Anatomy
Scalp Temple And Face Notes And Important Questions With Answers
Question 1: Why do infections of the superficial fascia of the scalp cause more pain?
Table of Contents
Answer: Superficial fascia has abundant fibrous tissue and a rich nerve supply.
Hence, infection of the superficial fascia irritates the nerve and one gets severe pain.
Read And Learn More: Head Anatomy Notes And Important Questions With Answers
Question 2:Why are sebaceous cysts and seborrhoea more frequently associated with the scalp?
Answer: The scalp has plenty of hair and sebaceous glands.
The ducts of sebaceous glands are prone to infection and get damaged by combing.
For this reason, the scalp is a common site for sebaceous cysts. Hence, sebaceous cysts and seborrhoea are more common.
Question 3: What is the “dangerous area of the scalp” and why is it called so?
Answer: The third layer of the scalp is loose areolar tissue. It is a dangerous area of the scalp.
An accumulation of blood in this area will not spread in the following directions.
1. It cannot descend in the neck because of the firm attachment of epicranial aponeurosis to the superior nuchal line.
2. It cannot descend laterally because of its attachment to the superior temporal line.
The only way it can spread is anteriorly. Hence, it accumulates deep in the eyelid and results in a black eye.
This results in damage to the eye hence it is called a dangerous area.
Question 4: What is “safety valve hematoma”? How the haemorrhage from the blood vessels of the scalp is arrested?
Answer: 1. Safety valve hematoma occurs due to the following reasons:
1. Fracture of the bone of the scalp, and
2. Intracranial bleeding (usually due to birth trauma in the newborn).
The symptoms of intracranial bleeding are delayed due to leakage of blood.
It spreads to the sub-aponeurotic layer from the fracture site.
It expands to accommodate large quantities of blood.
Since this hematoma delays the onset of symptoms of a serious condition, it is called safety valve hematoma.
2. By compressing at the site of injury, bleeding is arrested since underneath the scalp is the cranium which is a hard structure.
Question 5: Why do the wounds on the face bleed profusely?
Answer: The scalp has a profuse blood supply. It is supplied by 5 paired arteries.
These arteries pass through the dense connective tissue.
Ruptured arteries of any part of the body are constricted by the contraction of smooth muscles present in walls of the vessel.
The vessels in the scalp pass through the dense connective tissue.
The arteries of the scalp cannot overcome the resistance of the tough dens deep fascia.
Hence, they are kept open and they bleed profusely.
Question 6: What are the modifications of palpebral fascia?
Answer: The palpebral fascia of the two eyelids forms the orbital septum.
1. In upper eyelid becomes thick and forms tarsal plates or tarsi.
Tarsi are thin plates of condensed fibrous tissue located near the lid margins.
They give stiffness to the lids.
The upper tarsus receives two tendinous slips from the levator palpebrae superioris. I
- One from the voluntary part, and
- Another from involuntary part.
2. At the angles, it forms palpebral ligaments.
Question 7: What is stye (hordeolum)?
Answer: 1. Definition: It is a suppurative inflammation of one of the glands of Zeis.
It is a large sebaceous gland.
2. Clinical features
- The gland is swollen, hard, and painful.
- The lid is oedematous.
- Pus points near the base of one of the roots (follicle) of an eyelash.
Question 8: What is chalazion?
Answer: Definition: It is inflammation of a tarsal gland, causing a localized swelling pointing inward.
Modiolus
1. Modiolus (nave, pillar): It is a compact, mobile fibromuscular structure.
It is present at about 1.25 cm lateral to the angle of the mouth opposite the upper 2nd premolar tooth.
2. The five muscles interlacing to form the modiolus are:
- Buccinator,
- Zygomaticus major,
- Levator anguli oris,
- Depressor anguli oris
- Risorius.
3. Shape: Like a hub of a cart-wheel. The muscles radiate from it lie in different planes.
4. Palpation: It can be palpated between the opposed thumb compressing the skin at the angle of mouth and index finger simultaneously compressing the oral mucosa
at the same point.
5. Applied anatomy: The complex integrated movements of modiolar muscles help in biting, chewing, drinking, sucking, swallowing and speaking apart from the facial expressions.
Describe scalp under the following headings:
1. Layers,
2. Blood supply,
3. Nerve supply, and
4. Applied anatomy
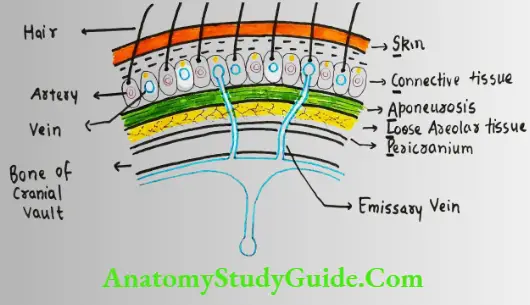
1. Layers: I. SCALPI
Skin: Skin is hairy and exceptionally thick. It contains plenty of sebaceous glands.
It is adherentto the underlying epicranial aponeurosis through th dense superficial fascia.
Connective tissue (superficial fascia): It is very dense and contains plenty of blood vessels and nerves.
I has the richest cutaneous blood supply in the body.
C. Aponeurosis (galea aponeurotica or epicranial aponeurosis): This contains occipitofrontalis muscle. It has
- Occipital, and
- Frontal belly.
- Occipital belly arises from
External occipital protuberance, and IL Highest nuchal lines and becomes continuous with epicranial aponeurosis.
Frontal belly arises from epicranial aponeurosis and merges with the procerus, corrugator supercilii and orbicularis oculi.
The direction of the fibres is anteroposterior. Thus, the occipital belly is attached to the bone and the frontal belly is attached to the dermis of skin.
Lose areolar tissue extends
- Posteriorly from highest and superior nuchal lines,
- Laterally from superior temporal lines, and
- Anteriorly into the eyelids.
fericranium: It is loosely attached to the surface of the bone except near sutures.
Hence, the fluid collected in this layer takes the shape of underlying bone.
2. Blood supply: Scalp has rich blood supply.
Arterial supply
In front of the auricle, Supraorbital artery (branch of ophthalmic artery), and Supratrochlear artery (branch of ophthalmic artery).
Superficial temporal artery (branch of external carotid artery).
Behind the auricle, it is supplied by
Posterior auricular artery (branch of external carotid artery), and
Occipital artery (branch of external carotid artery).
Note: Scalp is a site of anastomosis between branches of external and internal carotid arteries.
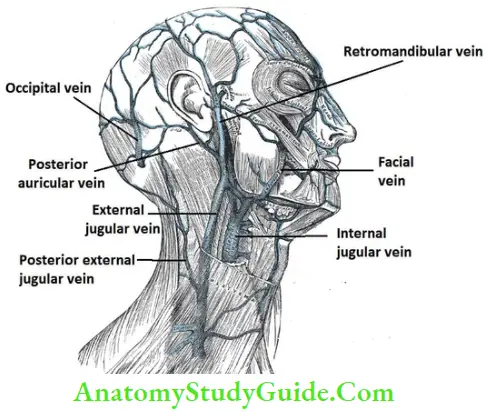
Venous drainage
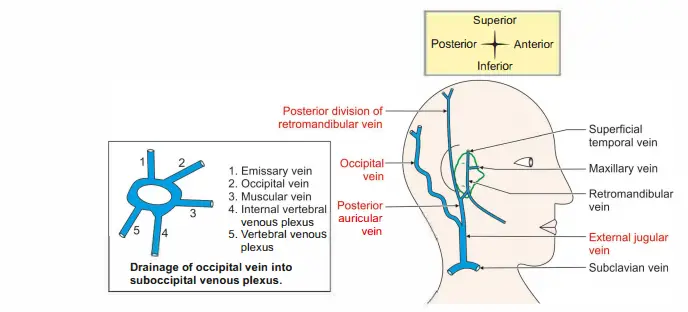
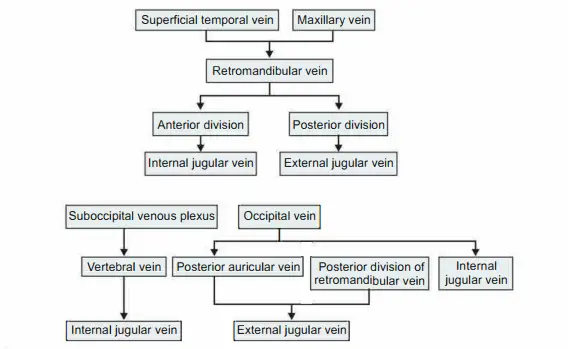
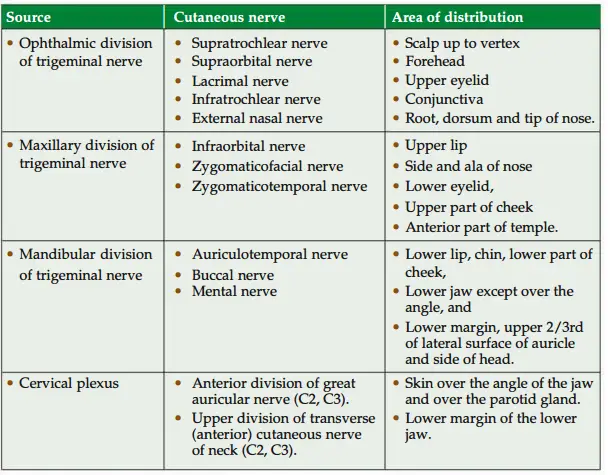
3. Nerve supply
Sensor
In front of auricle:
External jugular vein
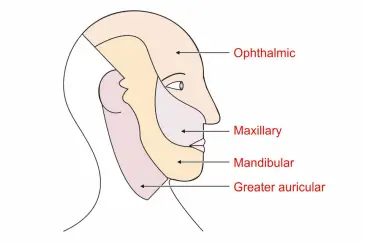
Supraorbital and supratrochlear, branches of ophthalmic division of trigeminal nerve.
Zygomaticotemporal a branch of zygomatic nerve which is a branch of maxillary division of trigeminal nerve.
Auriculotemporal nerve-mandibular division of trigeminal.
Behind the auricleI. Go To Posterior division of Great !!_icular nerve (ventral rami of C2-C3)
Lesser Occipital nerve. Ventral rami of (C2)
Greater Occipital nerve-dorsal ramus of C2 spinal nerve.
Third Occipital nerve-dorsal ramus of C3 spinal nerve.
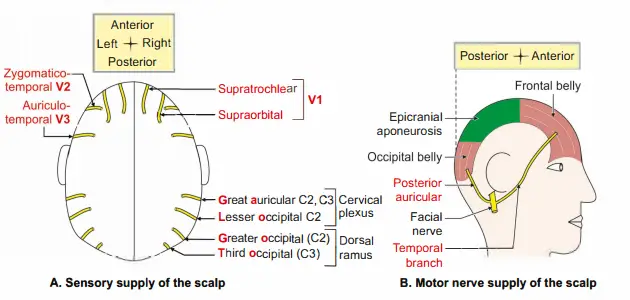
B. Motor
In front of the auricle: Temporal branch of facial nerve supplies frontal belly of occipitofrontalis.
Behind the auricle: Posterior auricular branch of facial nerve supplies occipital belly of occipitofrontalis.
Applied anatomy
First layer
Skin is thick and hairy.
It is the common site of sebaceous cyst.
The infection of the scalp behind the ear may cause transverse venous sinus infection.
It can be dangerous or fatal.
Second layer
The bleeding in second layer is profuse. This is because of two reasons:- The scalp has rich blood supply (five arteries on each side),
The tom vessels are prevented from constriction because the walls of the blood vessels are adherent to the dense connective tissue.
This prevents constriction of vessels.
The bleeding can be immediately arrested by compressing against hard bone, i.e. cranium.
As all thblood vessels of th scalp run frm periphery to centre, bleeding frm th scalp can easily be arrested by applying a tournit around th head.
Third layer: The direction of injury to the scalp decides the rate of healing of the wound.
There is rapid healing of the wound in injury parallel to direction of muscle fibres.
There is delayed healing of wounds, in injury perpendicular to the muscle fibres.
Fourth layer
This is the dangerous area of scalp. The infection from this layer spreads to the brain through emissary vein.
Accumulation of blood in this layer results in black eye.
Fifth layer
Bleeding in 5th layer takes the shape of underlying bone.
The condition is called cephalohaematoma.
Caput succedaneum: It is oedema occurring in and around scalp of newborn during labour.
Question 9:Why do the wrinkles of face tend to gap?
Answer: As the person ages, the skin loses its elasticity (resilience) which results into wrinkles , on the skin.
If the skin incision is not parallel to these cleavage or wrinkle lines (Langer lines), it has tendency to gap.
supranuclear lesion of facial nerve, only the lower part of the face is – paralysed.
Question 10:Why the upper part of face is spared?
Answer: The supranuclear lesions are also called upper motor neuron lesions.
It affects muscles of the lower½ of the face only.
The muscles of the upper½ of the face are spared because muscles of the upper½ of the face (muscles of forehead and eyebrows) are supplied by both cerebral hemispheres.
This is called bilateral cortical innervation.
Describe muscles of face under the following headings:
1. Action,
2. Nerve supply, and
3. Applied anatomy
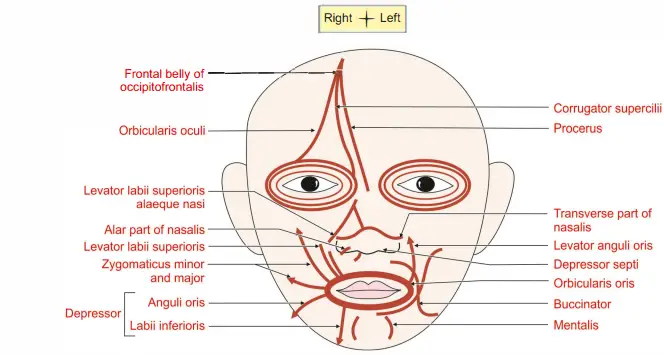
1. Action: The muscles of facial expression can be grouped as (mimetic muscles)
Muscles acting on the orifice of the orbit: These are subgrouped as constrictor (sphincters) and dilators.
Frontal belly of occipitofrontalis is responsible for elevation of eyebrows as in an expression of surprise and it also contracts in looking upwards.
The action is antagonistic to the orbital part of orbicularis oculi.
Corrugator supercilii drags the eyebrow medially and downward and protects the eye from bright sunlight.
It produces vertical wrinkles of the forehead.
Orbicularis oculi has three parts.
Palpebral part closes the eye gently as in sleep and blinking.
Orbital part closes the eye firmly as in dust storm.
Lacrimal part dilates the lacrimal sac.
Muscles acting on the orifice of the nose
Procerus (extended, tall). It is extended part of frontalis. It produces transverse wrinkles across bridge of nose as in frowning.
Nasalis has two parts.
Transverse part called compressor naris. It compresses the nasal aperture.
Alar part called dilator naris. It dilates the anterior nasal aperture in deep inspiration.
Depressor septi dilates anterior nasal aperture in anger.
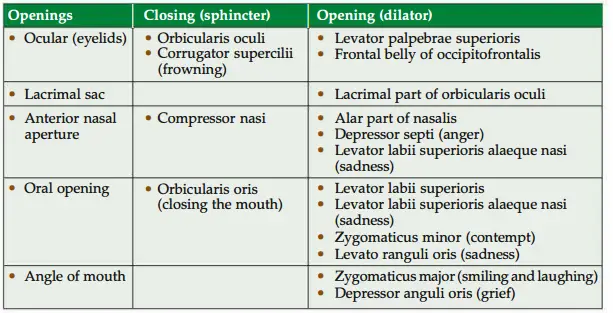
Muscles acting on the orifice of the mouth
Closure: Orbicularis oris closes the mouth.
Dilators
Subcutaneous layer: Risorius (risus-to laugh).
Superficial layer:
Zygomaticus major draws the angle of mouth upward and laterally as in laughing.
Zygomaticus minor elevates and everts upper lip.
Levator labii superioris alaeque nasi elevates and everts the upper lip and dilates the nostril.
Middle layer
Depressor anguli oris draws the angle of mouth downward.
Levator anguli oris
Depressor labii inferioris draws angle of mouth downward and somewhat laterally as in expression of irony.
Levator labii superioris elevates the lip.
Deeper layer
Mentalis protrudes the lower lip.
Buccinator flattens the cheek and forcibly expels the air between the lips (whistling).
Nerve supply!: The muscles of the face are developed from 2nd pharyngeal arch and the nerve of the 2nd pharyngeal arch is facial nerve.
Hence, all the muscles are supplied by facial nerve.
Applied anatomy
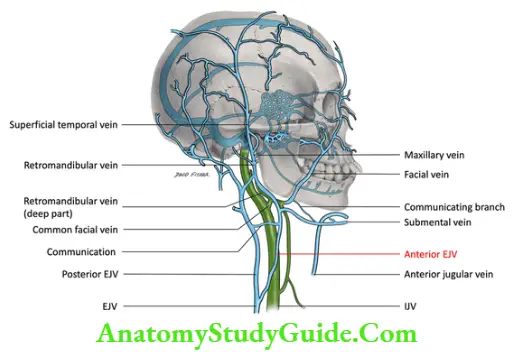
Describe facial vein under the following headings:
1. Formation; 2. Relations; 3. Tributaries; 4. Termination; 5. Applied anatomy
1. Formation: The angular vein receives superior labial vein and continues as facial vein.
2. Relations
- It lies deep to
- Zygomaticus major,
- Riorius, and
- Platysma.
- From above downwards, it lies superficial to
- Buccinator,
- Body of mandible,
- Masseter,
- Posterior belly of digastric, and
- Stylohyoid muscle.
- At termination, it crosses: a. Internal carotid artery, b. External carotid artery,
- Hypoglossal nerve, and d. Loop of lingual artery.
3. Tributaries
- Superior ophthalmic vein,
- Vein from alar nasi,
- Superior labial vein,
- Buccal vein,
- Deep facial vein from pterygoid plexus,
- Inferior labial vein,
- Masseteric vein,
- Tonsillar vein,
- Submental vein, and
- Submandibular vein
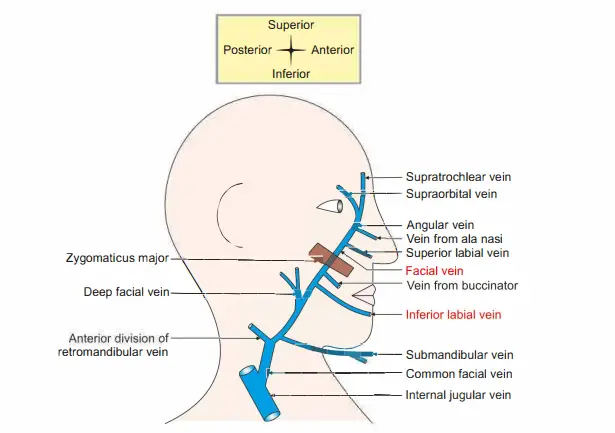
4. Termination: Common facial vein terminates into internal jugular vein.
5. Applied anatomy
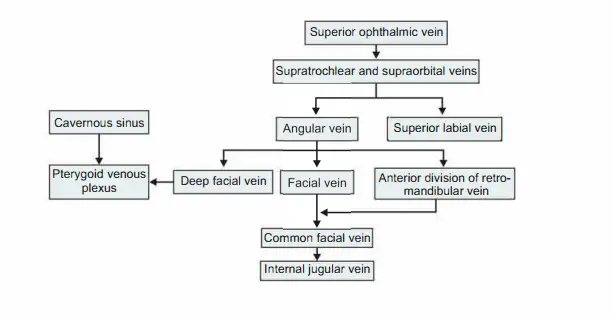
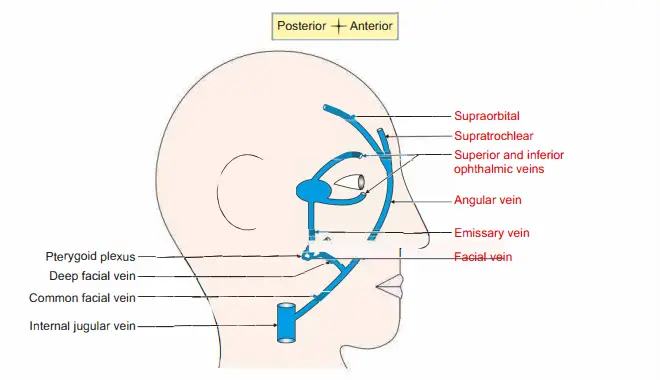
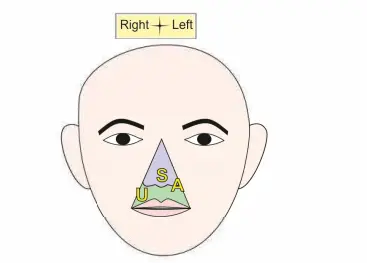
Infection of the face can spread to intracranial venous sinus. Hence, the veins draining Upper lip Septum of nose, and Adjoining nose lying between angular and deep facial veins forms the dangerous area of the face.
I. ..A is the dangerous area of face.
Following are the routes for the spread of infection.
Angular vein + superior ophthalmic vein + cavernous sinus.
Deep facial vein + pterygoid venous plexus + emissary vein + cavernous sinus.
The spread of septic emboli from the infected area to cavernous sinus can cause serious complications because of following reasons.
Veins of the face do not have valves.
- Veins of the face lie on facial muscles.
- There is no deep fascia on the face.
- The movements of the facial muscles may facilitate the spread of septic emboli to cavernous sinus.
Question 11:Why the facial muscles are called “muscles of facial expression”?
Answer: The muscles of face are not inserted on bone but in the skin.
Since there is no deep fascia in the face, contraction of these muscles causes contraction of some part of skin (on the face. It acts as a medium to express the emotional feelings.
Hence, facial muscles are called muscles of facial expression.
Question 12: What is the nerve supply of facial muscles?
Answer: 1. All the muscles on the face are supplied by facial nerve except levator palpebrae superioris which is supplied by oculomotor nerve.
2. Majority of the muscles on the face are muscles of facial expression.
However, there are exceptions.
These are buccinator and platysma.
They are supplied by facial nerve.
3. The muscles present on the face but included as muscles of mastication are temporalis, masseter, medial andlateral pterygoid.
These aresupplied by mandibular nerve, branch of trigeminal nerve (Vth cranial nerve).
Deep facial vein
Introduction: It is a communicating channel that conncts the facial vein to pterygoid venous plexus .
1. Course: It leaves the facial vein before it crosses the lateral surface of masseter and to the ramus of mandible.
2. Communications: It is connected to the cavernous sinus by the emissary veins passing through the
- Foramen lacerum,
- Foramen ovale, and
- Foramen spinosum.
3. Peculiarities: It has no valves.
4. Applied anatomy
The dangerous area of face lies between angular and deep facial veins.
The infection from the upper lip and the lower part of the nose can spread through the deep facial vein and cause cavernous sinus thrombosis.
The movements of the facial muscles may facilitate the spread of septic emboli.
Dangerous area of face
Infection of the face can spread to intracranial venous sinus.
Hence, the veins draining the following area is called dangerous area of face.
1. Area:SAI Upper lip.
Septum of nose.
Adjoining part of nose and lip lying between angular and deep facial veins forms the dangerous area of the face.
2. Following are the routes for the spread of infection.
- Facial vein + deep facial vein + pterygoid venous plexus + cavernous sinus.
- Angular vein + superior ophthalmic vein + cavernous sinus.
3. The spread of septic emboli from the infected area to cavernous sinus can cause serious complications because of following reasons.
- Veins of the face do not have valves.
- Veins of the face directly lie on the muscles of face.
- There is no deep fascia on the face.
- The movements of the facial muscles may facilitate the spread of septic emboli to cavernous sinus.
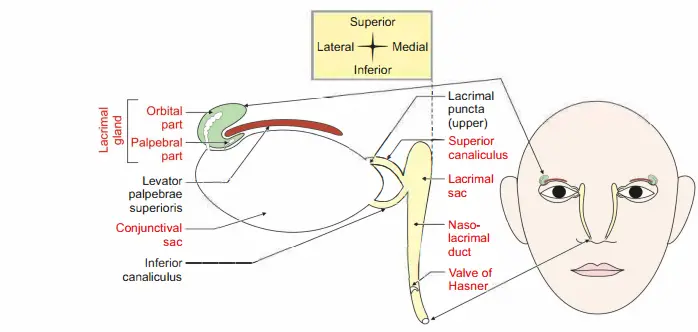
Question 13:What are the constituents of lacrimal apparatus?
Answer: It consists of
1. Lacrimal gland
- Orbital part, and
- Palpebral part
2. Conjunctiva! sac
3. Punctum
4. Canaliculus
- Superior, and
- Inferior canaliculus
5. Lacrimal sac
Nasolacrimal duct
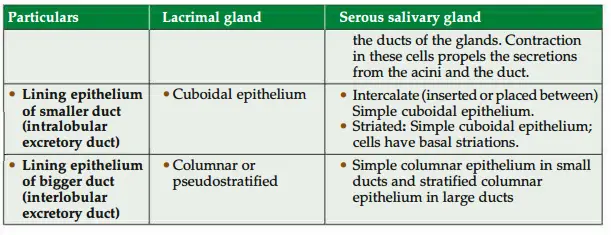
Question 14: What are the structural diffrences between lacrimal gland and serous salivary gland?
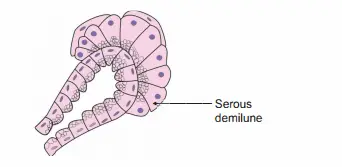
Question 15: microscopic structure of serous demilune
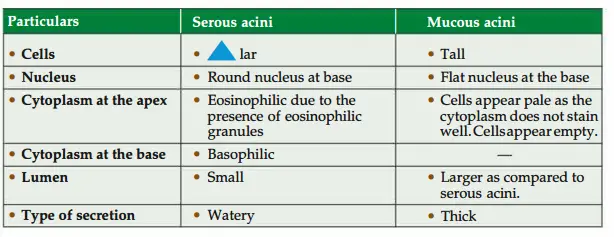
Question 16: Enumerate the diffrence between serous and mucus acini.
Question 17: What are serous demilunes?
Answer:
- Some of the mucous acini are capped with serous cells.
- They are arranged as a half-moon.
- Hence, they are called serous demilunes.
Where do we get myoepithelial cells in the body? How will you identify – them?
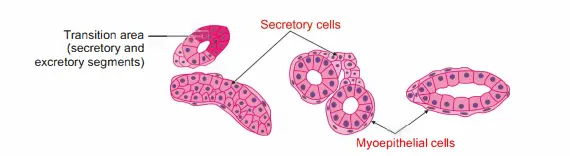
- Site
- Ducts: Between the epithelium and the basement membrane of the ducts.
- Sweat gland: There are cuboidal secretory cells of the sweat gland.
- At the base of the secretory cells, there are numerous myoepithelial cells.
- Identifying features :
- The cells are thin and spindle-shaped.
- They are located at the base of the secretory cells
Question 18: What are the functions of saliva?
Answer: 1. The saliva lubricates the luminal surface of th upper digestive and respiratory tracts.
2. It moistens the food to help in deglutination.
3. It initiates the digestion of carbohydrates by the enzyme salivary amylase.
4. It contains lysozyme and irnmglobulin. They are bactericidal in nature.
Describe lacrimal apparatus under the following heads:
1. Components,
2. Blood supply,
3. Nerve supply, and
4. Applied anatomy
1. Components: Lacrimal gland with ducts, conjunctiva! sac, lacrimal caruncle, lacrimal punctate, lacrimal canaliculus, lacrimal sac and nasolacrimal duct.
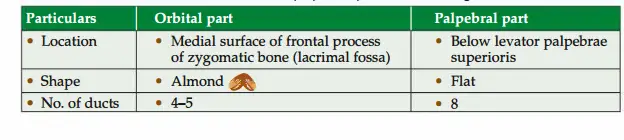
Lacrimal gland: Table 2.6 shows different parts of the lacrimal gland.
- Functions of lacrimal fluid (tears):
Maintains Transparency of cornea.Expresses emotion, Acts as bactericidal, Renders nourishment to the cornea, and Keeps the orbital Surface of the conjunctiva moist. - Conjunctiva
Gross features: It is a transparent membrane covering the sclera and lining the inner surface of the eyelid.
Conjunctiva! sac: It is a potential space between two eyelids and the cornea/sclera in the closed position of eyelids. It consists of
Orbital part which is in contact with the sclera and cornea.
Palpebral part: It is highly vascular and adherent to the tarsal plate. It lines the eyelid.
Nerve supply
Ophthalmic division of trigeminal nerve.
Maxillary division of trigeminal nerve.
Blood supply: Palpebral branch of the ophthalmic artery. - Puncta with lacrimal canaliculi: Each lacrimal canaliculus begins with punctum.
Length of canaliculus:10 mm. It has
L Vertical part-2 mm
Horizontal part-8 mm
It is lined by stratified squamous non-keratinized epithelium. It opens in the
lateral wall of the lacrimal sac behind the medial palpebral ligament. - Lacrimal sac: It is a membranous sac, that continues with the nasolacrimal duct.
It is a blind pouch. Superiorly, it measures 12 x 5 mm.
It continues inferiorly with the nasolacrimal duct. - Relations of lacrimal sac
Anterior
Medial palpebral ligament.
Orbicularis oculi muscle.
Medially: Lacrimal groove. - Laterally: Lacrimal fascia and lacrimal part of orbicularis oculi.
- Nasolacrimal duct: It is a membranous passage of 18 mm long.
It runs from the lower end of the lacrimal sac and opens in the inferior meatus of the nose.
The lower end of the duct is guarded by the valve of Hasner.
It prevents the backward flow of fluid.
2. Blood supply
Arterial supply: Lacrimal artery, a branch of the ophthalmic artery.
Venous drainage: The lacrimal vein drains into an ophthalmic vein.
Nerve supply!
Sensory: The sensations are carried by a lacrimal branch of the ophthalmic division of the trigeminal nerve.
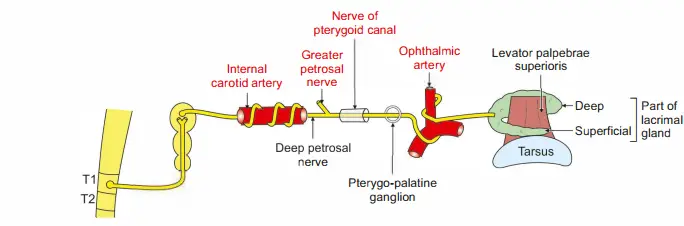
Sympathetic: It is vasomotor in function (Fig. 2.14).
Preganglionic fibers arise from the spinal cord (Tl-TS segments) and goes to the superior cervical sympathetic ganglion.
Postganglionic fibers are the plexus around the internal carotid artery and around the ophthalmic artery.
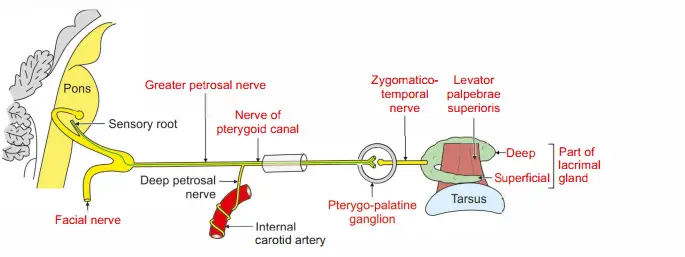
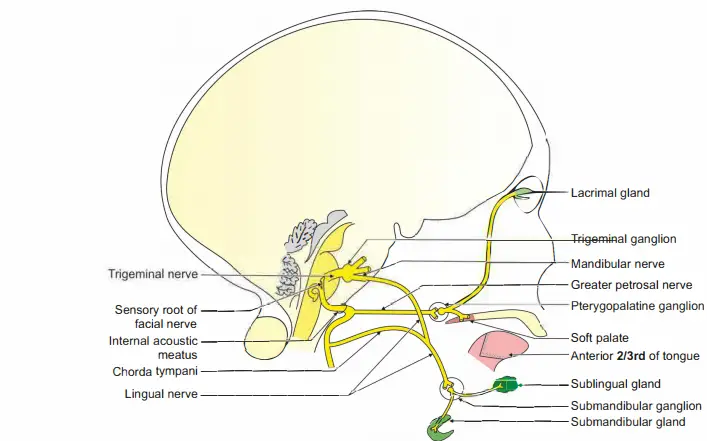
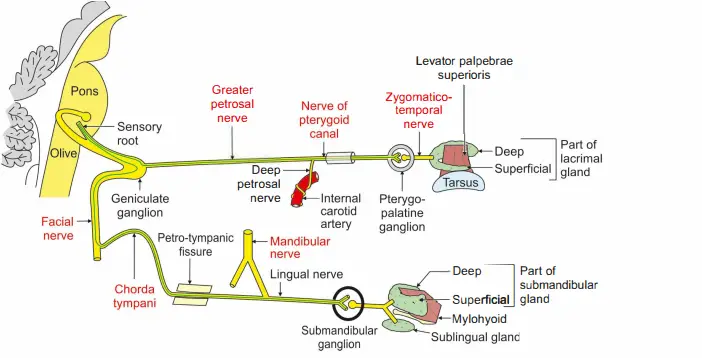
The parasympathetic nerve is secretomotor in function. It is carried by the facial nerve➔ pterygopalatine ganglion➔ maxillary nerve (VII- pterygopalatine ganglion-V2).
Preganglionic fibers arising from the lacrimatory nucleus present in the pons, pass via the facial nerve, and greater petrosal nerve and join with the deep petrosal nerve to form the nerve to the pterygoid canal.
The fibers are relayed in the pterygopalatine ganglion.
Postganglionic fibers pass through the maxillary nerve (zygomaticotemporal) lacrimal nerve-lacrimal gland.
The parasympathetic nerve is secretomotor in function.
It is carried by facial nerve➔ pterygopalatine ganglion➔ maxillary nerve (VII- pterygopalatine ganglion-V2).
Preganglionic fibers arising from the lacrimatory nucleus present in the pons, pass via the facial nerve, and greater petrosal nerve and join with the deep petrosal nerve to form the nerve to the pterygoid canal.
The fibers are relayed in the pterygopalatine ganglion.
- Facial nerve
- Greater petrosal nerve
- Nerve of pterygoid canal carotid artery
- Zygomatico- Levator temporal palpebrae nerve superioris
Secretomotor fibers of lacrimal gland uperDeepficialJ lacrimalglandPart of Postganglionic fibers pass through maxillary nerve (zygomaticotemporal)
lacrimal nerve-lacrimal gland.
Applied anatomy
Dacryoadenitis (dacry-tear) is the inflammation of the lacrimal gland.
Dacryocystitis is inflammation of the lacrimal sac and presents with pain, edema, and redness.
Dacryocystectomy is the removal of the lacrimal sac.
Removal of the palpebral part is equal to the removal of the entire gland because the ducts of the orbital part pass through the palpebral part.
Epiphora (Epiphora-sudden burst)-the overflow of tears.
Question 19: What is dacryocystitis?
Answer: Inflammation of the lacrimal sac is called dacrocystitis.
Question 20: What is the nature of the lacrimal gland?
Answer: It is a serous gland.
Question 21:What are the parts of the lacrimal gland?
1. Orbital part
2. Palpebral part
Orbicularis oculi
- Scalp, Temple, and Face
(Orbiculus—oit, oculi-eyeball) - Introduction: It is a muscle of the face, the sphincter of the orbital fissure.
- Attachments: It has three parts:
- Palpebral part: It is confined to the lids. It arises from the medial palpebral ligament.
- It is inserted into the lateral palpebral raphe.
- Orbital part: It extends beyond orbit. It arises from
- Nasal part of the frontal bone
- Anterior lacrimal crest
- Frontal process of the maxilla: It forms concentric rings and returns to the point of -origin.
- Lacrimal part (deeper part): It is attached medially to the
- Posterior lacrimal crest, and Lacrimal sac,
- They are inserted into the upper and lower eyelids.
Nerve supply
Mainly by a zygomatic branch of the facial nerve.
It is also supplied by the temporal branch of the facial nerve.
Actions
The palpebral part closes the eyelid gently.
Orbital and palpebral parts together closes the eyelid forcibly.
Levator palpebrae superioris is the opponent of upper palpebral fibres of orbicularis oculi.
Occipitofrontalis opposes the orbital part.
Development: They are developed from the mesoderm of the 2nd pharyngeal arch.
Applied anatomy : Infranuclear lesion of the facial nerve leads to paralysis of orbicularis oculi.
Hence, the patient cannot close the eyelid tightly.
Frequent closure of eyelids is required for the normal drainage of tears through the lacrimal ducts.
Due to paralysis of orbicularis oculi, there is overflowing of tears through the eyelid and expose keratitis.
Enumerate the branches of facial artery on the face
1. Inferior labial,
2. Superior labial,
3. Lateral nasal, and
4. Angular artery.
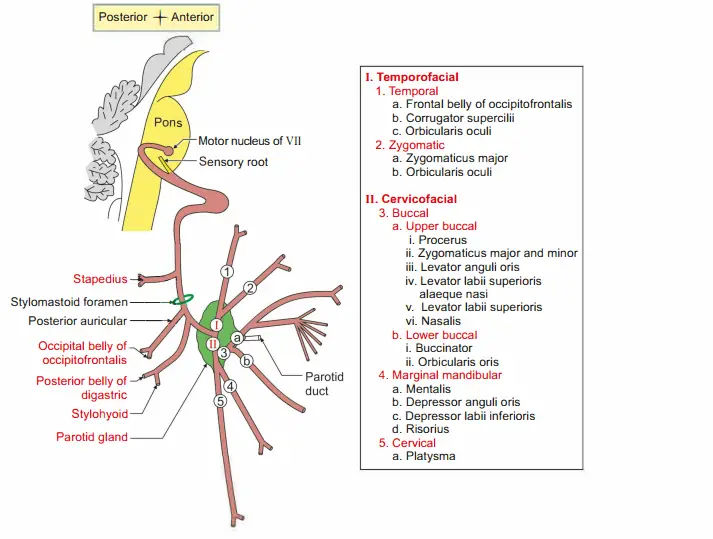
Describe facial nerve under the following headings:
1. Course and relations
2. Branches
3. Applied anatomy
It is a nerve of 2nd pharyngeal arch.
1. Course and relations
Intraneuronal (Fig. 2.16)
Motor root arises from motor nuclei of facial nerve situated in deep part of pons.
It winds around abducent nucleus. It forms a bulging in the floor of IVth ventricle called facial colliculus.
It is due to the phenomenon of neurobiotaxis.
The nerve fibres have a tendency to migrate in the direction from which they receive their stimuli.
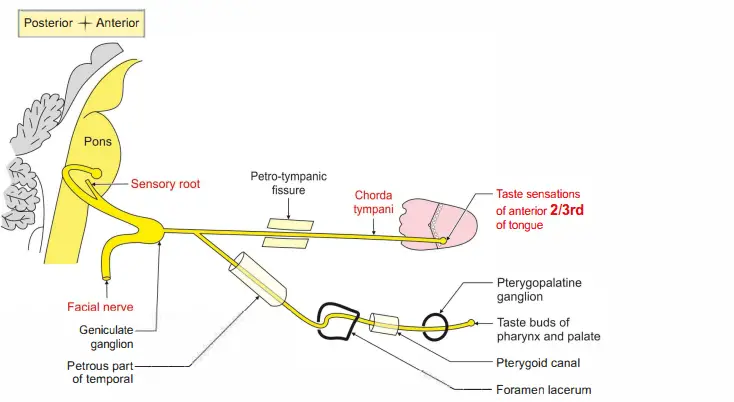
Sensory root (nervus intermedius) is formed by
Superior salivatory nucleus and lacrimatory nucleus.
Nucleus tractus solitarius.
Both the roots emerge at the junction of pons and olive.
Extraneuronal: Divided into three parts
First part: It passes through the internal acoustic meatus.
It reaches anterosuperior angle of the medial wall of the middle ear cavity. It bends to form second part.
It forms a bulging at the bend called geniculate ganglion.
Second part: It runs horizontally backwards along medial wall of tympanic cavity.
It lies above promontory and fenestra vetibuli and runs to the posterior part of medial wall.
Third part: It is posterior to posterior wall of middle ear cavity.
Runs vertically downwards and comes outside the cranium through stylomastoid foramen.
Extracranial: It turns anteriorly and pierces the posteromedial surface of parotid gland.
It emerges from anteromedial surface of parotid gland.
Terminates in the parotid gland: By dividing into terminal branches.
Branches
Intracranial
First part: No branches:
At the junction of 1st and 2nd parts, greater petrosal nerve arises.
It carries secretomotor fibres to the lacrimal gland.
Second part:
Sympathetic branches to middle meningeal artery.
Branch to lesser petrosal nerve, by which it reaches the otic ganglion.
Third part:
Stapedial branch: It passes through small canal and supplies stapedius muscle.
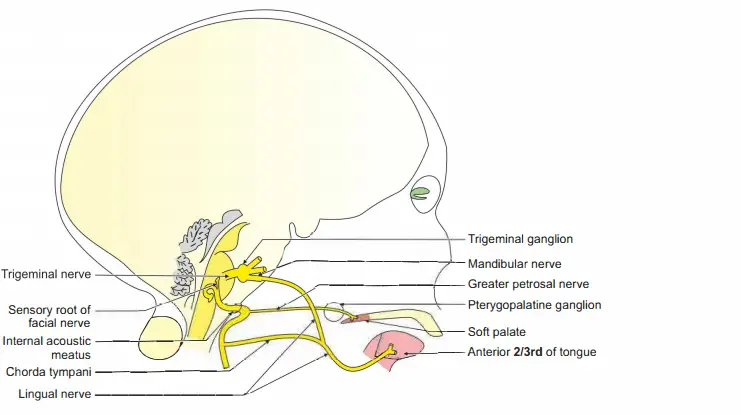
Chordatymni nerve: Itjoins ligul nerve and carries tate fires frmanteior 2/3rd oftongu.
Italsocarries secretomotor fires tosubmandibulargland .
Communicating branch to vagus.
Extracranial
- Posterior auricular branch gives communicating branch to great auricular and lesser occipital. It divides into
- Auricular branch to auricularis posterior.
- Occipital branch to occipital belly of occipitofrontalis.
- Digastric branch to posterior belly of digastric.
- Stylohyoid branch to stylohyoid muscle.
- Terminal
- Temporal branch to
- Frontal belly of occipitofrontalis,
- Muscles of external ear
- Auricularis superior
- Auricularis anterior
- Corrugator supercilii.
- Zygomatic branch to orbicularis oculi
- Buccal
- Upper (lower zygomatic)
- Zygomaticus major
- Zygomaticus minor
- Levator labii superioris
- Levator labii superioris alaequae nasi
- Levator anguli oris
- Lower
- Buccinator
- Orbicularis oris
- Mandibular branch to risorius.
- Cervical branch to platysma
Pes anserinus (pes-foot, anser-goose)NEET: Branches of the facial nerve in the substance of parotid gland form a network called pes anserinus.
This divides the parotid gland into superficial and deep parts.
Pes anserinus
1.Branches of facial nerve
2.Muscles attached to upper part of medial surface of tibia.
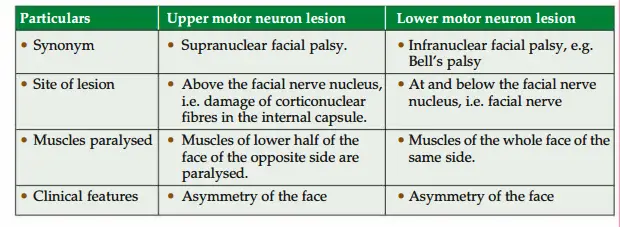
3. Applied anatomy Upper and lower motor neuron lesion of facial nerve.
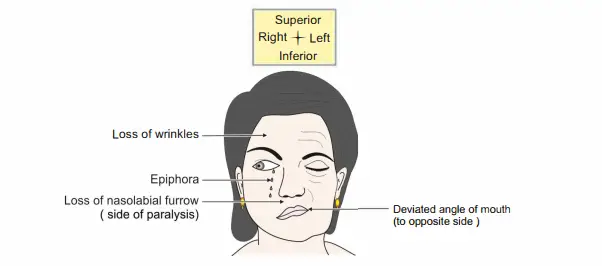
Note: While attempting to close the right eye (paralyzed side), the eye does not close and the eyeball rotates superiorly and laterally
Upper and lower motor neuron lesions of facial nerve
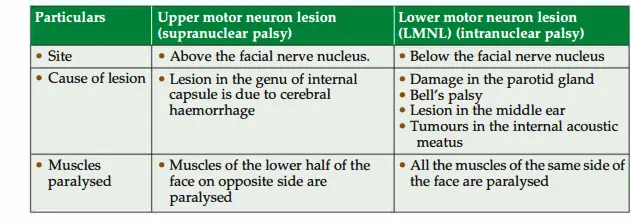
The difference in the upper and lower motor neuron lesions is displayed in Table 2.7.
Lower motor neuron lesion of facial nerve
The causes, and manifestation of lower motor lesion are described below.
1. Lesion of facial nerve distal to stylomastoid foramen: The lesion of facial nerve is due to vertical incision of the parotid gland.
2. Lesion of facial nerve at the stylomastoid foramen: It results in Bell’s palsy.
The ‘Bell’s palsy’ is the lower motor neuron type of facial palsy (paralysis of muscles of facial expression).
It occurs due to inflammation of facial nerve in the facial canal at the stylomastoid foramen.
The exact cause of inflammation is not known, but it is thought to be due to viral infection.
It causes inflammation and oedema of facial nerve.
It results in compression of facial nerve in the facial canal.
Pain of variable intensity behind the ear precedes facial weakness which develops over 48 hours period.
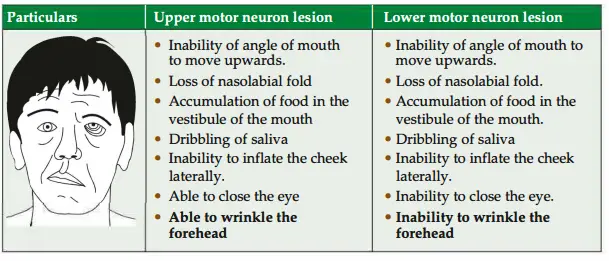
3. Characteristic features (All muscles of whole face are affected on the side of paralysis.)
- Facial asymmetry: Due to unopposed action of muscles of opposite side.
- Loss of wrinkles on forehead: Due to paralysis of fronto-occipitalis.
- Inability to close the eye (wide palpebral fissure): Due to paralysis of orbicularis oculi.
- Inability to move the angle of the mouth upwards and laterally during laughing due to paralysis of zygomaticus major.
- Loss of nasolabial furrow due to paralysis of levator labii superioris alaeque nasi.
- Accumulation of food in the vestibule of the mouth due to paralysis of the buccinator.
- Dribbling of saliva: Due to paralysis of orbicularis oris.
- Inability to inflate the cheek properly: Due to paralysis of buccinator muscle.
4. Lesion in the vertical course of the facial nerve within the mastoid bone results in the
- Loss of taste sensation on the anterior two-thirds of the tongue on the side of the lesion.
- There is loss of secretion from submandibular salivary gland; however, lacrimation and the stapedius reflex would be normal.
- A lesion in the middle ear segment of the nerve (tympanic) does not affect lacrimation but results into ipsilateral hyperacusis due to paralysis of stapedius.
5. Lesion at or proximal to the geniculate ganglion (translabyrinthine) produces diminished lacrimation on the same side, as well as disturbance in function of the other branches.
After regeneration, th parasympathtic secretomotor fires intended for salivary glands grow, and join the secretomotor fibres intended to supply the lacrimal gland; the anticipation of food then produces lacrimation, instead of salivation (syndrome of crocodile tears or Bogard syndrome)NEET_ The specific feature of this syndrome is paroxysmal lacrimation during eating.
Exact cause of lesion is not known. Most often it is due to viral infection leading to ro oedema and inflammation of the nerve.
Upper motor neuron lesion
1. Causes: It is due to damage of corticonuclear fibres. The lesion may be
- Facial nerve nucleus in the pons or
- Above the nucleus.
The main cause is lesion in the internal capsule.
2. Manifestations:
- Supranuclear lesions produce upper motor neuron type of paralysis.
The muscles of the lower half of the face of opposite side are paralysed.
The muscles of the upper half of the face are normal because they are bilaterally innervated. - Effects of upper motor neuron lesion: The patient is able to wrinkle the skin of his forehead, but he is not able to perform the actions of the muscles oflower 1/2 of these
(as they have unilateral innervation from the cerebral hemisphere hence paralyzed).
Question 18: What are the functions of buccinator muscle?
Answer: 1. It flattens cheek against gums and teeth.
2. It prevents accumulation of food in the vestibule.
3. This is the whistling muscle.
Leave a Reply