastric artery can be disastrous as large quantity of blood gets collected in the closed space.
12. The incision at McBurney’s point for appendicitis is likely to damage the ascending branch of the deep circumflex iliac artery.
Superior Vesical Artery
Superior Vesical Artery Introduction: Superior vesical artery is the first large branch of the anterior trunk of internal iliac artery.
1. Superior Vesical Artery Origin
It arises as the 1st large branch of the anterior trunk of internal iliac artery. It is at the level of the upper border of the pubis.
2. Superior Vesical Artery Development
It is the persistent, proximal, patent part of the fetal umbilical artery.
3. Superior Vesical Artery Course And Relations
- It lies on the lateral wall of the pelvis just below the pelvic brim.
- It runs anteroinferiorly medial to the posterior surface of the pubis.
- The artery is crossed by the ductus deferens.
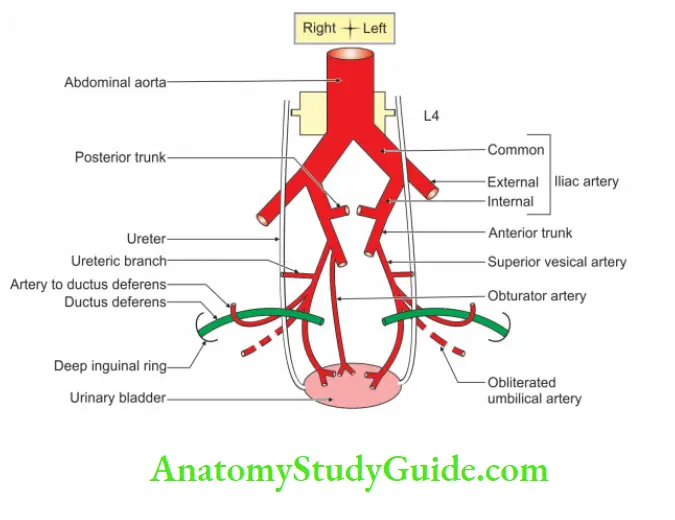
4. Superior Vesical Artery Distribution
1. It supplies to the upper portion of the bladder.
2. It anastomoses with the vesical branch of the
- Obturator
- Prostatic, and the
- Inferior vesical of the same side, and
- Superior vesical of the opposite side.
5.Superior Vesical Artery Branches
- Urachal to the medial umbilical ligament, and
- Ureteric to the lower end of the ureter. It also supplies to the seminal vesicles.
6. Superior Vesical Artery Fate
The distal part of superior vesical artery becomes obliterated to form medial umbilical ligament.
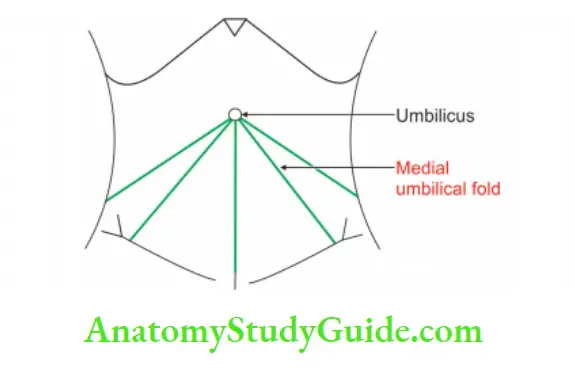
Name that betrays: Medical umbilical ligament does not function as ligament.
7. Superior Vesical Artery Applied Anatomy
Damage to the medial umbilical ligament below the level of the apex of the bladder should be avoided. It may cause gangrene of the bladder.
Lateral Sacral Artery
1. Lateral Sacral Artery Origin
Lateral sacral arteries are the branches of posterior division of internal iliac artery. They are usually two in number.
- Superior and
- Inferior
2. Lateral Sacral Artery Course And Relations
- The course downwards and medially to the front of the lateral mass of the sacrum.
- They pass in front of the pyriformis and sacral nerves.
- Both arteries lie upon the sacrum lateral to the anterior sacral foramina.
- The superior is confined to the region of the 1st two foramina.
- The inferior descends lateral to the sympathetic trunk as low as the coccyx.
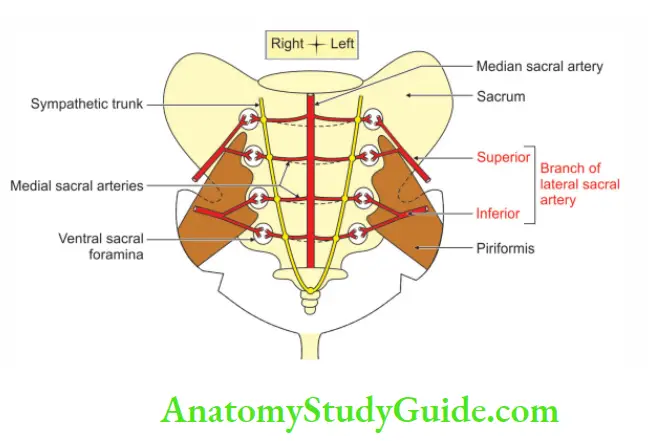
3. Lateral Sacral Artery Anastomosis
They anastomose with the median sacral artery.
4. Lateral Sacral Artery Distribution
They are distributed to the pyriformis and sacral nerves.
5. Lateral Sacral Artery Branches
- They give spinal branches.
- They enter the anterior sacral foramina and reach the sacral canal to supply its contents.
- Before entering the sacral canal, each spinal branch gives off a posterior branch.
- It emerges through the posterior sacral foramen.
- It anastomoses with branches of the superior and inferior gluteal and internal pudendal arteries.
- The lateral sacral arteries anastomose with each other and with the median.
Tributaries Of Inferior Vena Cava
Tributaries of inferior vena cava.
1. Common iliac vein
2. 3rd and 4th lumbar veins
3. Right
- Gonadal vein
- Renal vein
- Suprarenal vein
4. Hepatic veins are three large and many small veins directly open into inferior vena cava.
Question – 2: Describe inferior vena cava under following heads
1. Gross anatomy
2. Development, and
3. Applied anatomy.
Answer:
Inferior vena cava Introduction:
It is the systemic vein draining the venous blood from the structures present below the diaphragm.
1. Inferior vena cava Gross anatomy
Formation: It is formed by the union of
- Right common iliac vein.
- Left common iliac vein.
Level of formation: It is formed on the right side of body of 5th lumbar vertebra.
Termination: It opens into the lower and posterior part of right atrium and guarded by valves.
Dimensions:
- Breadth: 1”
- Length: 9”
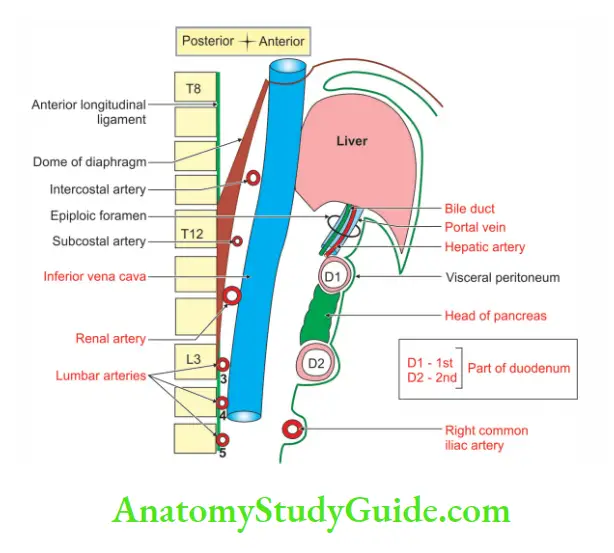
Inferior vena cava Relations:
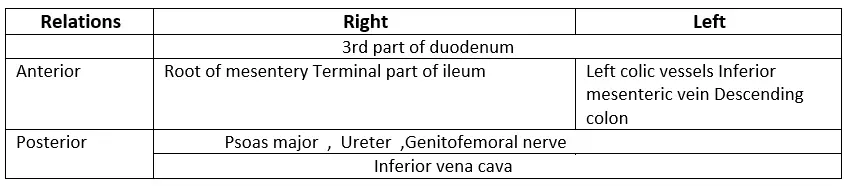
1. Inferior vena cava Anterior: From above downward, it is related to
- Posterior surface of liver
- Epiploic foramen
- 1st part of duodenum
- Portal vein
- Head of pancreas
- 3rd part of duodenum
- Right gonadal artery
- Parietal peritoneum
- Root of mesentery
- Right common iliac arteries.
2.Inferior vena cava Posterior:
Lower part:
- Bodies of lumbar vertebrae
- Anterior longitudinal ligament
- Right , Psoas major muscle , Sympathetic trunk
- 3rd and 4th lumbar arteries
Upper part:
1. Right:
- Crus of the diaphragm
- Coeliac ganglion
- Renal artery
2. Part of suprarenal gland
3. Middle suprarenal artery
4. Inferior phrenic artery
3. Right side:
- Right ureter
- 2nd part of duodenum
- Medial border of right kidney
- Hepatorenal pouch of Morison, and
- The bare area of the liver.
4. Left side:
- Abdominal aorta
- Right crus of the diaphragm
- Cisterna chyli
- Thoracic duct
- Omental bursa and
- Caudate lobe of liver.
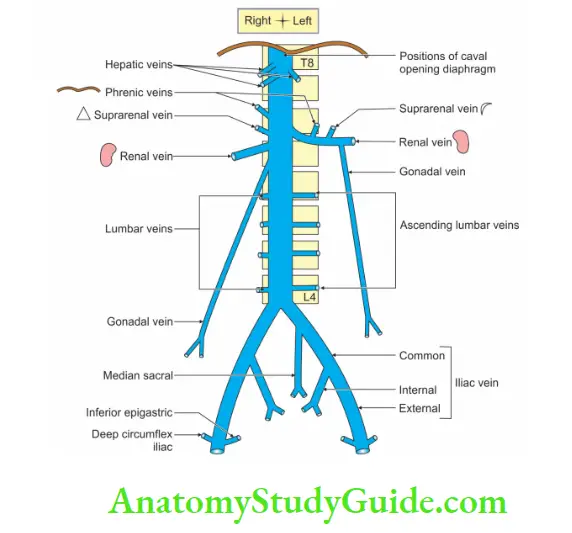
Tributaries
The tributaries of vena cava are not identical with the branches of the abdominal aorta.
Particularly, there is no corresponding to the three ventral branches to the gut.
Following are the tributaries of the inferior vena cava
Pair of veins:
- Common iliac
- Renal
- Phrenic
- Lumbar veins.
3rd and 4th pair of lumbar veins drain directly into the inferior vena cava.
Unpaired veins:
- Right gonadal vein.
- Right suprarenal vein and hepatic veins.
- Odd to remember
Odd to remember:
Note: 1st and 2nd lumbar veins drain into ascending lumbar veins.
2. Development
Chronological age: It develops in the 8th week of intrauterine life.
Germ layer: Mesoderm.
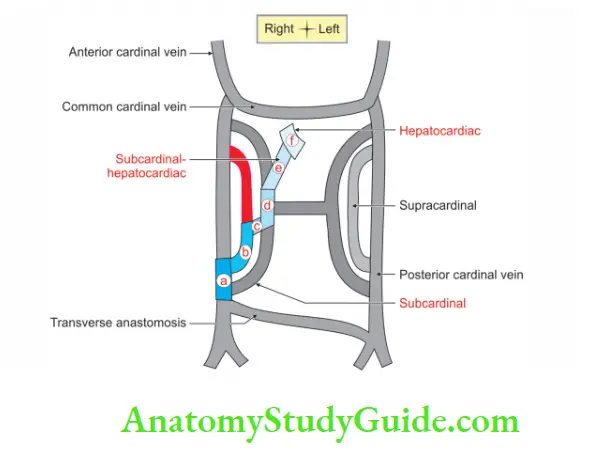
Sources: It is a composite vessel. It is developed from the following sources from below upwards.
“a” From the persistent caudal part of right posterior cardinal vein (between its junction with the supracardinal and anastomosis between the two posterior cardinals).
“b” From the lower part of right supracardinal vein (between its junction with the posterior cardinal and supracardinal subcardinal anastomosis). This part receives 3rd and 4th pairs of lumbar veins.
“c” From the anastomosis between right supracardinal and right subcardinal veins: This part receives right gonadal vein.
“d” From the upper part of right subcardinal vein: This part receives right supra-renal and both renal veins.
“e” From a new vessel: It develops behind the liver and communicates right subcardinal vein with common hepatic vein also called hepatocardiac channel.
“f” From the common hepatic vein: It is developed from suprahepatic part of right vitelline vein.
The post-renal segment of the vena cava lies on a more posterior plane than the pre-renal segment.
Anomalies:
- Double inferior venae cavae below the renal veins.
- Retrocaval ureter.
3. Applied Anatomy
1. In obstruction of inferior vena cava, a collateral circulation may be established.
2. The tributaries of superior and inferior venae cavae are communicated by a number of superficial and deep sets of veins.
3. Thrombosis in the inferior vena cava causes oedema of legs and back.
Cisterna Chyli
Cisterna Chyli Introduction:
It is dilated lymphatic sac.
1. Length: 5 cm
2. Site: In front of bodies of L1 and L2.
3. Tributaries
- Intestinal lymph trunk
- Right and left lumbar trunks.
Cisterna chyli:
1. Cisterna Chyli Gross anatomy
- It is an elongated lymphatic sac.
- Length: 5 to 7 cm.
- Situation: In front of the 1st and 2nd lumbar vertebrae, immediately to the right of the abdominal aorta.
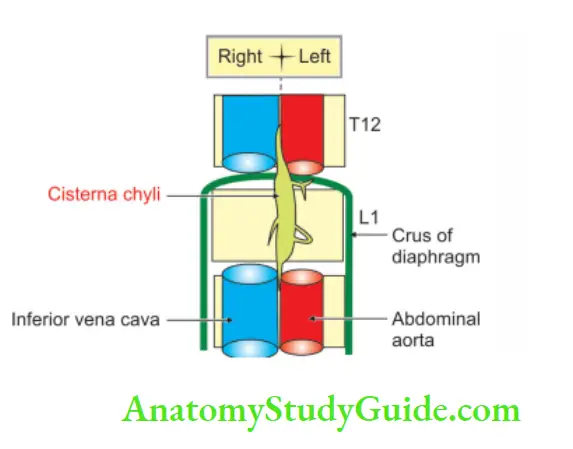
2. Cisterna Chyli Relations
Right:
- Right crus of the diaphragm
- Lumbar azygos vein
Left:
- Left crus of the diaphragm
- Abdominal aorta
- Coeliac trunk
- Superior mesenteric artery
Posterior:
- Anterior longitudinal ligament
- Bodies of L1 and L2
- An intervertebral disc between L1 and L2
3. Cisterna Chyli Tributaries
Right and left intestinal lymph trunks.
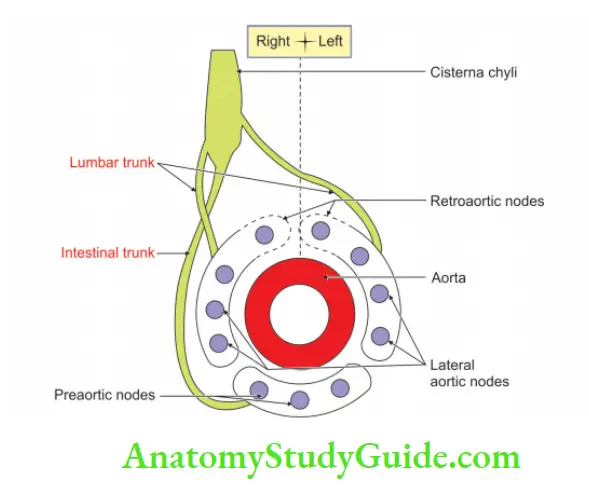
4. Cisterna Chyli Termination:
Its upper end continues as thoracic duct.
5. Cisterna Chyli Draining areas:
Intestinal trunk brings lymph from
- The stomach to intestine
- Pancreas
- Spleen
- Anteroinferior part of the liver
- All structures below diaphragm (lower half of the body).
6. Cisterna Chyli Applied Anatomy
1. Thoracic duct when obstructed due to filarial infestation or growth will give rise to chylothorax, chyluria, etc.
2. Thoracic duct when damaged during operation in the neck the lymph usually follows another chann
Leave a Reply