Anatomical Landmarks Edentulous Mandibular Arch Introduction
Fabrication of complete denture for mandible is different than in maxilla due to presence of movable organs on both the sides, i.e. tongue and cheeks. This chapter deals with various anatomical landmarks of edentulous mandible.
Table of Contents
Supporting Areas (Stress Bearing Areas):
- Buccal shelf area (primary stress bearing area)
- Retromolar pad (primary stress bearing area)
- Slopes of residual alveolar ridge (secondary stress bearing area).
Read and Learn More: Preclinical Prosthodontics Notes
Relief Areas:
- Crest of residual alveolar ridge
- Mental foramen
- Genial tubercles
- Torus mandibularis
- Sharp mylohyoid ridge.
Valve Forming Structures (Limiting Areas):
- Labial vestibule
- Buccal frenum
- Buccal vestibule
- Alveololingual sulcus
- Pterygomandibular raphe.
Supporting Areas (Stress Bearing Areas)
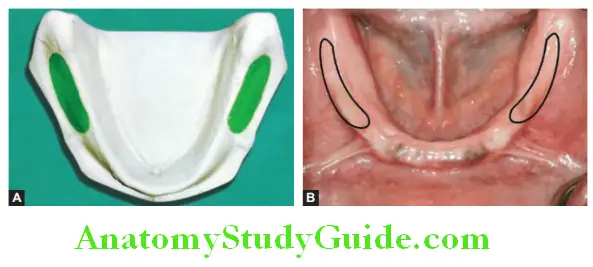
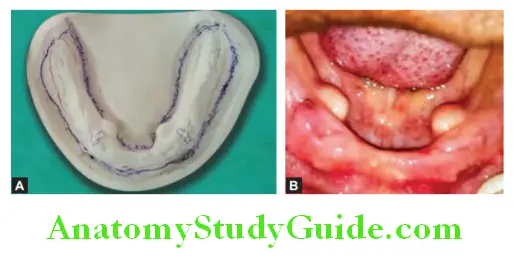
Buccal Shelf Area:
It is at right angle to masticatory load making it appropriate for primary supporting area. It is made up of cortical bone and firmly attached mucosa with muscle fibers running parallel to the buccal shelf region.
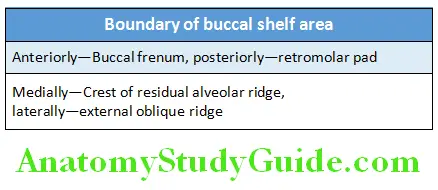
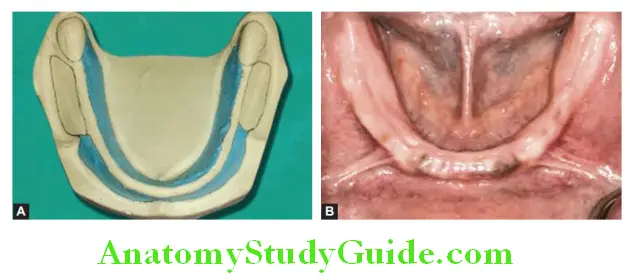
Retromolar Pad:
It is triangular soft pad of tissue at posterior most end of mandibular edentulous ridge. The mandibular denture should cover the retromolar pad. The underlying bone is dense cortical bone and has muscle attachment. The bone is resistance to resorption in this area makes it stress bearing area. The denture should cover it to get good support.
Slopes of Residual Alveolar Ridge:
Slopes of residual alveolar ridge provide more support than crest. Both buccal and lingual slopes of mandibular residual ridge are secondary supporting areas. These slopes are made up of thin plate of cortical bone and are at acute angle to masticatory load.
Relief Areas
Crest of Residual Alveolar Ridge:
This area is relieved because of type of bone present on the crest of mandibular residual alveolar ridge. The bone in this area is cancellous. In spite of submucosa having fibrous connective tissue at the crest, this area cannot bear the masticatory load directly hence considered as relief area. It should be relieved when it is sharp and spiny or knife edge.
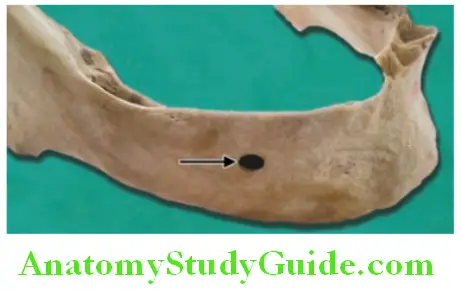
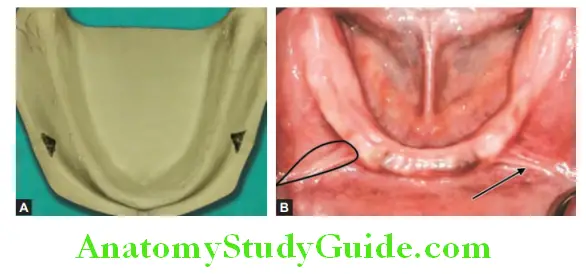
Mental Forame:
It is located between first and second premolars regions (see arrow in figure). Due to excessive ridge resorption it may lies close to crest of residual alveolar ridge. In such cases it should be relieved as pressure over the mental nerve coming out through foramen produces paresthesia in lower lip area see arrow in figure.
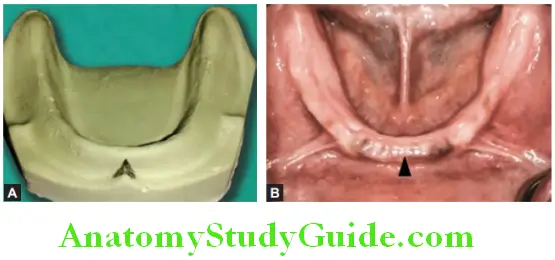
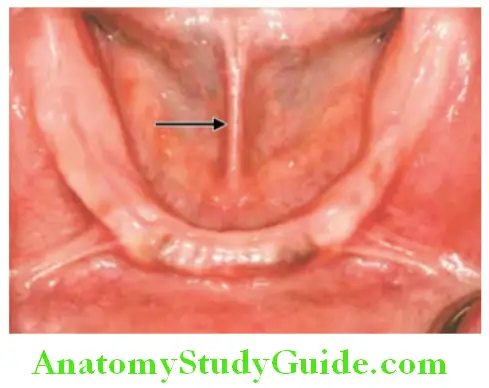
Genial Tubercle:
They are small bony protuberance two to three in number. Located lingually near midline area near inferior border of mandible, and serve as attachment for genioglossus and geniohyoid muscles (See arrow in figure). They become prominent in severely resorbed ridge cases, so in such cases relief should be provided to prevent discomfort. However, the denture needs to be extended beyond them to complete the sublingual seal.
Torus Mandibularis:
It is bony prominence located bilaterally lingually near premolar region. Surgical removal is usually indicated. Torus mandibularis is covered with thin mucosa so relief should be provided to prevent soreness in that area. Present only in 20% of population.

Valve Forming Structures (Limiting Areas)
Labial Frenum:
It is fold of fibrous band covered by mucous membrane at midline. It has attachment with orbicularis oris. Consider as active frenum. It should be properly housed in denture for enough clearance without compromising the seal.
Labial Vestibule:
It extends from labial frenum to buccal frenum. Overextension of denture in this region causes instability of denture or soreness of mucosa in this region. Muscle attachment in this area is near to the crest of the ridge which limits the extension of denture flange in this area. Recording of proper depth-width and proper contouring gives best esthetics to patient. Muscles in this region are incisivus, mentalis, and orbicularis oris (Im O).
Buccal Frenum:
Fold of mucous membrane. Buccal frenum is located in premolar region just distal to cuspid eminence. Single or double in number and broad fan shaped. It needs wider clearance due to broad shape. Located over depressor anguli oris muscle.
Buccal Vestibule:
It extends posteriorly from buccal frenum to the retromolar pad region bounded by residual alveolar ridge on one side and buccinator on the other side. This space is influenced by action of masseter muscle in the distobuccal border to produce a notch in the denture called as masseteric notch.
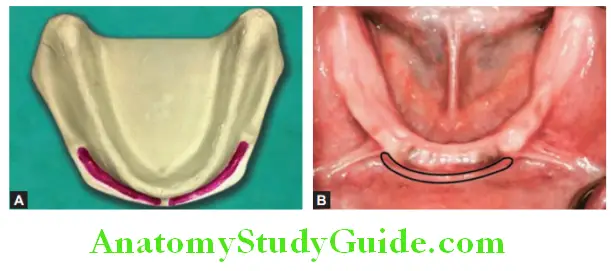
Lingual Frenum:
It is a fold of mucous membrane. It attaches base of the tongue to supragenial tubercle. It should be registered in function. It usually occurs as a narrow and single band. It is a highly resistant and active frenum. It produces lingual notch in impression. It overlies the genioglossus muscle.
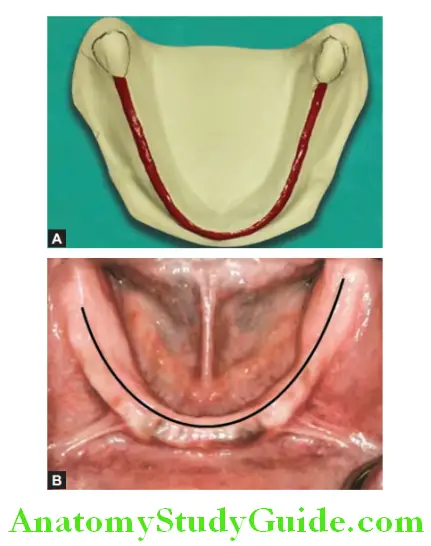
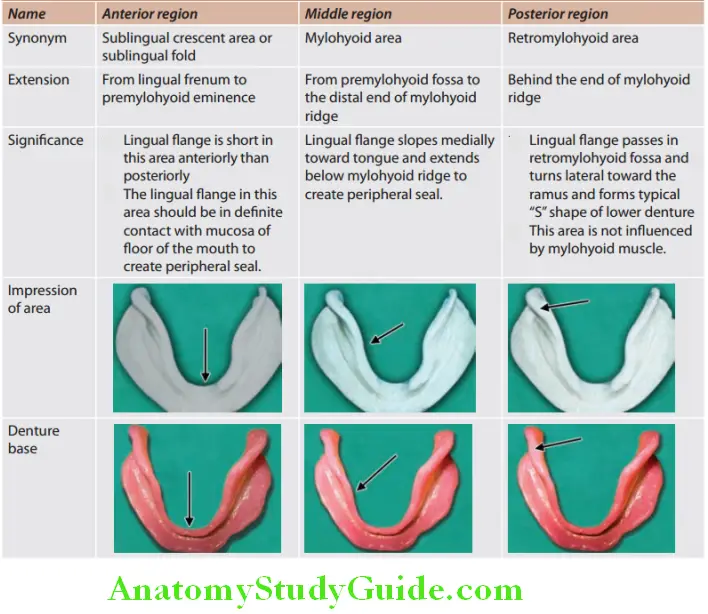
Alveololingual Sulcus:
It is space between tongue and residual alveolar ridge. It extends from lingual
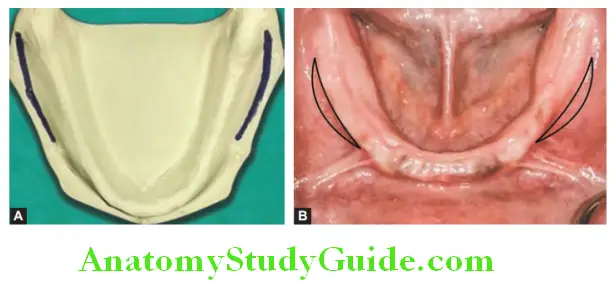
frenum to retromylohyoid curtain. While making impression, borders of impression should be in contact with the floor of mouth when tongue touches the upper incisor region. Overextension of denture in this region causes soreness or instability. The alveololingual sulcus can be divided in three parts.
Leave a Reply