Temporal and Infratemporal Regions Questions and Answers
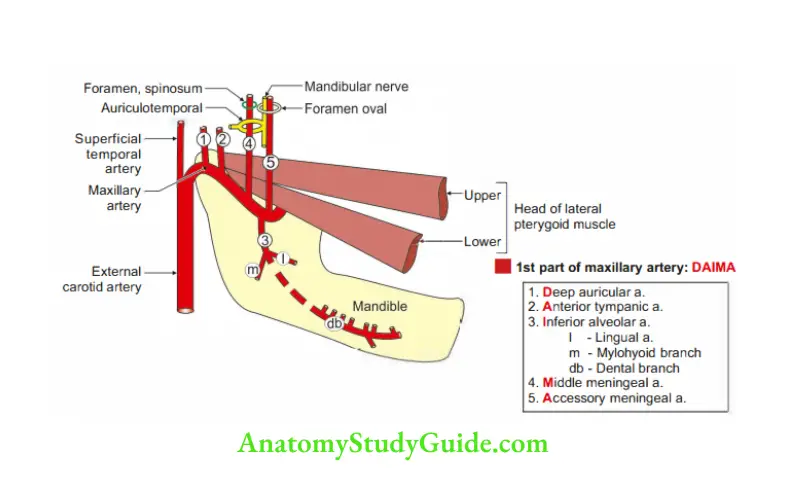
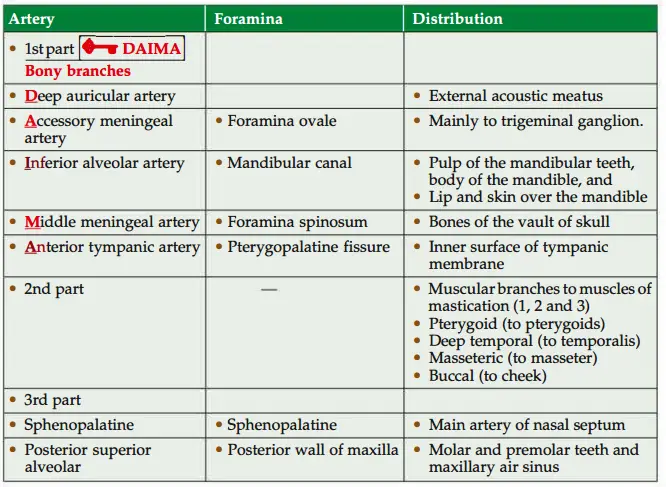
Question 1: Give the branches of 1st part of the maxillary artery.
Table of Contents
Answer: DAIMA
1. Deep auricular,
2. Anterior tympanic,
3. Inferior alveolar,
4. Middle meningeal, and
5. Accessory meningeal.
Read And Learn More: Head Anatomy Notes And Important Questions With Answers
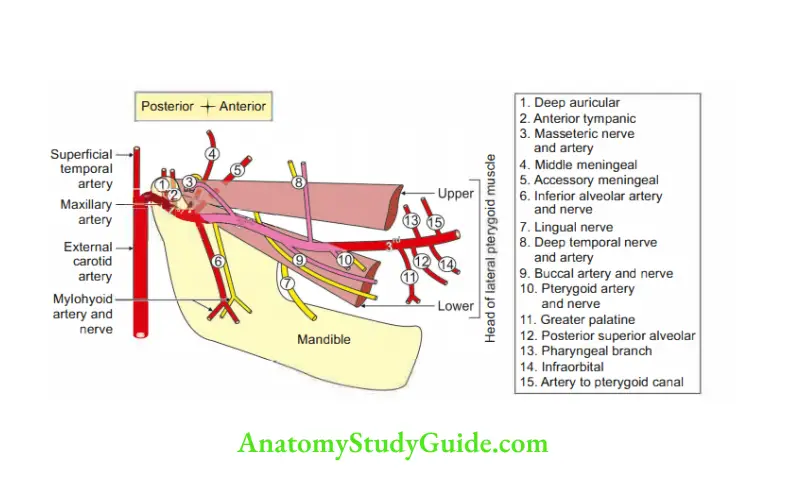
Maxillary artery
Maxillary artery Introduction: It is one of the two terminal branches of the external carotid artery given at the neck of the mandible. It is the artery of the upper and lower jaws, the muscles of mastication, the palate, and the nose.
1. Maxillary artery Course: It is divided into three parts by the lower head of the lateral pterygoid muscle.
It enters the infratemporal fossa.
It lies between the neck of the mandible and the sphenomandibular ligament.
Here the auriculotemporal nerve is above the artery and the maxillary vein lies below the artery.
It enters the pterygopalatine fossa through the pterygomaxillary fissure.
It is divided conveniently into three parts by lateral pterygoid muscle
- 1st part lies proximal to the lower head of the lateral pterygoid.
- 2nd part lies in relation to the lateral pterygoid.
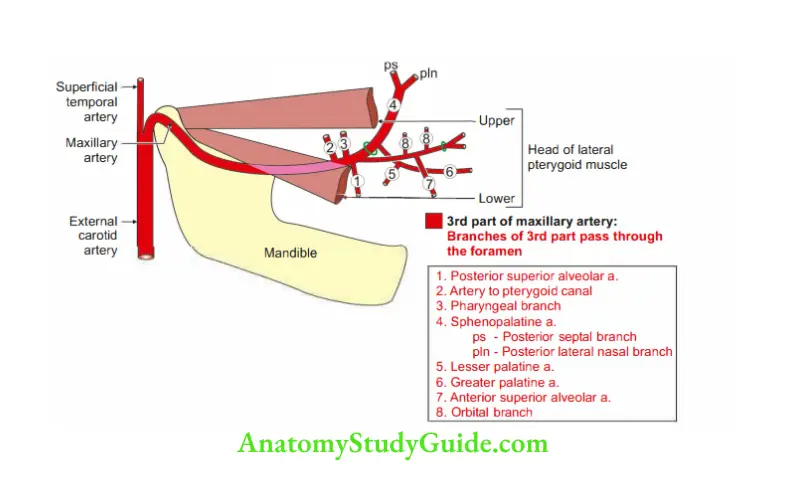
It lies either superficial or deep to the lower head of the lateral pterygoid. - 3rd part lies in the pterygopalatine fossa distal to the upper head of the lateral pterygoid.
2. Maxillary artery Branches: Branches of 1 stand 2nd parts accompany the branches of the maxillary nerve.
3. Maxillary artery Applied anatomy
- Middle meningeal artery is the largest meningeal branch. Clinically, it is the most a important branch of maxillary artery.
- It may be torn in fracture of the skull producing extradural haematoma that –
overlies the motor area of the cerebral cortex.
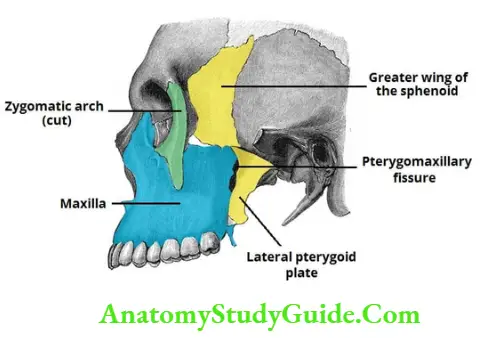
Question 2: Describe Infratemporal Fossa under the following heads:
1. Infratemporal Fossa Boundaries,
2. Infratemporal Fossa Contents, and
3. Infratemporal Fossa Applied anatomy
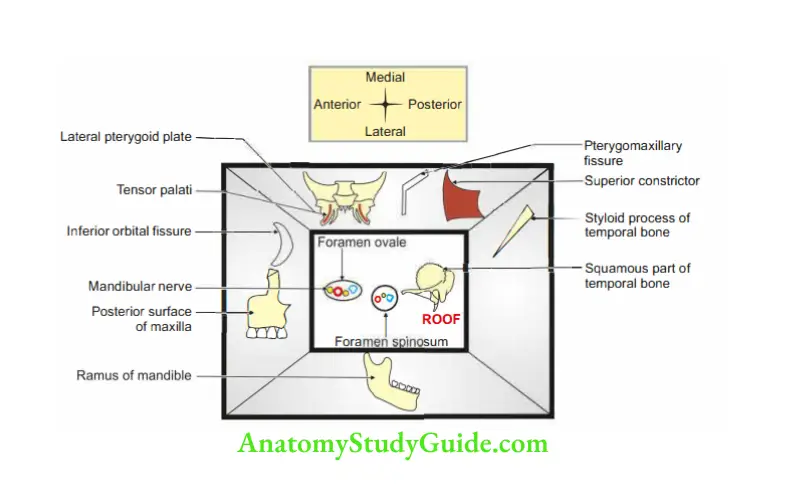
Answer: 1. Infratemporal Fossa Boundaries
Infratemporal Fossa Location: It is the space located deep to the ramus of the mandible.
Infratemporal Fossa Communication
- Temporal fossa.
- Orbit.
- Middle cranial fossa
Infratemporal Fossa Openings
- Foramen ovale,
- Foramen spinosum,
- Pterygomaxillary fissure, and
- Inferior orbital fissure.
Note: The foramen rotundum cannt be seen in the roof of infratemporal fossa.
Infratemporal Fossa Superiorly or roof: It is formed by
- The inferior surface of the greater wing of the sphenoid bone.
- Mandibular surface and inferior surface of the petrous part of the temporal bone.
Infratemporal Fossa Anteriorly
- Posterior surface of maxilla.
- Inferior orbital fissure.
Infratemporal Fossa Medially
- The lateral surface of the lateral pterygoid plate.
- Tensor palatini.
- Superior constrictor.
- Pterygomaxillary fissure.
Infratemporal Fossa Posteriorly
- The anterior surface of the styloid process of the temporal bone.
- Carotid sheath.
Infratemporal Fossa Laterally
- Medial surface of the ramus of the mandible.
- Coronoid process.
2. Infratemporal Fossa Contents
A deep part of the parotid gland
Infratemporal Fossa Muscles
- Insertion of temporal is into the coronoid process,
- Medial pterygoid, and
- Lateral pterygoid.
Infratemporal Fossa Arteries: The Maxillary artery and its branches from the 1st and 2nd parts are the contents of the infratemporal fossa.
Branches of 1st part
- Deep auricular,
- Anterior tympanic,
- Inferior alveolar,
- Middle meningeal, and
- Accessory meningeal.
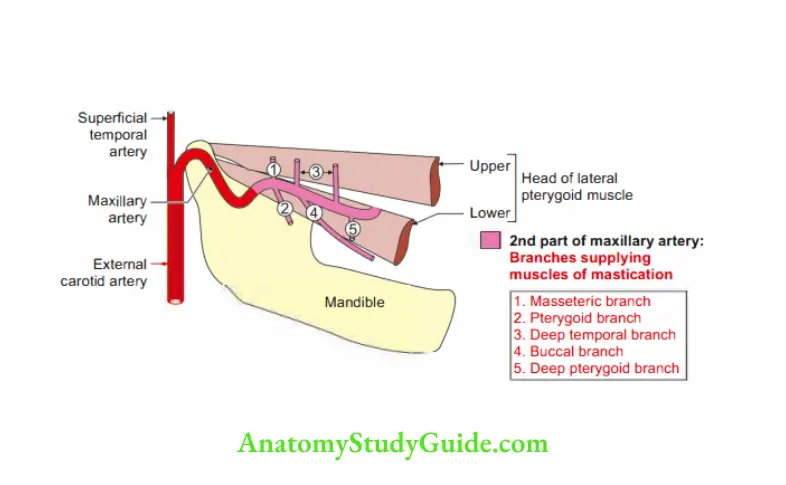
Branches of 2nd part (to muscles of mastication).
- Masseteric branch,
- Temporal branch,
- Pterygoid branch, and
- Buccal branch.
Pterygoid Venous Plexus
Nerves
Branches of mandibular division of trigeminal nerve.
Branches from the main trunk.
- Branch to medial pterygoid.
- Meningeal branch.
Branches from the anterior trunk (mainly motor)
- Masseteric branch.
- Branch to lateral pterygoid.
- Deep temporal branch.
- Buccal branch.
Sensory branches are not the contents of the infratemporal fossa.
Chorda tympani nerve
Posterior superior alveolar branches of maxillary nerve.
Ganglion: Otic ganglion.
Applied anatomy
- Lefort and zygomatic fracture: It is a bilateral horizontal fracture of the maxilla.
It invariably involves infratemporal fossa.
It damages the nerves, blood vessels, and muscles in the region.
The clinical manifestations are Injuries to the 2nd and 3rd divisions of the trigeminal nerve and chorda tympani resulting in altered sensations in the oral cavity and face.
Injuries involving otic ganglion interfere with salivation.
Damage to the motor nerve results in loss of chewing and swallowing movements. - Fractures of the zygomatic bone involve the infratemporal fossa and the maxillary
air sinus.
The infection of this region has grave consequences.
It spreads in the middle cranial fossa through the various foramina present at the roof of the fossa. - Infection from
The impacted 3rd molar tooth also spreads to the infratemporal fossa.
The main symptom of the infection is painful reflex muscle spasm.
The infratemporal fossa may spread to orbit through inferior orbital fissures.
It may result in cavernous sinus thrombosis. - Infection also can spread to the nose, palate, and pharynx through the pterygopalatine fissure.
Question 3: Describe Temporomandibular Joint under the following heads:
1. Temporomandibular Joint Classification,
2. Temporomandibular Joint Ligaments,
3. Temporomandibular Joint Movements and muscles bringing movements,
4. Temporomandibular Joint Sets of movements
5. Temporomandibular Joint Axis of movement
6. Temporomandibular Joint Range of mandibular movements
7. Temporomandibular Joint Nerve supply, and
8. Temporomandibular Joint Applied anatomy
Answer: 1. Temporomandibular Joint Classification: It is also called ginglymoarthrodial joint. It provides
- Hinge movement, and G
- living movement
Structurally: Compound, complex, condylar, multiaxial, saddle-shaped,a typical synovial joint.
- Compound: Two bones namely the mandible and temporal bones and the articular disc take part in the formation of the TM joint.
The inferior surface of the mandibular fossa of the squamous part of the temporal bone,
The superior surface of the head of the mandible, and
Fibrocartilage articular disc. - Complex: The joint cavity is separated by an articular disc into upper meniscotemporal and lower menisci-mandibular compartments.
- Condylar: Left and right condyles of the head of the mandible form a bicondylar articulation.
- Multiaxial: The movements are vertical, transverse, and anteroposterior axis.
- Saddle-shaped: The articular surface of the head of the mandible is convex.
the concave surface which articulates with the concavo-convex surface of the mandibular fossa of the temporal bone. - Atypical synovial: The articular surfaces of the head of the mandible and mandibular fossa of the temporal bone are not covered by hyaline cartilage but are covered by fibrocartilage.
Here collagen fibres predominate and cartilage cells are few.
Because the concerned bones ossify in the membrane.
Functionally: Diarthrosis.
2. Temporomandibular Joint Ligaments: The ligaments can be divided into
Main ligaments
Fibrous capsule
Attachments
- Above
Anteriorly: Anterior to articular tubercle.
Posteriorly: Posterior to the squamotympanic fissure.
Medially and laterally: To the margins of the mandibular fossa. - Below: The capsule is attached at a higher level near the articular margin of the head of the mandible. Posteriorly, it is attached to the neck lower down.
Nature of the capsule
- Loose and lax above the disc
- Lense and thick below the disc
Peculiarities
- It is spacious, lax, and strong.
- It gives attachment to the lateral pterygoid muscle.
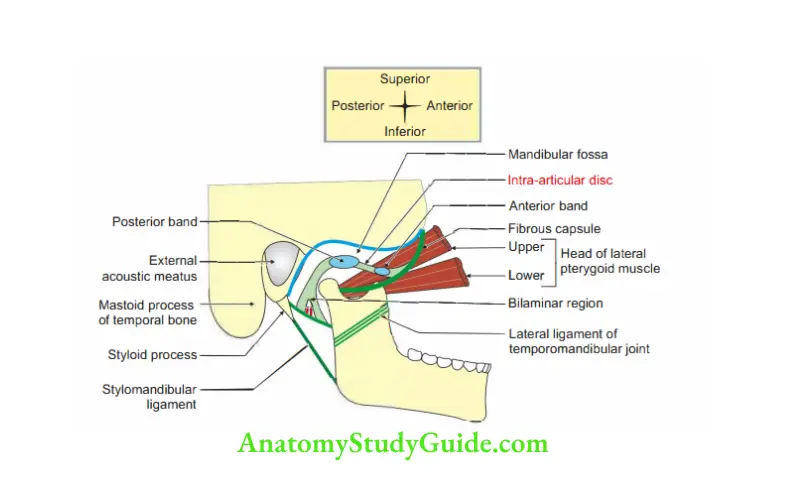
Articular disc: It is oval in shape and fibrocartilage in nature (Fig. 10.6).
- Morphologically, it represents lateral pterygoid muscle.
- It is attached
Anteriorly, medially, and laterally near the head of the mandible.
Peripherally to the inner side of the fibrous capsule. - Parts
Anterior extension.
Posterior bilaminar extension. - Variation in thickness: It is thick peripherally and thin in the center.
- Peculiarity: Gives attachment to lateral pterygoid muscle.
- Functionally, it divides the joint cavity into upper and lower compartments.
The movement in the upper compartment is gliding.
The movement in the lower compartment is rotatory and gliding.
Lateral ligament of TM joint
- It is a stout band of fibrous tissue.
- It covers a lateral aspect of the capsule and strengthens it.
- It extends from the tubercle of the root of the zygoma to the neck of the mandible.
- It tightens in retraction and protraction and relaxes in the rest position.
Synovial membrane
- It lines the fibrous capsule above and below the disc but does not cover the disc.
- It lines the non-articular surface of articulating bones.
- In newborns, even the articular surfaces are covered by synovial membrane.
2. Temporomandibular Joint Accessory ligaments
Sphenomandibular ligament
- Introduction: It is an accessory ligament of the temporomandibular joint, which lies on a deep plane away from the fibrous capsule.
Attachments
- Above to the spine of the sphenoid bone.
- Below to the lingula of the mandible.
Stylomandibular ligament
- It is a thickening of deep cervical fascia between the angle of the mandible and the styloid process.
- It stretches
From the
Apex, and
Adjacent anterior aspect of the styloid process - To the Angle of the mandible, and Posterior border.
It is considered only an accessory to the joint. The function is not exactly known.
3. Temporomandibular Joint Movements and muscles bringing movements: There are three sets of mandibular movements at the TM joint.
1. Movements and muscles bringing movements.
Depression and elevation
- Depression is produced mainly by the lateral pterygoid. The digastric, geniohyoid, and mylohyoid muscles help when the mouth is opened wide or against resistance.
- Elevation is produced by the masseter, the temporalis, and the medial pterygoid muscles of both sides.
Side-to-side movement (gliding movement): Lateral or side-to-side movements are produced by the medial and lateral pterygoids of each side acting alternately.
Protraction and retraction
Protraction is done by the lateral pterygoid (principally its inferior head) and medial pterygoids.
Retraction is produced by the posterior fibers of the temporalis.
It may be resisted by the middle and deep fibers of the masseter, the digastric, and the geniohyoid muscles.
2. Position of articular disc and head of the mandible in movements of TM joint
When the chin is depressed
In the upper compartment: Meniscofemoral compartment
- The articular disc and the head of the mandible move forward.
- The movement is on the upper articular surface.
The movement continues till the head of the mandible lies inferior to the articular tubercle.
In the lower compartment
- At the same time, the head of the mandible rotates on the lower surface C of the disc.
- The latter movement alone is capable of permitting simple chewing movements over a small range.
When small chewing movements are made without separating lips. The head of mandible moves in the mandibular fossa.
When the mouth is opened wide, the head of the mandible swings forward and downwards.
4. Temporomandibular Joint Sets of movements: There are three sets of mandibular movements at the TM joint.
These are
1. Depression and elevation
- In a slight opening of the mouth or depression of the mandible, the head of the mandible moves on the undersurface of the disc like a hinge.
- In the wide opening of the mouth, the hinge-like movements are followed by the gliding of the disc and the head of the mandible, as in protraction.
At the end of this movement, the head comes to lie under the articular tubercle.
These movements are reversed in closing the mouth or elevation of the mandible. - Active depression is produced mainly by the lateral pterygoid. The digastric, geniohyoid, and mylohyoid muscles help when the mouth is opened wide or against resistance.
- Passive depression is produced by gravity.
- Elevation is produced by the masseter, the temporalis, and the medial pterygoid muscles on both sides.
2. Side-to-side movement (gliding movement): Lateral or side-to-side movements
are produced by the medial and lateral pterygoid of each side acting alternately.
3. Protraction and retraction
- In protraction, the articular disc glides forward over the upper articular surface, the head of the mandible moving with it.
The protrusion is done by the lateral (principally its inferior head) and medial pterygoids. - In retraction, the articular disc glides backward over the upper articular surface, the head of the mandible moving with it.
It is produced by the posterior fibers of the temporalis.
It may be resisted by the middle and deep fibers of the masseter, the digastric, and geniohyoid muscles.
5. Temporomandibular Joint Axis of movement
- In small movements, the axis is through the head of the mandible.
- In a wider range of movements, the axis passes approximately through the mandibular foramen.
6. Temporomandibular Joint Range of mandibular movements
1. Opening of the mouth
- The maximal opening of the jaw is about 50 mm.
- The functional range of the opening is about 40 mm.
- Opening of the jaw by rotation is about 25 mm.
- The last range of 15 mm is by anterior translateral (from side to side) gliding.
2. In protrusion of the mouth: The maximal range of protrusion and lateral displacement is about 10 mm each.
7. Temporomandibular Joint Nerve supply
- The auriculotemporal nerve is a branch of the posterior division of the mandibular nerve.
- The masseteric nerve is a branch of the anterior division of the mandibular nerve.
8. Temporomandibular Joint Applied anatomy
Lockjaw
- Disc displacement: The unique feature of the articular disc is it is made up of elastic cartilage which is flexible.
It serves as a cushion between two bony surfaces.
The disc lacks arteries and nerves. Hence, it is pain-insensitive.
Anteriorly, it continues as lateral pterygoid muscle.
Posteriorly, it continues as methodical tissue.
The retrodiscal tissue has a rich nerve supply and blood supply. - Disc displacement is the most common disorder. In most cases, the disc is dislocated anteriorly.
As the disc moves forward, methodical tissue is caught between two bones.
This can be very painful as it has a rich nerve supply. - The forward dislocated disc forms an obstacle for condylar movement. In order to open the jaw fully, the condyle has to jump over the backend with sense.
This produces a clicking sound. This condition is called disc displacement with reduction. - In later stages of disc dislocation, the condyles stay behind all the time unable to set back on the disc, the clicking sound disappears but mouth opening is limited.
This is usually the most symptomatic stage. - The jaw is set to be locked as it is unable to open its wide mouth.
At this stage, the condition is called disc displacement without reduction.
Fortunately, in the majority of cases, the condition resolves by itself.
This is called the natural adaptation of retrodiscal tissue.
This becomes scar tissue and functionally replaces the disc.
In fact, it becomes too similar to disc and is called pseudodisc. - Forward dislocation is the commonest form of displacement.
With the mouth open, the condyles are in the articular eminence, and sudden violence, even muscular spasms (a convulsive yawn), may displace one or both temporomandibular joints. - Anterior dislocation readily occurs in the edentulous, i.e. person without teeth.
It is easily reduced; the joint is less stable because the increased elevation of the edentulous mandible permanently elongates the lateral ligament. - The reduction of the TMjoint is easily achieved by pressing down on the molar teeth with thumbs placed in the mouth, and at the same time pushing the chin upward and backward.
The downward pressure on the molar teeth overcomes the tension of the temporalis and masseter muscles which are in spasm.
Andu the upward and backward pressure on the chin helps the head of the mandible to put into its original position. - The lateral ligament of the TM joint is very strong.
It helps in the following ways:
It prevents backward falling of the head of the mandible.
It prevents the fracturing of the tympanic plate.
This is very much true when a severe blow falls on the chin. - The articular disc of the temporomandibular joint may become partially detached
from the capsule. It results in noisy movements.
It produces an audible click during movements at the joint.
Describe the factors responsible for the stability of Temporomandibular Joint
The following factors maintain the stability of the temporomandibular joint.
1. Temporomandibular Joint Bones
- Forward displacement is prevented by articular tubercles, and
- Backward displacement by post-glenoid tubercle.
2. Temporomandibular Joint Ligament: The lateral ligament of TMJ strengthens the capsule posterolaterally. It prevents the backward dislocation of the mandible.
3. Temporomandibular Joint Muscles
- The protrusion is limited by the tension in the temporalis.
- Retraction is limited by the tension in lateral pterygoid muscles.
4. Temporomandibular Joint Position of the mandible: In occlusion, the following factors play an important role in the stabilization of the joint.
- Teeth themselves stabilize the mandible on the maxilla. No strain is thrown on the joint when an upward blow is received by the mandible.
- Forward movement of the condyle is discouraged by the
Prominence of articular eminence, and
Contraction of posterior fibers of temporalis. - Backward movement is prevented by the
Fibers of lateral ligament, and
Contraction of the lateral pterygoid.
Articular Disc of TM Joint (meniscus)
Articular Disc of TM Joint Introduction: It is the fibrocartilaginous structure separating the cavity of the TM joint.
1. Morphology
- Shape—oval
- Attachments
Anteriorly to the neck of the mandible.
Peripherally to the fibrous capsule.
Medially and laterally to the neck of the mandible. - Surfaces: The superior surface of the disc is anteroposteriorly concavo-convex.
The inferior surface of the disc is concave. - Extensions
Thick anterior band
Thick posterior band
Thin in the middle - The posterior band divides into two laminae with a venous plexus in between
Upper lamina: It is attached above the mandibular fossa and is fibroblastic in nature.
Lower lamina: It is attached to the mandible and is non-elastic. - Variation in thickness
Thick at the periphery, and
Thin in the center.
2. Articular Disc of TM Joint Peculiarities: It gives attachment to lateral pterygoid muscle.
3. Articular Disc of TM Joint Functions: It divides the joint cavity into upper and lower compartments.
4. Articular Disc of TM Joint Movements
- Gliding movement in the upper compartment.
- Gliding and rotation movement in the lower compartment.
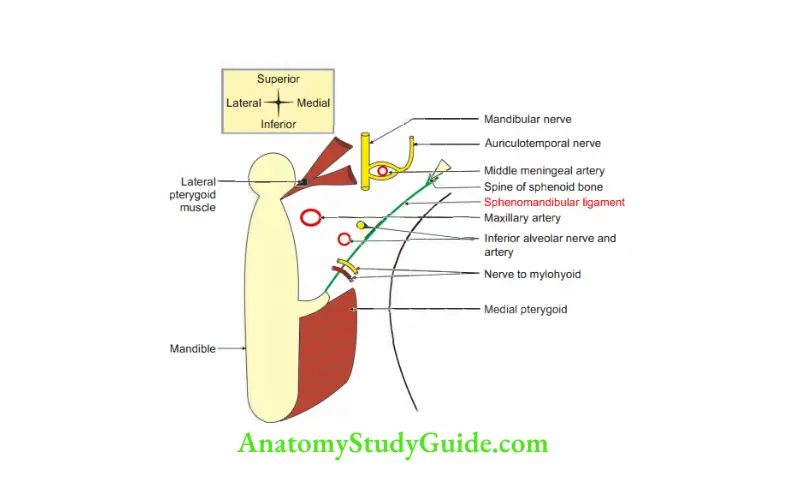
Sphenomandibular Ligament
Sphenomandibular Ligament Introduction: It is an accessory ligament of the temporomandibular joint. It lies on a deep
plane away from the fibrous capsule.
1. Sphenomandibular Ligament Attachment: From spine of sphenoid bone to the lingula of mandible.
2. Sphenomandibular Ligament Relations
Laterally: MAIL
- Maxillary artery.
- Auriculotemporal nerve.
- Inferior alveolar nerve.
- Lateral pterygoid muscle.
Sphenomandibular Ligament Medially:
- Medial pterygoid muscle.
- Corda tympani nerve.
- Wall of the 12arynx.
3. Sphenomandibular Ligament Development: It develops from the mesenchyme of the 1st pharyngeal arch. It is a remnant of the dorsal part of Meckel’s cartilage.
4. Sphenomandibular Ligament Applied anatomy
Sphenomandibular ligament is ruptured by
- Fracture of the neck of the mandible, or
- Dislocation of temporomandibular joint.
It leads to loss of taste sensations due to injury to chorda tympani nerve.
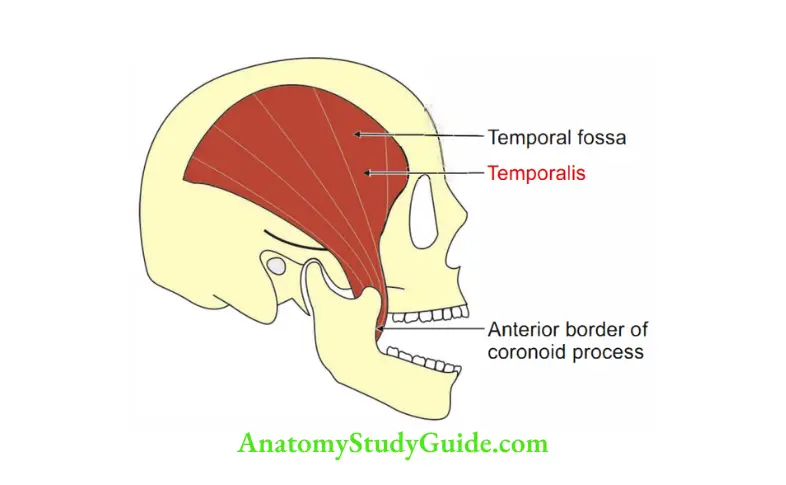
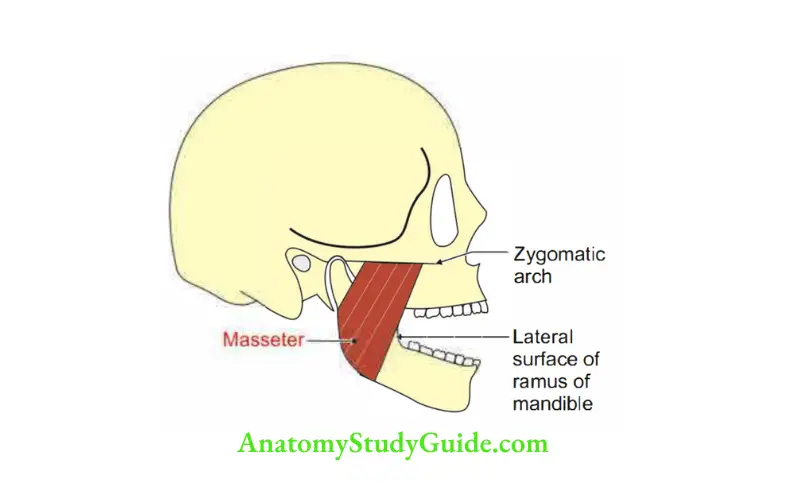
Question 4: Describe muscles of mastication under the following headings:
1. Muscles Of Mastication Proximal attachments,
2. Muscles Of Mastication Distal attachments,
3. Muscles Of Mastication Action, and
4. Muscles Of Mastication Nerve supply
Answer:
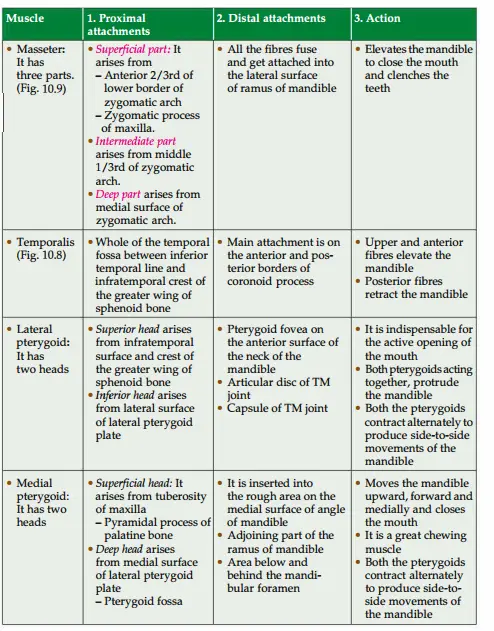
4. Muscles Of Mastication Nerve supply: All the muscles of mastication are supplied by branches from the anterior trunk of the mandibular nerve except the medial pterygoid which is supplied by the branch from the main trunk of the mandibular nerve.
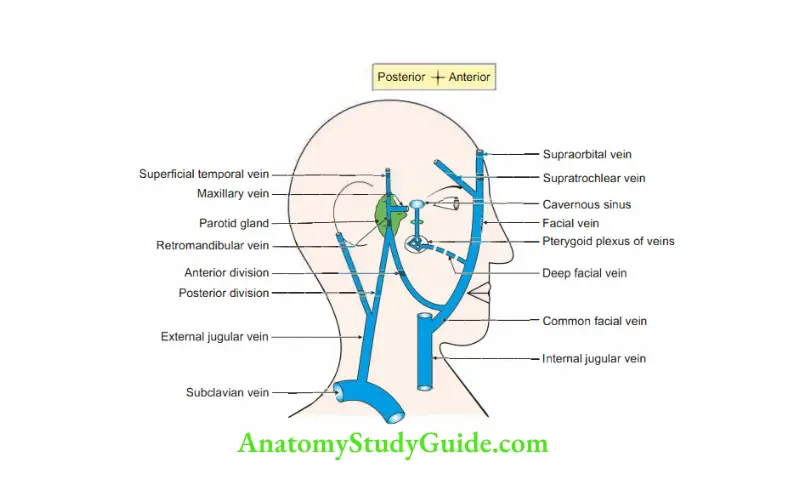
Pterygoid venous plexus
Introduction: It is a plexus of veins present
- Superficial to lateral pterygoid muscle.
- Deep to lateral pterygoid muscle.
- In the lateral pterygoid muscle.
- Partly between temporalis and lateral pterygoid.
- Partly between two pterygoid muscles.
1. Tributaries of the plexus correspond to the branches of the maxillary arteries. They are
1. From muscles of mastication.
- Deep temporal
- Masseter
- Pterygoid
- Buccal
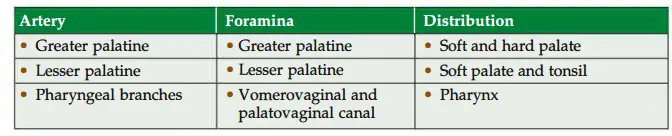
2. Veins of palate
- Palatine
- Sphenopalatine
3. Veins of cranium: Middle meningeal vein
2. Termination: It drains into the maxillary vein which is formed at the lower border of
lateral pterygoid muscle deep to the neck of the mandible.
They run back and join with the superficial temporal vein to form the retromandibular vein.
3. Communications: It has important communication with
- Inferior ophthalmic vein through veins of the inferior orbital fissure.
- Cavernous sinus via emissary veins. These emissary veins pass through the foramen ovale and foramen of Vesalius (emissary sphenoidal foramen)
- Facial vein via deep facial veins.
4. Role of pterygoid plexus: (Contraction of lateral pterygoid muscle facilitates venous return to the heart. Hence, lateral pterygoid is called a peripheral heart.) The veins of the plexus have valves that suck the blood from incompressible parts (face, bones, and orbit) and pump it back into maxillary veins.
5. Applied anatomy: The infection from the face can spread to the cavernous sinus via the plexus.
Lateral Pterygoid Muscle
Lateral Pterygoid Muscle Introduction: It is the muscle of mastication.
1. Lateral Pterygoid Muscle Features:
1. It acts as a peripheral heart. It has a plexus of veins present
- Superficial to lateral pterygoid
- In the lateral pterygoid
- Deep to lateral pterygoid
These veins have valves that help in venous return.
2. The emissary veins passing through the foramen ovale and foramen lacerum connect the pterygoid venous plexus to the cavernous venous sinus.
3. It is a key muscle of the temporal and infratemporal regions.
2. Lateral Pterygoid Muscle Origin: It arises from two heads
1. Upper head arises from
- Roof of infratemporal fossa.
- Infratemporal crests of the greater wing of the sphenoid bone.
2. The lower head is larger and arises from the lateral surface of the lateral pterygoid plate.
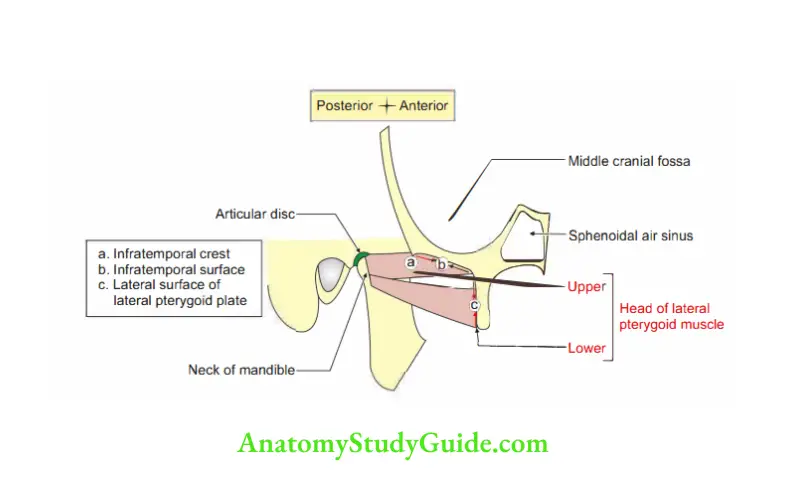
3. Lateral Pterygoid Muscle Insertion: The two heads lying edge-to-edge fuse and form a short tendon which is inserted into
- Pterygoid fovea of the neck of the mandible.
- Capsule of temporomandibular joint.
- Articular disc of temporomandibular joint.
4. Lateral Pterygoid Muscle Relations
1. Superficial (visualize mandible and structures attached and related to it.)
- Masseter,
- Ramus of the mandible,
- Tendon of temporalis, and
- Maxillary artery.
2. Deep
- Mandibular nerve
- Middle meningeal artery
- Sphenomandibular ligament
- Deep head of medial pterygoid
3. Structures emerging at the upper border
- Deep temporal nerve
- Masseteric nerve
4. Structures emerging at the lower border
- Lingual nerve,
- Inferior alveolar nerve, and
- Middle meningeal artery.
5. Between two heads of lateral pterygoid
- 3rd part of the maxillary artery.
- Buccal branch of mandibular nerve.
5. Lateral Pterygoid Muscle Nerve supply: It is supplied by a branch anterior division of the mandibular nerve.
6. Action
- It is an indispensable muscle for the active opening of the mouth.NEEr
- Protraction: It draws condyle and disc forward.
- Helps in side-to-side movements.
7. Development: It is developed from the mesoderm of 1st pharyngeal arch.
Question 5: Describe the mandibular nerve under the following headings:
1. Course and relations,
2. Development,
3. Branches, and
4. Applied anatomy
Introduction: It is 3rd division of the trigeminal nerve. It is a mixed nerve supplying the muscles developed from 1st pharyngeal arch. It is also sensory to the skin and mucous membrane of the mandible.
1. Course and relations
- It arises from trigeminal ganglion.
- It lies in the dura mater of the middle cranial fossa lateral to the cavernous sinus.
- The sensory and motor roots pass through the foramen ovale.
- Both roots meet in the infratemporal fossa and a mixed nerve is formed.
- It begins as a trunk and divides into anterior and posterior divisions.
- The nerve lies deep to the upper head of the lateral pterygoid and tensor palatini.
- The optic ganglion lies between the mandibular nerve and the lateral pterygoid.
2. Development: It is the nerve of the 1st pharyngeal arch.
3. Branches
From main trunk
Sensory: Meningeal (nervus spinosus): It gives a cartilaginous branch to the eustachian tube and enters the middle cranial fossa through foramen spinosum.
It is accompanied by middle meningeal vessels. In the skull, it supplies
- Dura mater of middle cranial fossa,
- Mastoid antrum, and
- Mastoid air cells.
Motor: It gives the motor branch to the medial pterygoid and gives the motor root to the otic ganglion.
The root passes near or through the ganglion without synapse.
Its fibres supply
- Tensor palatini, and
- Tensor tympani
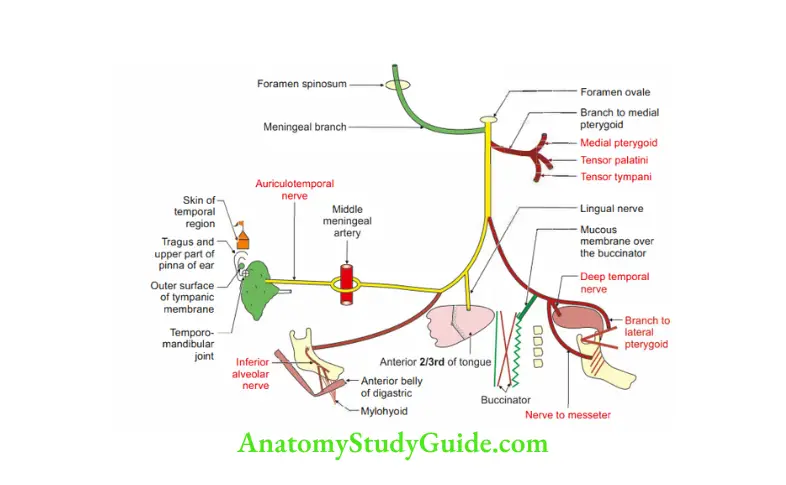
Branches from divisions: After a distance of 4 to 5 mm, the nerve divides into a cat of nine tails. Six branches from the anterior division and three branches from posterior division.
Anterior division (mainly motor): All the branches of the anterior division are motor except the buccal branch which is sensory.
Masseteric nerve: It runs on the upper border of the lateral pterygoid and supplies
- Masseter muscle, and
- Temporomandibular joint.
Buccal branch: It is purely sensory. It passes between two heads of lateral
pterygoid. It runs in a fascial tunnel on the deep surface of the temporal muscle
and supplies
- The external skin of the cheek,
- Internal mucous membrane,
- Proprioceptive sensations of buccinator muscle, and
- Gums of lower jaw opposite lower molar and premolar.
Along with parotid duct, buccal branch of mandibular nerve pierces buccinator.
Pterygoid branches: They are two in number and supply
Upper head of lateral pterygoid, and
Lower head of lateral pterygoid.
Temporal branches: They are anterior and posterior and run on the upper border of the lateral pterygoid.
They supply the temporalis muscle.
Posterior division (mainly sensory): All the branches of the posterior division are sensory except the nerve to mylohyoid which is motor.
As a rule, the anterior division is motor, and the posterior division is sensory.
Every rule has an exception.
On a lighter note: Exception proves the rule. If there are no exceptions, there are no rules.
All the branches of the anterior division are motor except the buccal branch which is sensory.
All the branches of the posterior division are sensory except the nerve to the mylohyoid which is motor.
Auriculotemporal: It arises from two roots.
It hugs the middle meningeal artery since it is going to the temple to have a darshan.
It passes backward between the neck and the ligament of the mandible (sphenomandibular ligament).
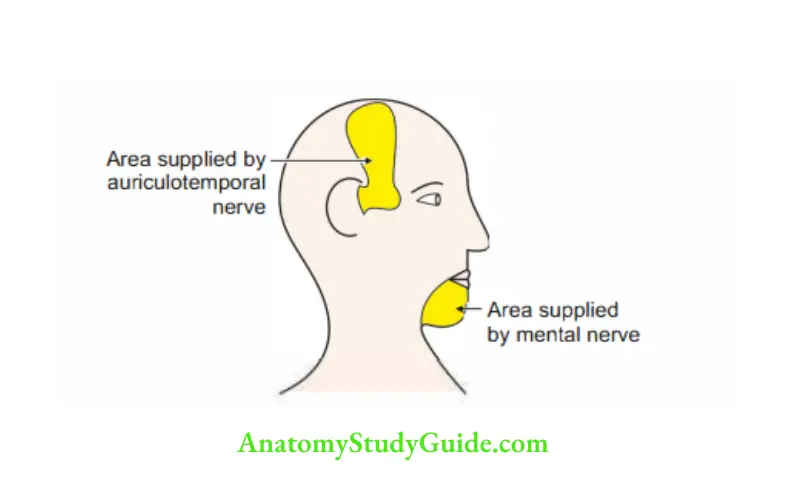
As the name suggests, it supplies structures surrounding the ear and temporal region.
- Skin of temporal region,
- Temporomandibular joint,
- Tragus,
- The upper part of the pinna of ear,
- The outer surface of the tympanic membrane, and
- Parotid gland (postganglionic secretomotor fibres from otic ganglion).
Great auricular nerve is great in the following aspects
1. It is the largest ascending branch of the cervical plexus.
2. It supplies the skin over the parotid gland and parotid fascia.
3. It supplies the area of skin of the ear which is pinched by a person who is great for the pinched person.
Note: Skin over the parotid gland and parotid fascia is supplied by the great auricular nerve.
2. Inferior alveolar nerve
- It is a large branch of the posterior division.
- It emerges below the lower head of the lateral pterygoid.
- It lies anterior to its vessels and between sphenomandibular ligament 1 and the ramus of the mandible.
- It gives a branch called a nerve to the mylohyoid and enters the mandibular canal.
- Nerve to mylohyoid pierces sphenomandibular ligament. It supplies
Mylohyoid muscle, and
Anterior belly of digastric muscle. - Inferior alveolar nerve supplies
Three molars and two premolar teeth. It divides into
Mental nerve, and
Incisive nerve. It supplies pulps and the periodontal membrane of the canine and incisors. - Lingual nerve: It appears below the lateral pterygoid muscle on the side of the pharynx.
It joins with the chorda tympani at an acute angle.
It emerges medial to the mandible at the third molar tooth.
It carries General and special sensations of the anterior two-thirds of the tongue (through chorda tympani)
The mucous membrane of the floor of the mouth.
4. Applied anatomy
- The sensory function of the mandibular nerve is tested with a wisp of cotton on the skin of the mandible.
- Motor function of the mandibular nerve is tested by asking the patient to clench the teeth firmly.
The contraction of the masseter can be felt by palpation when the teeth are clenched. - Injury to trigeminal nerve causes paralysis of muscles of mastication.
The chin is kept in the midline by the balanced tone of the muscles.
In paralysis of the pterygoid muscles of one side, the chin is pushed to the paralyzed side by the muscles of the opposite side. - Pain arising from an area supplied by one branch of the trigeminal nerve may be referred to as another area of skin supplied by another branch of the nerve.
Thus, caries of the teeth of the lower jaw or ulcer of the tongue may cause pain in the ear because both are supplied by branches of the mandibular nerve.
A needle introduced to a depth of 4 cm in the coronal plane above the mandibular notch and in front of the neck of the mandible reaches the mandibular nerve.
Usually, the needle is inserted until it strikes the lateral pterygoid plate.
It is then passed posteriorly along the lateral pterygoid plate to reach the vicinity of the foramen ovale. - Mandibular nerve block: It is given for the extraction of the teeth of the lower jaw.
The needle is inserted in the interval between pterygomandibular raphe and the anterior margin of the ramus of the mandible.
The tip of the needle is near the inferior alveolar nerve, just before it enters the mandibular canal. The anesthetic injected here blocks the nerve. - A lesion at the foramen ovale involves the mandibular nerve and results in paraesthesia along the mandible, the lower (mandibular) teeth, and the side of the face. There is also paralysis of muscles of mastication and loss of the jaw-jerk reflex as this nerve supplies both afferent and efferent fibers for the jaw-jerk reflex.
- Mandibular neuralgia: The pain along the distribution of mandibular division of trigeminal nerve is called mandibular neuralgia. It is often difficult to treat. This is treated by division of the sensory root of the trigeminal nerve.
Inferior alveolar (dental) nerve
Introduction: It is a branch of the mandibular nerve. Its muscular part supplies the mylohyoid and anterior belly of the digastric.
Its sensory part carries sensations of the teeth, pulp, and periodontal membrane of the lower jaw.
1. Origin: It arises from the posterior division of the mandible nerve, below the lower head of the lateral pterygoid.
2. Course and relations: It lies anterior to its vessels between the sphenomandibular ligament and ramus of the mandible and enters the mandibular foramina.
It runs along with vessels in the mandibular canal. It supplies three molars and two premolars.
3. Branches
- Mental nerve,
- Incisive nerve and
- Nerve to mylohyoid: It pierces the sphenomandibular ligament and supplies mylohyoid muscle.
4. Applied anatomy
- An inferior alveolar nerve block is used for the extraction of all teeth, except incisors.
- For inferior alveolar block, the needle is inserted orally through the buccinator
above the 3rd molar tooth and in front of pterygomandibular raphe.
SN-85 Otic ganglion
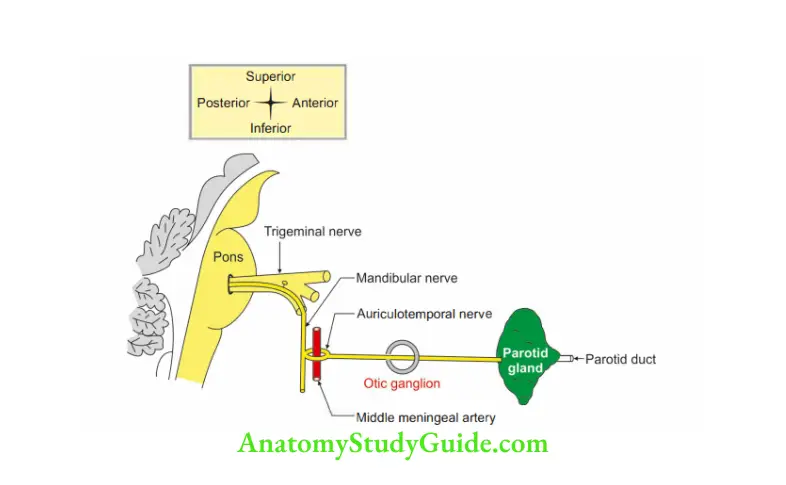
It is a collection of cell bodies of postganglionic parasympathetic nerves. It is situated t outside the central nervous system. The fibers supply the parotid gland. Topographically ”
(the description of the anatomical region), it is related to the mandibular nerve and functionally it is related to the glossopharyngeal nerve.
1. Size: 2-3 mm in size.
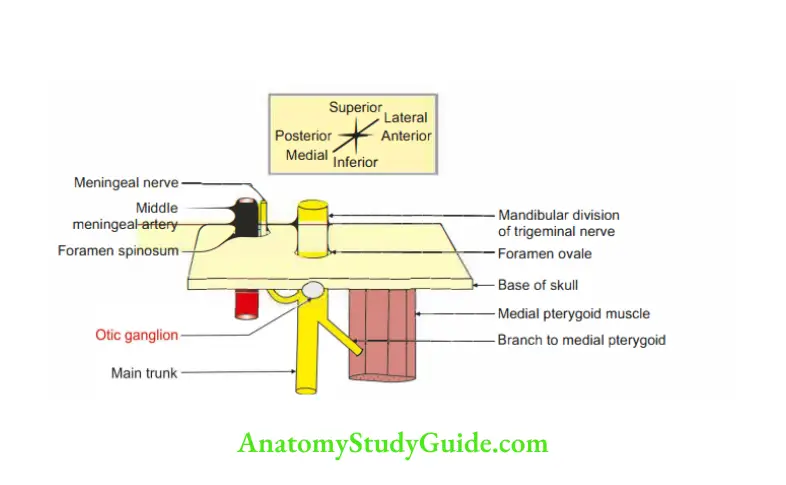
2. Situation: Infratemporal fossa at the base of foramen ovale.
3. Synonym: Arnold ganglion.
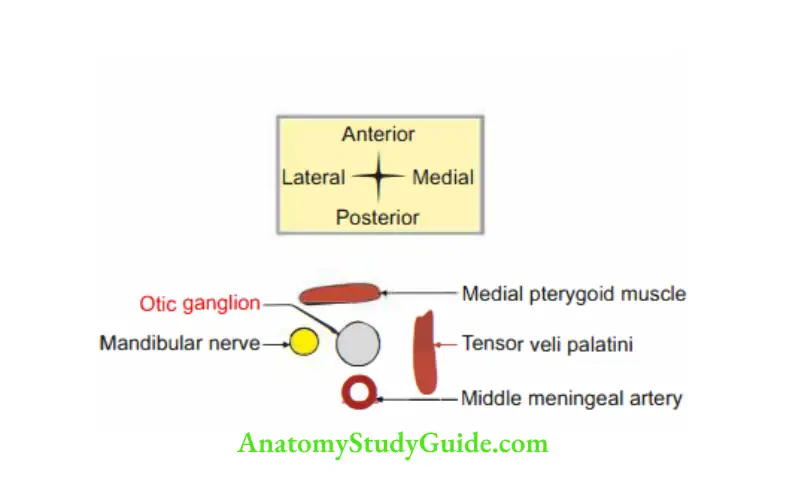
4. Relations of otic ganglion
- Superiorly: Foramen ovale.
- Anteriorly: Medial meningeal muscle
- Posteriorly: Middle meningeal artery.
- Medially: Tensor veli palatini.
- Latera11y: Mandibular nerve.
5. Connections:
1. Parasympathetic or motor root
- Preganglionic: Inferior salivatory nucleus-glossopharyngeal nerve—panic branch of glossopharyngeal nerve.
It forms the tympanic plexus along with caroticotympanic branch of the internal carotid artery. A branch from the plexus, a lesser petrosal branch is given that passes through foramen ovale-otic ganglion-relay. - Postganglionic: Auriculotemporal nerve-parotid gland.
2. Sensory: The auriculotemporal nerve passes through the otic ganglion without a relay.
Sympathetic
- Preganglionic: Spinal nerve-superior cervical sympathetic ganglion.
- Postganglionic: Plexus around external carotid artery-maxillary artery middle meningeal artery.
6. Branches:
- Auriculotemporal nerve to parotid gland.
- Nerve to the medial pterygoid passes through the otic ganglion and supplies the
Tensor palatini, and Tensor tympani. - The otic ganglion is connected to the chorda tympani nerve and the nerve of the pterygoid canal.
This communicating channel possibly forms an alternate route of the taste pathway from the anterior two-thirds of the tongue to the geniculate ganglion of the facial nerve.
7. Applied anatomy: Injury to the auriculotemporal nerve manifests in the loss of salivation.
Leave a Reply