Question 1: Describe investing layer of deep cervical fascia under the following heads:
1. Investing Layer Of Deep Cervical Fascia Attachments
2. Investing Layer Of Deep Cervical Fascia Features
3. Investing Layer Of Deep Cervical Fascia Applied anatomy
Table of Contents
It is connective tissue like a cervical collar. It keeps all the structures of the neck in position.
1. Investing Layer Of Deep Cervical Fascia Attachments
1. Superiorly
- External occipital protuberance
- Superior nuchal line
- Mastoid process
- Base of mandible
2. Inferiorly
- Spine of scapula
- Acromion process
- Clavicle
- Manubrium.
Read And Learn More: Neck Anatomy Notes And Important Questions With Answers
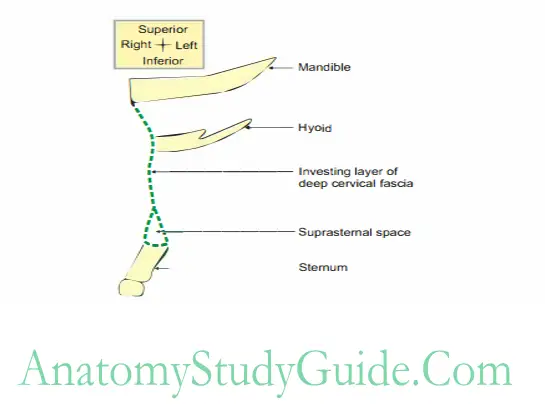
3. Anteriorly
- Symphysis menti
- Hyoid bone
- Oblique line of thyroid cartilage.
Deep Cervical Fascia Features
Thickness varies
It is thick over.
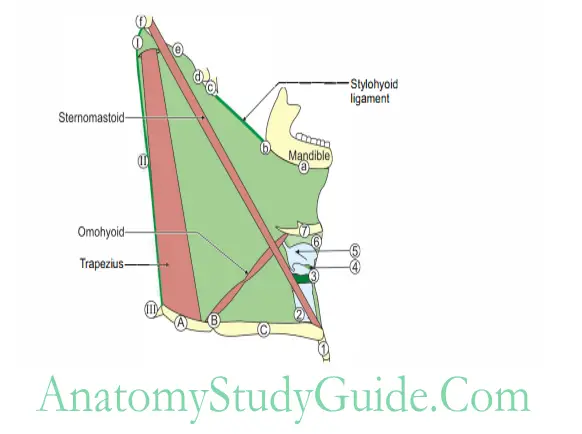
Route of tracings of attachment of investing layer of deep cervical fascia
Anterior inferior- anterior superior- posterior superior – posterior inferior- anterior inferior
Deep Cervical Fascia Anteroinferior
1. Manubrium sternum
2. Trachea
3. Cricoid cartilage
4. Cricothyroid membrane
5. Oblique line of thyroid cartilage
6. Thyrohyoid membrane
7. Body of hyoid bone
Deep Cervical Fascia Superior
1. Base of mandible
2. Angle of mandible
3. Styloid process
4. Mastoid process
5. Superior nuchal line
6. External occipital protuberance
Deep Cervical Fascia Posterior
1.External occipital crest
2. Ligamentum nuchae
3. Spine of 7th cervical vertebra
Deep Cervical Fascia Inferior
1.Spine of scapula
2. Acromioclavicular joint
3. Clavicle
- Over parotid gland, called parotid fascia.
- Between styloid process and angle of mandible called stylomandibular ligament.
1.It is thin on
- Styloid process,
- Mandible, and
- Tympanic plate.
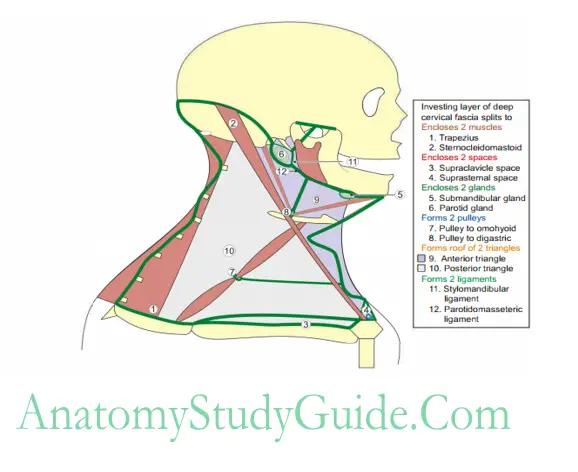
Investing Layer Of Deep Cervical Fascia
Magic of “2”
- Encloses 2 muscles
Trapezius and
Sternocleidomastoid. - Encloses 2 Salivary glands
Parotid and
Submandibular. - Forms 2 laminae
Pretracheal and Prevertebral. - Forms roof of 2 triangles
Anterior and Posterior. - Forms 2 spaces
Suprastemal and Supraclavicular. - Forms 2 structures
Exam-Oriented Anatomy
Stylomandibular ligament and Parotidomasseteric fascia. - Forms 2 slings
Intermediate tendon of digastric and Omohyoid.
Deep Cervical Fascia Applied anatomy
Ludwig’s angina: It is a . .ar swelling primarily due to infection of the submandibular with sublingual and submental space.
It is limited laterally by two halves of mandible and posteriorly by hyoid bone.
This is because of the attachments of investing layer of deep cervical fascia to the base of mandible and hyoid bone.
Collar stud abscess: The abscess is formed deep to deep fascia. The main cause is tuberculosis of deep cervical lymph nodes.
It leads to caseation of lymph nodes.
The abscess accumulates in deeper layer and penetrates deep fascia and points in the superficial layer called collar stud abscess.
Mumps: Viral infection of the parotid gland is called mumps.
The fascia over parotid gland is thick and closely adherent.
The inflammation or abscess of the gland does not have space for expansion.
The capsule is stretched and the nerves are stimulated. Hence, the infection of the parotid gland is painful.
Applied anatomy of Deep Fascia of Neck
1. The investing layer of deep cervical fascia is fixed to hyoid bone.
Any collection of blood, pus, serum or abscess in the subcutaneous tissue of the suprahyoid area does not descend below the hyoid bone.
2. Pus collected from caries of cervical vertebrae may travel
Axillary sheath: First it appears in the axilla and then in the arm.
Pharyngeal wall: It travels in the superior mediastinum and appears as a midline swelling.
It is seen when the mouth is opened.
Investing Layer Of Deep Cervical Fascia
In the thorax: It presents as a swelling in the superior mediastinum.
3. Carotid sheath is frequently exposed in block dissection of the neck during surgical removal of deep cervical lymph nodes.
4. Whn the neck is extended, the carotid sheath retracts backwards.
Hence, suicidal attempt by sharp cutting weapons often fails to reach the carotid arteries.
5. Thyroid Swelling moves with Swallowing but does not Swift (move) on protrusion of tongue.
6. The abscess in the floor of mouth is drained by a deep incision below the mandible by dividing the mylohyoid muscle.
7. The blood vessels in the deep fascia do not contract and tend to bleed profusely.
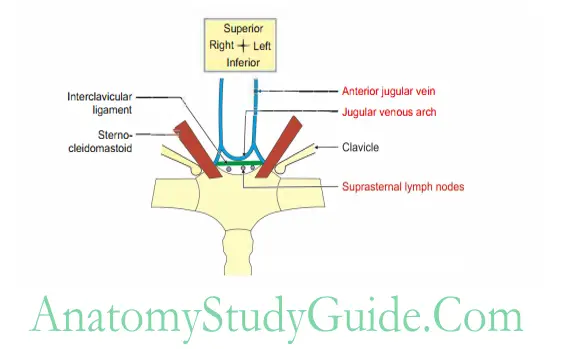
8. Injury in the suprastemal space of Bum ruptures anterior jugular vein and results into air embolism which may be fatal.
Suprasternal space (space of Burns)
Suprasternal space Introduction: It is the space above the sternum (Fig. 3.5).
1. Suprasternal space Formation: It is formed by two laminae of investing layer of deep cervical fascia
2. Suprasternal space Attachments: It is attached to anterior and posterior borders of jugular notch.
3. Suprasternal space Contents
- Muscles: Sternal heads of right and left stemomastoid.
- Veins
Jugular venous arch and
Anterior jugular vein - Suprasternal lymph nodes
- Interclavicular ligaments
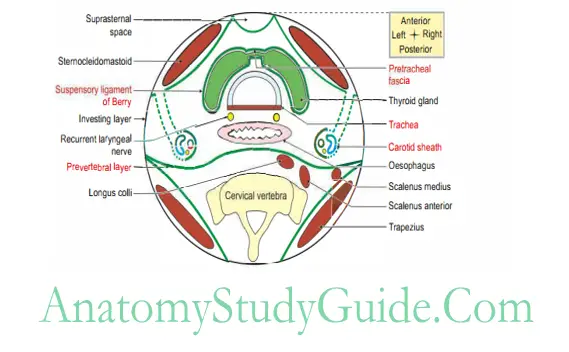
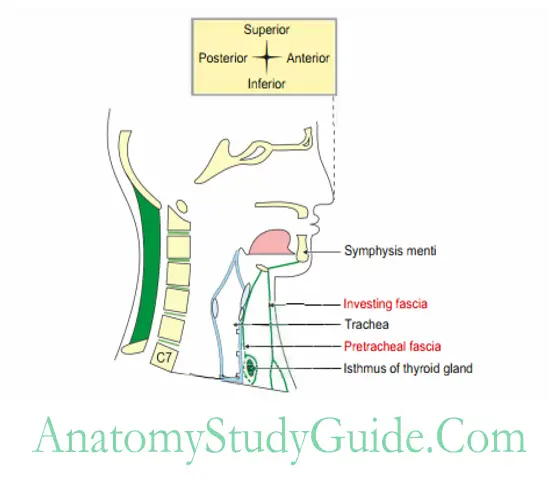
Pretracheal Fascia
The condensed deep cervical fascia in front of trachea is called pretracheal fascia.
1. Pretracheal Fascia Attachments
Superiorly
- Hyoid bone in the median plane,
- Oblique line of thyroid cartilage, and
- Cricoid cartilage, more laterally.
Investing Layer Of Deep Cervical Fascia
Inferiorly
- Below the thyroid gland, it encloses the inferior thyroid veins.
- It passes behind the brachiocephalic veins and finally blends with the arch of the aorta.
- On either side, it fuses with the carotid sheath deep to the sternomastoid.
2. Other features
- On either side, it sends septa which connect the thyroid gland to the cricoid cartilage and form a suspensory ligament of the throid gland.
- It is called ligament of Berry.
- Hence, the thyroid gland moves with deglutition.
- The ligaments are attached chiefly to the cricoid cartilage and may extend to thyroid cartilage.NEET
- It supports the thyroid gland and do not let it sink into the mediastinum.
- The capsule of the thyroid gland is very weak along the posterior borders of the lateral lobes.
- Hence, the thyroid gland can enlarge posteriorly and compress oesophagus and produces dysphagia.
3. Pretracheal Fascia Functions
The fascia provides a slippery surface for free movements of the trachea during Z swallowing.
It forms neurovascular sheath to carotid vessels.
Pretracheal Fascia Applied anatomy
- Thyroid swelling moves with swallowing but does not shift on protrusion of tongue.
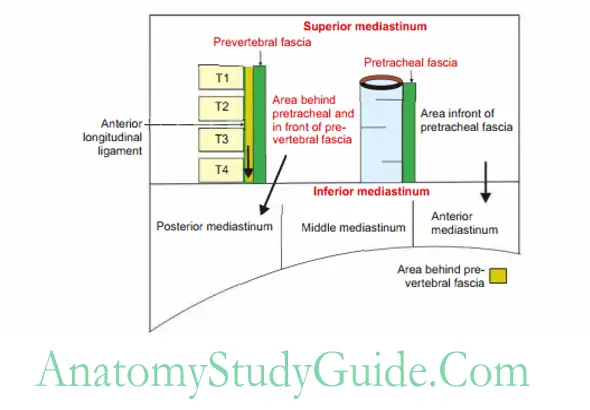
- The abscess present in front of pretracheal fascia descends in the anterior mediastinum.
- The abscess present behind the pretracheal fascia descends to the posterior mediastinum.
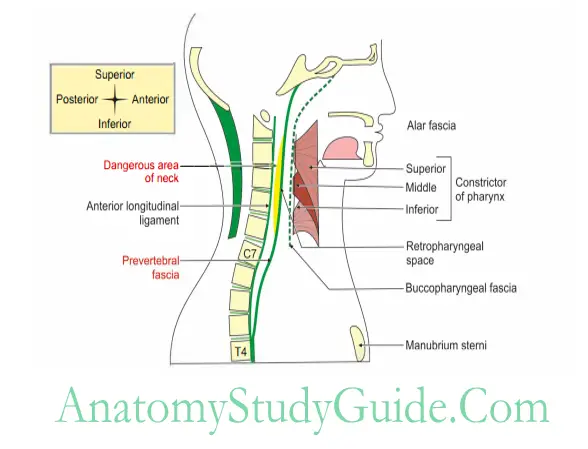
Prevertebral fascia
It is a deep fascia of neck, present in front or anterior to the cervical and 1st four thoracic vertebrae .
1. Prevertebral Fascia Attachments
- Superiorly: Base of skull.
- Posteriorly: Anterior longitudinal ligament of body of 3rd and 4th thoracic vertebrae.
- Laterally: Gets lost deep to trapezius.
2. Prevertebral Fascia Features
- It splits into anterior and posterior layers.
Anterior layer is called alar fascia. It fuses with buccopharyngeal fascia.
Posterior layer is firmly attached to anterior longitudinal ligament. - It encloses vertebral muscles.
- It forms the floor of posterior triangle.
- It contributes axillary sheath (cervicoaxillary canal).
(It does not invest subclavian and axillary veins which lie in the loose areolar tissue).
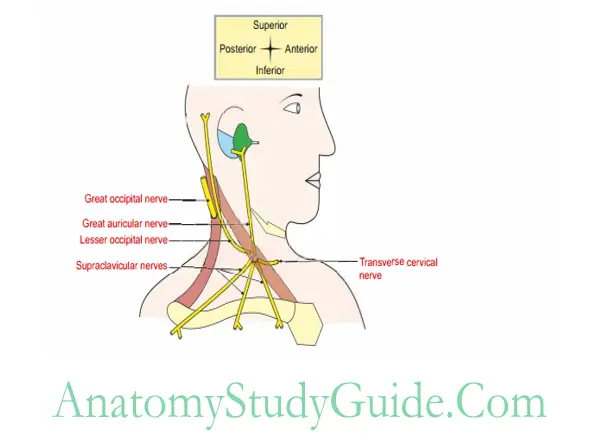
3. Prevertebral Fascia Structures piercing
- Great auricular nerve
- Lesser occipital nerve
- Transverse cervical nerve and
- Supraclavicular nerves.
4. Prevertebral Fascia Relations
- Anteriorly: Retropharyngeal space.
- Superficial
Accessory nerve (Xlth cranial nerve)
Lymph nodes of posterior triangle. - Deep
Muscles forming floor of triangle.
Cervical plexus.
Trunks of brachia! plexus.
3rd part of subclavian artery.
Investing Layer Of Deep Cervical Fascia
5. Prevertebral Fascia Functions: To provide a smooth base for gliding movements of pharynx, oesophagus and carotid sheath during movements of neck and during swallowing.
6. Prevertebral Fascia Applied anatomy
- There is dangerous area of the neck. It is bounded anteriorly by anterior layer of alar fascia and posteriorly by posterior layer of prevertebral fascia.
- The abscess formed behind the prevertebral fascia travel down into superior I mediastinum up to T3-T4.
- The abscess formed infront of prevertebral fascia travel to superior mediastinum and then the posterior mediastinum.
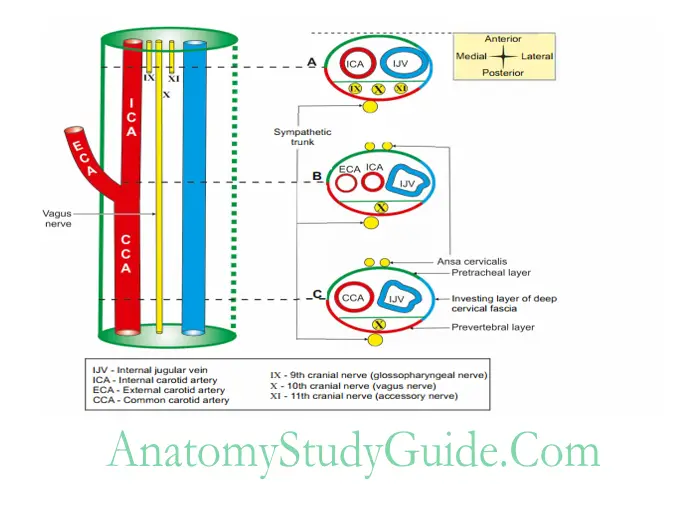
Carotid sheath
It is a condensation of deep cervical fascia around carotid artery and internal jugular vein.
1. Extent: It extends from base of skull to the arch of the aorta.
2. Formation: It is formed by all the layers of deep cervical fascia.NEET
- Anterior wall is formed by pretracheal fascia.
- Posterior wall is formed by prevertebral fascia, and
- Investing layer of deep cervical fascia.
3. Thickness: It is thick around artery and thin around vein to allow free expansion during increased venous return.
4. Relations
- Anteriorly: Ansa cervicalis within the wall of the sheath.
- Posteriorly: Sympathetic trunk behind the sheath.
5. Contents
- Internal carotid artery in the upper part of sheath.
- Common carotid artery in the lower part of sheath.
- Internal jugular vein behind the internal or common carotid artery.
- Vagus nerve posteriorly and in between artery and vein.
- Deep cervical lymph nodes.
6. Carotid Sheath Applied anatomy
- Carotid sheath frequently exposed in block dissection of the neck during surgical removal of deep cervical lymph nodes.
- Infection or inflammation of adjacent structures may involve carotid sheath. It
may produce symptoms of - Thrombosis of internal jugular vein.
Compression of 11th to 12th cranial nerves.
Carotid body tumour (potato tumour) arises from carotid body.
Investing Layer Of Deep Cervical Fascia
Question 2: Name the muscles forming floor of the posterior triangle.
1. Splenius capitis.
2. Levator scapulae.
3. Scalenus medius.
4. Semispinalis capitis-occasionally
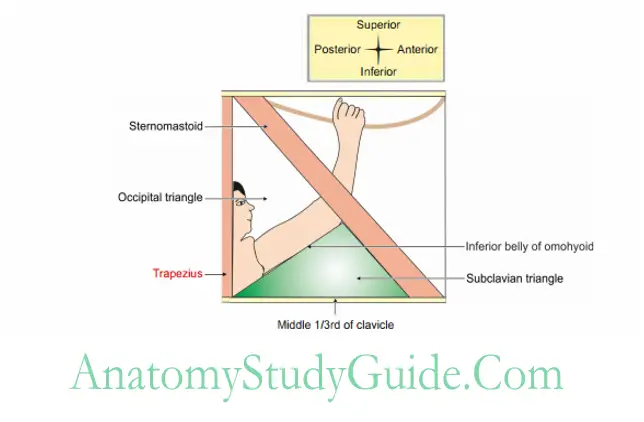
Question 3: Name the boundaries of posterior triangle of neck
1. Anteriorly: Posterior border of stemocleidomastoid.
2. Posteriorly: Anterior border of trapezius.
3. Base: Middle one-third of clavicle.
4. Apex: Meeting point of stemocleidomastoid and trapezius at superior nuchal line.
Question 4: Describe posterior triangle under the following headings:
1. Posterior Triangle Boundaries,
2. Posterior Triangle Subdivisions,
3. Posterior Triangle Roof,
4. Posterior Triangle Floor,
5. Posterior Triangle Contents, and
6. Posterior Triangle Applied anatomy.
1. Boundaries
- Anteriorly: Posterior border of stemocleidomastoid.
- Posteriorly: Anterior border of trapezius.
- Base: Middle one-third of clavicle.
- Apex: Meeting point of stemocleidomastoid and trapezius at superior nuchal line.
2. Subdivisions: It is subdivided by inferior belly of omohyoid into
- Occipital triangle
- Subclavian or supraclavicular triangle
3. Roof
- Skin.
- Superficial fascia.
- Investing layer of deep cervical fascia.
- Platysma forms the lower and anterior part of roof.
- Roof is pierced by
- Nerve: The arrow in front of nerves indicates the direction of nerves
- Lesser occipital,
- Great auricular,
- Transverse cutaneous nerve of neck,
- Supraclavicular nerves. –
- Veins: External jugular vein and its tributaries.
- Lymph vessels.
4. Floor: Mainly formed by 2nd layer of muscles of neck (above downwards). These muscles are carpeted by deep fascia of neck. They are grouped as
- Obliquely placed
Splenius capitis,
Levator scapulae, - Vertically placed
Scalenus medius, and
Scalenus posterior. - Muscles present occasionally are carpeted by prevertebral fascia.
Semispinalis capitis at the apex;
1st digitations of serratus anterior.
Note: Scalenus anterior usually does not form the floor. It is overlapped by the sternomastoid.
5. Contents: The spinal accessory nerve and the lymph nodes are the true contents of the posterior triangle and all others are behind or infront of the fascia! floor.
- Muscle: Inferior belly of omohyoid.
- Nerves
Accessory nerve: It is hooked by lesser occipital nerve.
The nerve divides the triangle into upper care free triangle and lower careful triangle.
Investing Layer Of Deep Cervical Fascia
The important structures lie below the spinal root of accessory nerve.
Roots, trunks of hrachial plexus and their hranches.
- Nerve to rhomboids.
- Nerve to serratus anterior.
- Nerve to subclavius.
- Suprascapular nerve.
- Muscular branches to
Scalenus muscles.
Longus colli.
Cervical nerves
- Greater occipital nerve emerges from the apex of the triangle and reaches scalp.
- Great auricular nerve.
- Lesser occipital nerve.
- Transverse cervical nerve of neck.
- Supraclavicular nerve.
- 3rd and 4th cervical nerves supplying trapezius.
Arteries
- Occipital artery, a dorsal branch of external carotid artery emerges from the apex of the occipital triangle.
- Transverse cervical artery is a branch of thyrocervical trunk (branch of 1st part of subclavian artery). It is one ofthe contents ofoccipital triangle. It divides into ascending and descending branches at anterior border of sternocleidomastoid.
- Suprascapular artery
- Transverse cervical artery has to reach anterior border of trapezius to distribute the same and to anastomose around scapula. It needs to travel through subclavian triangle.
Veins: External jugular vein and its tributaries.
- Transverse cervical
- Suprascapular
- Anterior jugular veins.
- Subclavian vein is lower down and is not included in the triangle.
Lymph nodes
- Supraclavicular lymph nodes are present along the posterior border of sternomastoid.
- Occipital lymph nodes.
Applied anatomy
- Left supraclavicular (Virchow’s) lymph nodes are enlarged inmalignancyof testis, stomach and other abdominal organs.
- The pressure in the external jugular vein can be recorded in the recumbent position.
It is increased in right-sided heart failure and in the obstruction of the superior vena cava. - The retropharyngeal abscess may extend in the lower part of posterior triangle.
- Spinal root of accessory nerve is the important content. It is plastered to the investing layer of deep fascia at the roof of triangle. Hence, a superficial incision to open a subcutaneous abscess at the posterior border of sternocleidomastoid should be made carefully to avoid injury to nerve.
- Sometimes nerve to subclavius gives a branch to join the phrenic nerve.
This is called accessory phrenic nerve.
In surgery of phrenic avulsion from the root of the neck, the accessory phrenic nerve, if present, might tear the subclavian vein with alarming symptom.
This is because the main trunk loops around the vessel.
The accessory phrenic nerve, branch of nerve to subclavius is an important nerve of unimportant muscle.
Subclavian steal syndrome: It takes place in obstruction of the subclavian artery proximal to the origin of vertebral artery.
The blood from the brain is diverted to the limb via subclavian artery.
Question 4: Describe the subclavian triangle under the following headings:
1. Boundaries,
2. Contents, and
3. Applied anatomy.
1. Subclavian Triangle Boundaries: A subclavian triangle is lower part of posterior triangle. It has following boundaries.
- Anteriorly by lower part of posterior border of sternocleidomastoid.
- Posteriorly by anterior border of inferior belly of omohyoid.
- Base by middle one-third of clavicle.
- Apex is meeting point of inferior belly of omohyoid with sternocleidomastoid
- Roof by
- Skin containing platysma,
- Superficial fascia,
- Investing layer of deep cervical fascia, and
- Structures piercing deep fascia. They are
- External jugular vein
- Supraclavicular nerve
- Unnamed cutaneous vessels and lymphatics.
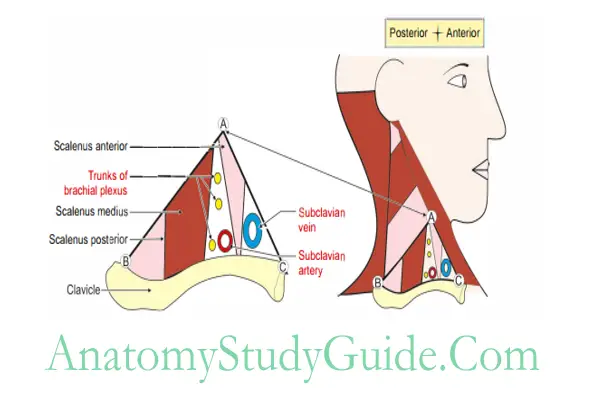
Floor contains
- 1st rib,
- Scalenus medius, and 1
- st digitation of the serratus anterior.
2. Subclavian Triangle Contents
- Third part of subclavian artery It curves laterally and downwards between the scalenus anterior and scalenus medius.
It runs along the brachial plexus.
It passes through the cervicoaxillary canal. - Dorsal scapular arter (branch of 3rd part of subclavian artery: This artery is also called descending scapular artery.
It passes laterally through or in front of brachial plexus. - Suprascapular artery (branch of thyrocervical trunk): It is one of the three branches of thyrocervical trunk.
It passes in front of Scalenus anterior and phrenic nerve and behind
Sternomastoid and internal jugular vein. - Superficial (transverse) cervcal arter (branch of thyrocervcal trunk): It crosses in front of phrenic nerve and scalenus anterior before it enters posterior triangle.
- Terminal part of external jugular vein: It pierces deep fascia and drain into subclavian vein.
- Trunks of brachia! plexus: The upper and middle trunks lie above and lower trunk lies below the 3rd part of subclavian artery.
- Branches of roots of brachia! plexus
Dorsal scapular nerve: It supplies rhomboids major and minor.
Long thoracic nerve: It supplies serratus anterior. - Branches from trunks of brachia! plexus
Nerve to subclavius: It supplies subclavius.
Suprascapular nerve: Near the posteroinferior angle, it accompanies suprascapular artery. It supplies supraspinatus and infraspinatus. - Supradavicular lymph nodes: These nodes also called posteroinferior group of deep cervical nodes. They drain
- Occipital region of scalp,
- Back of the neck,
- Axillary and
- Deltopectoral nodes of the superior extremity, and also the
- Upper deep cervical lymph nodes.
Note: Spinal accessory nerve and lymph nodes are the true contents of the posterior triangle as they lie between fascial roof and the floor of the triangle.
All others are either behind the fascial floor or in front of the fascial roof.
3. Subclavian Triangle Applied anatomy
- Subclavian triangle is an important clinical area for following reasons.
- It is better inspected from front but palpated from behind.
- The pulsations of the great veins may be seen, if the central venous pressure is raised.
The external jugular vein, a prominent feature, may be distended due to - Kinking,
- Raised venous pressure or
- Obstruction of the veins.
- Subclavian vein is used to keep the venous catheter for long-term intravenous injections.
- The subclavian artery can be felt pulsating as it crosses the 1st rib.
- The trunks of brachial plexus may be felt above and behind it. The brachial plexus block is given by injecting anaesthetic agent around the trunk just above the midpoint of clavicle.
- Troisier’s sign: Enlargement of the left supraclavicular lymph nodes in cancer of the stomach.
- The cancer of the lung and breast spreads to the supraclavicular nodes of the side of lesion.
Omohyoid
Omohyoid (omos-pertaining to shoulder)
1. Omohyoid Attachments
- Origin: Lateral part of inferior border of hyoid bone.
- Insertion
- Superior border of scapula
- Suprascapular ligament.
2. Omohyoid Features: It has
- Superior belly,
- Inferior belly, and
- Intermediate tendon.
The two bellies are pulled by fibrous pulley, a band of deep cervical fascia and attached to clavicle.
It divides the posterior triangle into two parts.
The part above the muscle is called occipital triangle and the part below the muscle is called subclavian triangle.
3. Omohyoid Nerve supply
- Superior belly: Superior root of ansa cervicalis.
- Inferior belly: Inferior root of ansa cervicalis.
4. Omohyoid Applied anatomy: It overlaps internal jugular vein near hyoid bone. Hence, it acts as a useful guide during operation of the underlying vein.
Great auricular nerve
1. Great auricular nerve Root value: Ventral ramus of C2 and C3 (branches for cervical plexus). C2 is more important. It is a large trunk passing obliquely upwards over sternocleidomastoid.
2. Great auricular nerve Distribution
Skin over
- Angle of mandible,
- Parotid gland,
- Lower and lateral surface of ear lobule,
- Mastoid region, and
- Skin of scalp posterior to ear.
Parotid fascia
3. Great auricular nerve Applied anatomy: It is palpable and visibly thickened in tuberculoid leprosy.
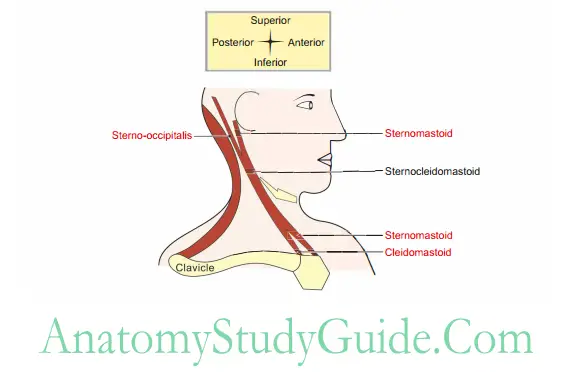
Sternocleidomastoid
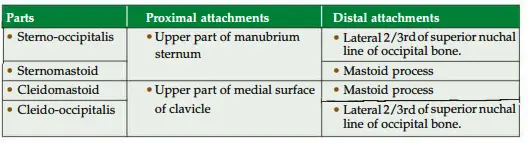
1. Sternocleidomastoid Relations
- Superficial: Skin containing
Cutaneous nerves
Great auricular,
Transverse cervical, and
Medial supraclavicular. - Vein: External jugular vein
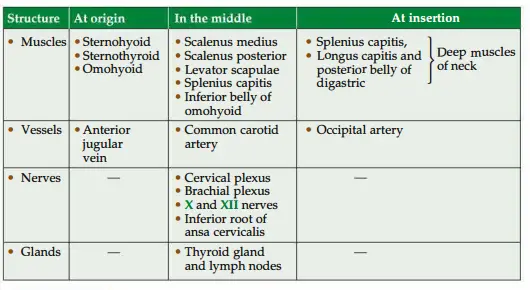
Sternocleidomastoid Deep
2. Sternocleidomastoid Nerve supply
- Motor: Spinal root of accessory nerve (11th cranial nerve).
- Proprioceptive: 2nd and 3rd ventral rami of cervical nerves.
3. Sternocleidomastoid Action
- The chief purpose of the muscle is to protract the head (it is a combination of flexion of cervical spine and extension of atlantoaxial joint simultaneously).
Protraction is brought by the contraction of muscles of both sides. - Contraction of muscle of one side tilts the head towards the same side of shoulder and turns the chin towards the opposite side.
- Testing of the muscle
The chin is turned to the opposite side against resistance. The muscle of one side is palpated.
The chin is bent downwards to test the sternocleidomastoid of both sides.
Sternocleidomastoid Applied anatomy
- Congenital torticollis: During difficult labour, undue pulling of the head of the baby causes tearing of the fibres of the sternocleidomastoid.
The subsequent 1 fibrosis and contracture is called congenital torticollis (wry neck). - Torticollis: (torti-twisted, callum-neck): The head is bent to one side (to the ,side of spasm) and the chi points towards the opposite side of lesion. It is because of spasm of sternomastoid on the other side.
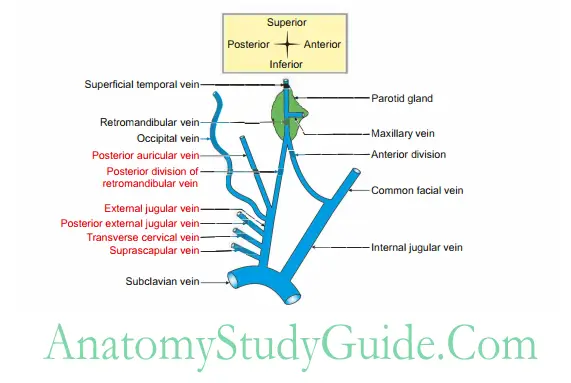
External jugular vein
- External jugular vein Formation: It is formed by union of posterior division of retromandibular and posterior auricular vein.
2. External jugular vein Site: It begins just below the angle of the mandible or within the parotid gland.
3. External jugular vein Peculiarity: It is provided with no valves in its entire course of the vein.
4. External jugular vein Course
- Begins in the lower part of parotid gland.
- Descends almost vertically between platysma and the deep fascia.
- Pierces the fascial roof of the supraclavicular triangle of the neck at the posterior border of sternocleidomastoid.
- Runs in the subcutaneous tissue superficial to sternocleidomastoid.
- It pierces the anteroinferior angle of the posterior triangle and opens into subclavian vein.
5. External jugular vein Tributaries
Transverse cervical, Supraclavicular, Anterior jugular vein, and Posterior external jugular vein.
6. External jugular vein Termination: It drains into subclavian vein behind clavicle.
7. External jugular vein Applied anatomy
- The level of the blood column in the external jugular vein is an indication of the right atrial pressure.
- Puncture of external jugular vein is fatal because of following reasons:
It pierces deep fascia above the clavicle to drain into subclavian vein.
Its lumen is held open by the deep fascia which is attached to its margin.
Leads to sucking of air into the lumen due to negative intrathoracic pressure.
Thereby, it produces an air embolism which is a fatal condition.
Question 4: Describe accessory nerve under the following headings:
1. Origin, course and distribution,
2. Branches, and
3. Applied anatomy.
1. Accessory Nerve Origin, course and distribution
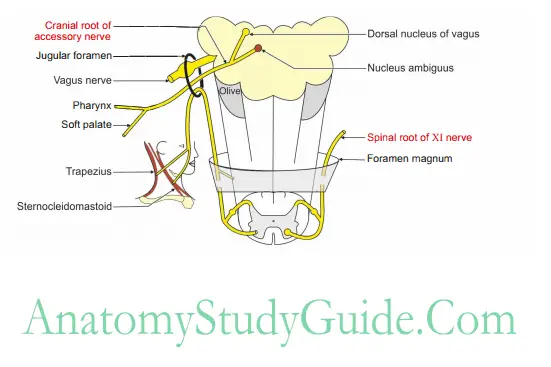
Cranial root
- It emerges by 4 to 5 rootlets, attached to posterolateral sulcus of the medulla.
- It runs with 9th and 10th cranial nerves and the spinal root of accessory root.
They reach the jugular foramen. - In the jugular foramen, the cranial root unites with the spinal root and again separates. r
- The cranial root, fuses with the vagus nerve and supplies the muscles of “pharynx and larynx.
Accessory Nerve Origin Spinal root
- It arises as small rootlets between the ventral and dorsal rami of spinal nerves,from upper 5 segments of spinal cord.
- In the vertebral canal, the filaments unite to form a single trunk and enter the cranium through foramen magnum.
- It runs along with cranial root of accessory and joins in the jugular foramen.
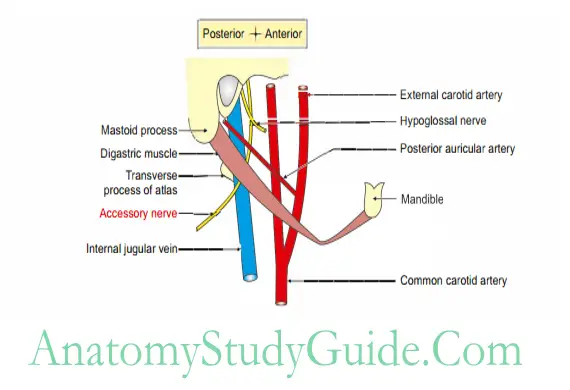
They get separated and emerged independently. - It descends vertically, between the internal jugular vein and internal carotid artery.
- It reaches a point midway between the angle of the mandible and the mastoid process.
- It runs downwards and backwards superficial to internal jugular vein and deep to sternomastoid.
- It pierces the anterior border of stemomastoid at the junction of upper 1 /4th with the lower 3 /4th and emerges through the posterior border of stemomastoid a little above its middle.
- It enters the posterior triangle and lies over the levator scapulae muscle.
It leaves the posterior triangle by passing deep to the anterior border of trapezius and ends by supplying it.
2. Accessory Nerve Origin Branches
3. Accessory Nerve Origin Cranial root supplies muscles of
Palate (except tensor palati which is supplied by mandibular nerve),
Pharynx (except stylopharyngeus which is supplied by glossopharyngeal nerve), and Larynx.
Accessory Nerve Origin Spinal root supplies
Stemocleidomastoid, and Trapezius.
Accessory Nerve Origin Applied anatomy
The accessory nerve is tested clinically
- By asking the patient to shrug his shoulders (trapezius) against resistance and comparing the power on the two sides, and
- By asking the patient to tum the face to the opposite side (stemomastoid)against resistance and again comparing the power on the two sides.
The effects of damage of the spinal part of accessory nerve is as follows:
- The face is turned towards the side of injury.NEEr
- There is an inability to shrug the shoulder towards the side of injury. It is due to paralysis of trapezius muscle.
The pus accumulated near the posterior border of stemocleidomastoid is drained by taking incision across the stemomastoid.
A note of caution, the incision is not taken along the posterior border of stemocleidomastoid to avoid injury of the spinal part of accessory nerve.
Spinal root of accessory nerve is crossed by a lesser occipital nerve at the middle of posterior border of stemocleidomastoid.
Leave a Reply