Treatment Guidelines In The 1990s The Nhlbi Report
In the summer of 1991, the National Heart, Lung, and Blood Institute (NHLBI) released the most comprehensive set of guidelines ever published in the United States for diagnosing and managing asthma.
Table of Contents
This eight-chapter report, written by a panel of American experts in the field of asthma and allergy chaired by Dr. Al Sheffer of Harvard Medical School, is designed to set a gold standard for all primary-care physicians and health providers who treat asthma.
What provoked the need for such a manuscript? The alarming increase in asthma hospitalizations and mortality seen in the 1980s is one reason. Economics is another. U.S. asthma-related healthcare expenses exceeded four billion dollars in 1988.
Read And Learn More: Air Pollution Asthma Complications Treatment Guidelines
The last and most important reason for this report is that new research findings have led to dramatic changes in the way asthma should be treated.
While most if not all asthma specialists were aware of these alterations in asthma therapy, many primary physicians were not. This NHLBI report, an outgrowth of the National Asthma Educational Program, will have a profound effect on the treatment of asthma.
It reflects the current state of the art concerning the underlying cause of asthma and presents detailed recommendations for the diagnosis and treatment of asthma.
While the NHLBI report is mainly directed at primary-care doctors, it will benefit all healthcare providers who deal with asthma, including respiratory therapists, health educators, nurse practitioners, school nurses, social workers, and psychologists.
The recommendations in the NHLBI report are based on classifying asthma into the following three categories based on asthma’s severity:
- Mild episodic asthma,
- Chronic moderate asthma, and
- Chronic severe asthma.
While such a classification may seem overly simplistic, it serves as an instrument that allows the healthcare provider (or patient or family) to assess the level of severity of asthma appropriately and follow a preconceived stepwise treatment plan.
It is given that asthma is a highly variable disease, and patients can fluctuate from one category to another at any time.
The critical treatment decisions in the NHLBI medication programs are based on a stepwise care approach in which the doses and frequencies of asthma medications are increased or decreased according to the severity of asthma.
Before I summarize the principles and rationale of asthma drug therapy presented in the NHLBI report in layman’s terms, I need to discuss the use of the peak flow meter, which plays a crucial role in the implementation of the NHLBI decision-making guidelines.
Peak Flow Meters
Pulmonary function or breathing tests are essential yardsticks in the diagnosis and management of asthma. These breathing tests can be compared to monitoring blood pressure in people with hypertension and monitoring blood sugar levels in diabetics.
What is the peak expiratory flow rate (commonly called the PEFR)? This measurement is the flow velocity or amount of air a person can exhale during a forced expiration after taking as full a breath as possible PEFR can be measured by a simple, relatively inexpensive portable device called a peak flow meter.
Which measures the amount of air in liters (one liter is about a quart) exhaled per minute. Even though these inexpensive and easy-to-use devices have been available for a decade, it is only recently that peak flow meter use has been recommended as a routine means of monitoring the course of asthma.
Poor perception of the severity of asthma is a well-known factor in patients exhibiting asthma relapses. Studies have shown the peak flow meter to be a much more accurate instrument than a stethoscope in assess- ing the severity of an asthma relapse.
Peak Flow Meter Applications
The peak flow meter has many uses. It can assess the severity of acute or chronic asthma in the healthcare provider’s office or the emergency room. The peak flow meter can be used before and after exercise to determine the presence or absence of EIA.
The peak flow meter can help the patient or family monitor asthma at home and guide the need to decrease or increase asthma medications. School personnel can use the peak flow meter to appraise the student who experiences acute asthma in the gymnasium, on the playing field, or in the classroom.
The peak flow meter is a very valuable addition to new asthma drug studies. Lastly, the peak flow meter is very helpful in detecting what type of occupational exposure may be triggering asthma in the workplace.
The peak flow meter is not a perfect instrument. Two limitations of the peak flow meter are the following:
- It is effort dependent; in other words, it depends on the patient’s ability and willingness to exhale as hard and as fast as possible and
- Peak flow meters measure only larger size airway functions. Asthma that is affecting the small airways only may go undetected by the peak flow meter.
Patient and family education is of the utmost importance if the peak flow meter is to be an effective instrument. Education should include how and when to use the peak flow meter, how to record peak flow rates, how to interpret the readings, and when to communicate with healthcare providers.
Most adults and children (occasionally even three- or four-year-olds) can be taught to generate a peak expiratory flow rate. As the PEFR is effort-dependent, patients need to be coached to put forth their best effort.
Peak flows can be recorded in a notebook, table, or graph. Many peak flow meters provide charts on which peak flow rates can be recorded. The NHLBI guidelines recommend that peak flow decisions be based on the patient’s “personal best” rather than by using a percentage of a normal predicted value.
Many people exhibit a wide variation between their morning and evening peak flow rates. A 20 percent swing in peak flow readings can be a normal variation on a day-to-day basis. Those patients who tend to drop their peak flows in the morning are called “morning dippers.
” A person’s personal best peak flow rate often occurs in late afternoon or evening after maximum asthma therapy. Sometimes a course of oral cortisone may be needed to establish that personal best.
Our practice usually advises new asthma patients to record their peak flow rates two to three times a day for a few weeks or longer after they have been placed on daily asthma medications. Once their asthma stabilizes, the peak flow rates can be charted when asthma warning signs occur or during an obvious asthma relapse.
Dr. Guillermo Mendoza and Dr. Thomas Plaut strongly recommend using a zone system similar to traffic lights to simplify the use of the peak flow meter. Three zones are established based on the individual’s personal best, predicted value, or the higher of these two numbers.
The green zone ranges from 80 to 100 percent of personal best and signals a “go,” an all-clear signal that the asthma is stable and that routine treatment should continue.
The yellow zone ranges from 50 to 80 percent of the personal best and indicates that the patient should proceed with caution, an acute relapse may be imminent, and asthma medications need to be increased.
The red zone, below the 50 percent level of personal best, signals a red light, a dangerous medical alert. Bronchodilator drugs should be administered and health-care providers should be notified if peak flow measurements do not immediately return to the yellow or green zone.
These suggested zones are general guidelines at best and specific asthma therapy should be individually tailored by the healthcare provider, patient, and family.
While some physicians advocate the use of peak flow meters for all asthmatics, others feel that the usefulness of peak flow meters is overstated and that the widespread use of peak flow meters is unnecessary, as it results in too intense a focus on asthma by the family and patient.
Dr. Donald Cockroft, professor of respiratory medicine at the University Hospital in Saskatchewan, Canada, is less than enthusiastic about using peak flow meters in the adult population. He feels that only 5 percent of his adult patients have the type of asthma in which home peak flow measurements are helpful.
Cockroft agrees that peak flow readings are helpful to a physician attempting to diagnose occupational or exercise-induced asthma. He feels that peak flow meters are more beneficial in the management of children with moderate to chronic asthma.
In contrast, Dr. Thomas Plaut feels that any patient who requires daily asthma treatment needs a peak flow meter. The NHLBI guidelines strongly state that all patients with asthma should utilize peak flow meters.
A recent study by Dr. Holly Pinzone, from the University of Ohio, published in the Annals of Allergy studied the predictability of peak flow meters in ten asthmatic children. Her results supported the conclusion that peak flows improve the predictability of asthma relapses.
Dr. Frank Twarog at Harvard Medical School appropriately points out in an accompanying editorial that some physicians use peak flow meters only because of the emphasis placed on these devices in various asthma education programs, self-help manuals, and asthma publications.
He comments that many of the improvements attributed to peak flow meters are due to more frequent follow-up visits and extensive educational and medical programs.
I agree with Dr. Twarog, who feels that the peak flow meter should be part of an overall plan of asthma education but that simply providing a peak flow meter as a means of measuring airway obstruction may not achieve the desired effect.
He wisely states that the utilization of peak flow meters will ultimately depend on patient compliance. Retrospective studies on diabetics asked to measure their blood sugar at home have shown a high rate of noncompliance even among well-educated diabetic patients and their families.
Similar problems with compliance can be anticipated with the peak flow meter. I estimate that nearly half of the patients I see during an asthma relapse have not used a peak flow meter prior to coming to the emergency room or our office.
Typical excuses offered as to why the peak flow meter was not used include, “I forgot” and “I left it in the closet.”Our practice prescribes peak flow meters to every patient with ongoing moderate to severe asthma who requires daily asthma medication. We do not “zone” all of our patients into green, yellow, and red zones.
This more confined approach is reserved for patients with more moderate to severe unstable asthma. We also utilize peak flow meters to determine the presence or absence of occupational and exercise-induced asthma.
The peak flow meter certainly allows the on-call doctor to make a more objective analysis of asthma relapses by phone during the evening or on weekends.
I also agree with Dr. Cockroft in that I do not think peak flow meters should be routinely utilized in patients with mild asthma, as such use could potentially cause social difficulties or emotional dysfunctions similar to those seen when patients with hypertension monitor their own blood pressure on a daily basis.
The peak flow meter serves as an important tool that allows the healthcare provider (or the patient) to assess the level of severity of asthma objectively and follow a predesigned treatment plan.
In summary, the peak flow meter is a vital component of the management of moderate to severe asthma that should be used in combination with intensive self-management and education programs focusing on using medications appropriately, recognizing the early warning signs of relapsing asthma, and implementing appropriate environmental controls.
Goals Of Asthma Therapy
The overall goals of asthma therapy are outlined. The ultimate objectives of asthma therapy are symptom control, near-normal lung function, few (if any) asthma relapses, and minimal school and work loss.
Additional objectives include normal or near-normal sleep patterns, normal exercise tolerance, and few (if any) emergency-room visits, all while avoiding the adverse effects of asthma medicines.
The NHLBI guidelines carefully describe a “step care” approach to asthma therapy. In step care treatment, the number of medications and dosing frequency is increased according to the severity and duration of a person’s asthma.
Differentiation is made between round-the-clock or daily preventative medicines and as-needed or “rescue” medicines. Within this context, we will now review the drug therapy in the major categories of asthma, namely
- Mild episodic asthma,
- Chronic moderate asthma,
- Chronic severe asthma, and
- Acute relapsing asthma. Please refer to the accompanying figures, which summarize each treatment plan.
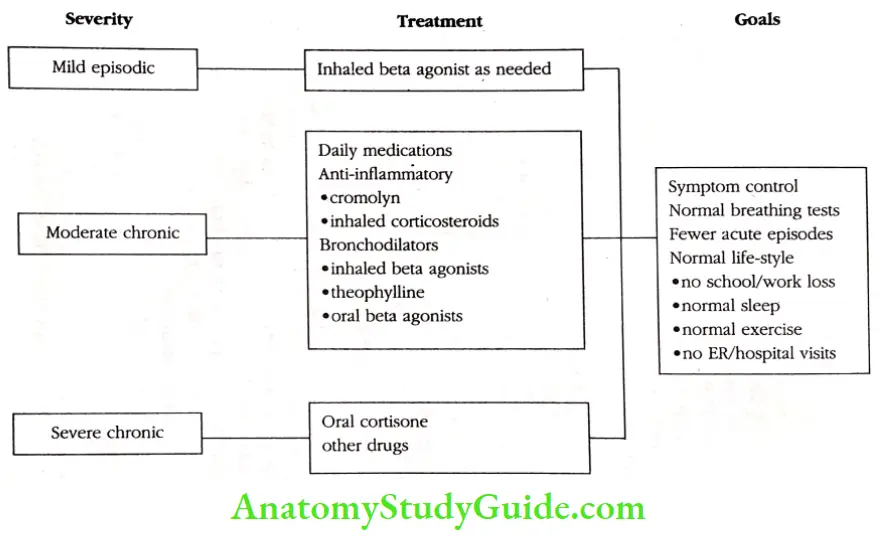
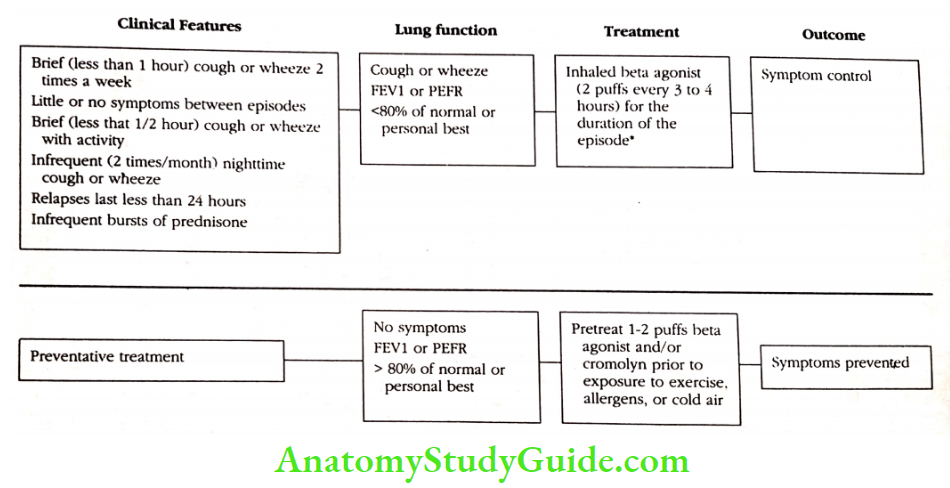
Mild Episodic Asthma
Mild asthma is typified by brief (usually less than one hour) episodes of coughing and wheezing occurring no more than two times a week. Patients with mild asthma are relatively symptom-free between relapses. They have good exercise tolerance, although some do wheeze with exercise, especially in colder air.
They have nocturnal asthma no more than one or two times per month and good school or work attendance. Pulmonary function tests and peak flow rates are usually 80 percent or better than predicted except during an acute attack.
Mild asthma responds quite well to the simple use of aerosolized bronchodilators such as a beta-agonist drug delivered by a metered dose inhaler. Children under age five may require nebulized, oral, or dry powdered beta-agonist drugs. Patients with mild episodic asthma rarely need to use prednisone as a rescue medicine.
Most asthma relapses last twelve to twenty-four hours, and regular drug therapy is not required except for short periods of time during allergen exposure or during a respiratory infection.
Many patients with mild episodic asthma benefit from pretreatment with Cromolyn or a beta-agonist prior to exposure to allergens, exercise, or cold air.
Chronic Moderate Asthma
Patients with chronic moderate asthma cough, wheeze, or shortness of breath more than one or two times per week. Symptoms frequently interfere with sleep and activity levels. Constant wheezing is noted during or after exercise, particularly during colder, damper weather. Asthma relapses can last several days.
These patients frequently miss school or work. Acute asthma leads to an occasional office or emergency room visit (usually less than three per year) Lung functions and peak flow rates range from 60 to 80 percent of normal or personal best, and peak flow rates can drop 20 to 30 percent during acute exacerbations.
All patients with moderate asthma have underlying inflammation of their bronchial tubes that does not go away when the bronchodilator drugs alone are used. The most important innovation in asthma therapy in the last five years is that it has been shown that anti-inflammatory agents.
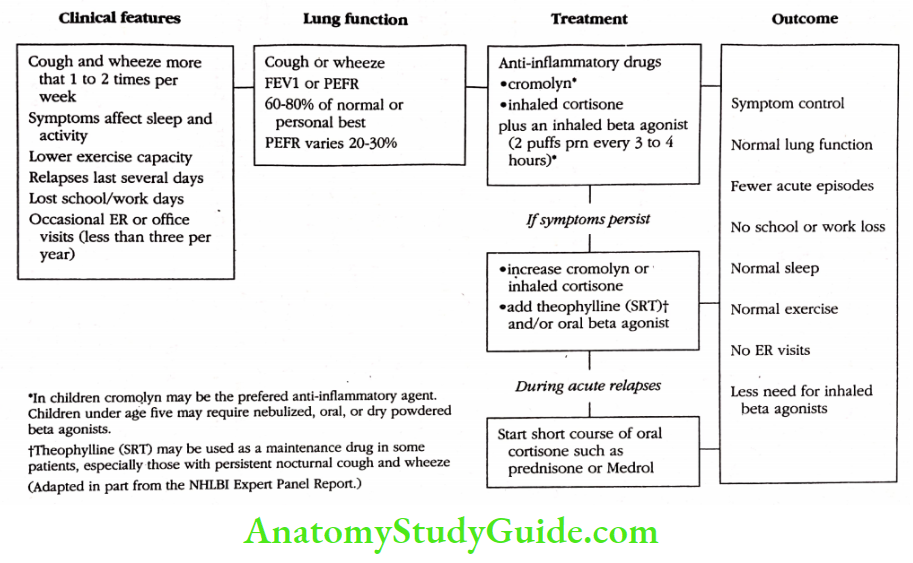
Cromolyn and corticosteroids are the first-line drugs of choice in the treatment of chronic moderate asthma. Cromolyn sodium (Intal or Fintal) has shown effectiveness in patients with moderate asthma, particularly in children and young adults in whom allergens play a major role.
Cromolyn is virtually void of any side effects and in essence, is one of the safest drugs in medicine. The most effective drugs for many patients with chronic moderate asthma are inhaled corticosteroids.
The three preparations available in the United States, beclomethasone (Vanceril or Beclo- vent), flunisolide (AeroBid), and triamcinolone (Azmacort), have been widely studied in various dosing schedules, and by and large they have been proven to be effective and safe with long-term use.
More potent preparations available in other developed countries may soon be introduced to the United States. Beta agonist drugs are also used in chronic moderate asthma. Some patients require these bronchodilator drugs on a regular basis before they inhale their anti-inflammatory agents.
Other patients utilize beta-agonists on an as-needed basis. When symptoms persist despite the use of an anti-inflammatory drug and an inhaled beta agonist drug, an oral beta agonist preparation or a long-acting theophylline medication can be added.
Theophylline is often recommended for patients with persistent nocturnal cough and wheeze. A short course of prednisone is indicated in patients with moderate asthma when relapses triggered by allergen exposure or respiratory infection are not controlled with their usual daily program.
Prednisone is given when peak flow rates remain below 50 percent of personal best. A few patients with moderate asthma benefit from utilizing both Cromolyn and inhaled cortisone.
Cromolyn is a preferred anti-inflammatory agent in young children, and children under age five who use beta-agonists may require nebulized, oral, or dry powdered beta-agonists.
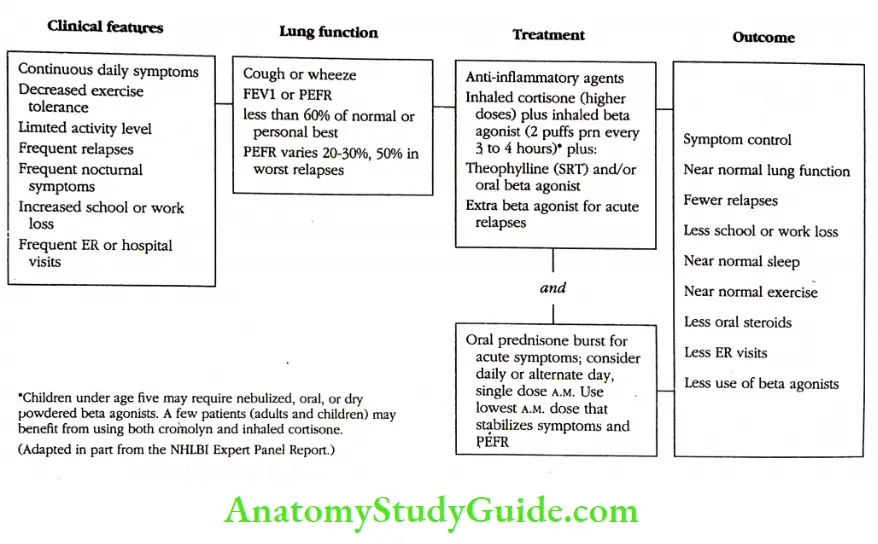
Chronic Severe Asthma
Unfortunately, 10 to 20 percent of patients have chronic severe asthma. The clinical features of chronic severe asthma are characterized by daily coughing and wheezing, decreased exercise tolerance, and lowered activity levels.
These patients suffer frequent asthma relapses and usually require more than two or three emergency room visits and or hospitalizations a year. They have frequent nocturnal wheezing and coughing, and their peak flow rates often show a typical morning dipping pattern.
Pulmonary functions are persistently abnormal, often less than 50 percent of predicted, and peak flow rates vary 20 to 50 percent during significant asthma relapses.
The obvious treatment for chronic severe asthma is inhaled anti-inflammatory agents, and inhaled corticosteroids are the drug of choice in this group.
Unfortunately, children under age five may not be able to utilize inhaled cortisone, although the new spacer devices with face masks make it easier to administer inhaled corticosteroids to this age group.
Most patients in this severe category are not controlled by an anti-inflammatory agent alone. Some benefit from using higher doses of inhaled cortisone in doses of up to twenty to twenty-four puffs per day of beclomethasone or its equivalent.
Patients with severe asthma always require beta-agonist drugs, either on a regular basis or as needed. Oral beta agonists and theophylline should be considered as maintenance drugs in patients with severe asthma.
Patients with severe asthma often require frequent rescue pulses of prednisone to prevent hospitalizations or life-threatening asthma. When patients with severe asthma relapse every time pred- nisone is tapered or discontinued, they should be considered candidates for alternate-day prednisone.
The alternate-day dose should be the lowest single early morning dose that stabilizes asthma. Patients with severe asthma, especially those who have experienced a life-threatening or near-fatal asthma episode, should have a well-defined crisis plan that makes it easy for them to make a decision about when to start prednisone.
They should be advised that overreliance on their beta agonist inhaler may result in a significant delay in seeking care, which may trigger a life-threatening asthma episode.
Acute Relapsing Asthma
We will now focus on the principles of management of acute asthma in the home, physician’s office, emergency room, or hospital setting. Obviously, the best treatment for acute asthma is to avoid common allergens or asthma triggers by practicing appropriate environmental controls.
The next best way to abort an acute episode is to learn to recognize the early warning signs. Not everyone who experiences an asthma relapse need to call their doctor, but patients who are at risk for life-threatening asthma. should be advised to seek out medical attention and follow a crisis plan tailored to their individual needs.
High-risk patients include those with a prior history of near-fatal asthma or respiratory failure requiring intubation, recent hospitalization, repeated emergency room visits, chronic use of prednisone, withdrawal from prednisone, a past history of fainting or seizures, or serious psychosocial problems.
Patients who fit the above description should immediately proceed to the hospital setting for management of acute asthma during an attack, while those with less serious asthma can often rely on home care.
There is a growing tendency to administer acute care in a physician’s office or clinic setting when available, as the patient’s primary physician or asthma specialist is more likely to be familiar with the patient’s needs and past history of asthma medications.
So informed, the doctor is more likely to design an asthma program to prevent additional asthma relapses.
The Acute Episode
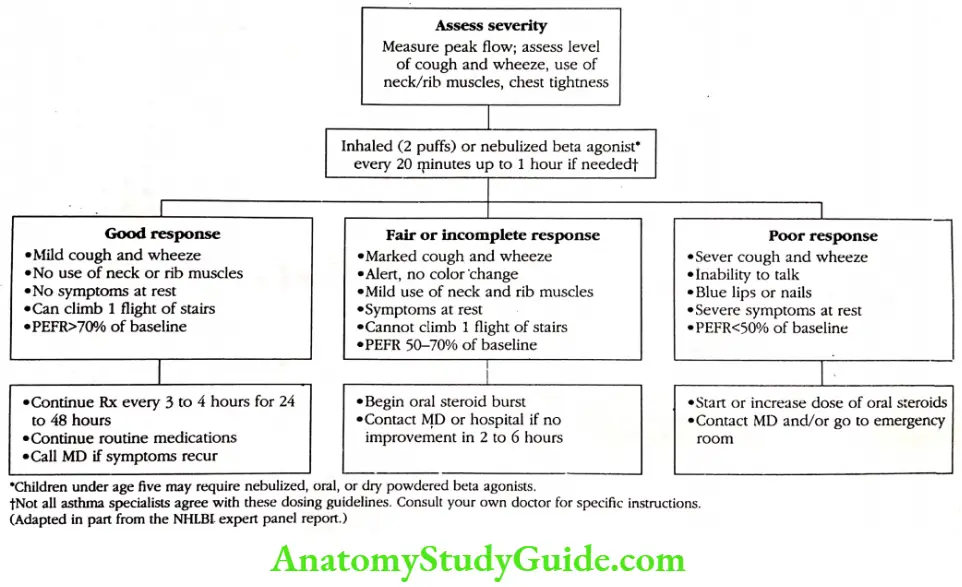
When evaluating an acute asthma relapse at home or in the physician’s office, it is important immediately to assess the severity of the acute asthma attack.
Obvious physical signs to evaluate during an acute attack include the severity of cough and wheezing, use of accessory muscles (neck and rib muscles) to breathe, chest tightness, inability to talk and or exercise, and discoloration of lips and fingernails.
The quickest way to test severity objectively is to measure the peak flow rate and compare it to the patient’s normal or personal best. The fundamental treatment of acute asthma attacks is the administration of a nebulized or an inhaled dose of a beta-agonist drug.
Current NHLBI recommendations state that these inhalations (two puffs) can be given every twenty minutes for up to one hour if needed. In children, only two doses are recommended. Not all asthma specialists agree with this NHLBI recommendation.
I suggest that you follow instructions from your own doctor on the dosing frequency and interval of inhaled beta-agonists. Several home management techniques have been shown to be relatively ineffective in managing acute asthma.
Including drinking large volumes of liquid, breathing moist air or mist from a hot shower or nebulizer, breathing into a bag, or taking over-the-counter antihistamines or cold remedies.
There are three possible responses to initial treatment with an inhaled beta agonist: good, fair, and incomplete, and poor. A good response is typified by mild coughing and wheezing, no use of neck or rib muscles, no symptoms at rest, and the ability to climb one flight of stairs.
Peak flow rates are usually 70 percent or better than the baseline. Treatment should be continued for twenty- four to forty-eight hours along with routine asthma medicines, and health-care providers should be contacted if symptoms recur.
A fair or incomplete response after one hour of treatment is characterized by marked coughing and wheezing, patient alertness with no color changes (cyanosis), and minimal use of neck and rib muscles. This patient may have some symptoms at rest and cannot exercise vigorously.
Peak flow rates are usually 60 to 70 percent of personal best or baseline. Many physicians advise their patients to start a pulse of oral steroids at this point.
As we feel that the decision regarding the need for prednisone is best made by the patient’s doctor, our practice advises patients to contact their primary care provider, our office, or the hospital when there is no improvement within two to six hours.
A poor response to inhaled beta-agonists means just that. Severe coughing and wheezing persist, patients need to use their accessory muscles to breathe, they often cannot speak without gasping, and they have blue discoloration (cyanosis) of their lips and nails.
Peak flow rates are usually less than 50 percent of the baseline. These are the people who die from asthma when they delay seeking care. Immediate contact with their healthcare provider or local emergency room is essential for patients with this type of asthma relapse.
If these patients cannot contact their provider or get to an emergency room within minutes, they should start oral prednisone on their own.
Before concluding this discussion on the use of asthma medications in various types of asthma, I would like to point out that drug management is only one component of any successful asthma education program.
Strict environmental precautions are essential, and immunotherapy or allergic injections will benefit many patients with IgE-mediated asthma. Such global treatment of asthma should be based on the understanding of the underlying basic mechanisms.
The patients should develop a sense of when to anticipate asthma relapses and start appropriate therapy. Patient and family education is the cornerstone of all asthma treatment programs.
Asthma Crisis Plan
Our practice has devised a crisis plan for the high-risk asthma patient. This plan is given to the patient, family, primary physicians, clinic and school nurses, local emergency rooms, and any allied health personnel who may be involved in the care of the patient.
The purpose of this plan, reproduced, is to make everyone involved with the patient aware of the severity of the patient’s asthma and convey the need for immediate and appropriate care when such a patient suffers a significant asthma relapse. A copy of this plan can be given to the patient or family.
While it is not necessary for the patient to carry this plan at all times, it should be used when the patient is traveling or visiting medical facilities unfamiliar with the severity of the patient’s asthma.
This plan can be sent to the patient’s primary physician, school or work location, summer camp, and local clinic or hospital.
Reports of increasing hospitalizations and deaths in patients with asthma of all ages have led to the identification of high-risk factors that are predictive of life-threatening asthma attacks.
Patients with asthma in this high-risk group have been shown to have many of the following characteristics:
- Severe asthma of any type
- A past history of seizures
- Asthma that is unresponsive to the usual bronchodilators, cromolyn, and cortisone inhalers
- Sudden attacks of life-threatening asthma
- Past history of respiratory failure that required assisted ventilation
- Severe nighttime (nocturnal) wheezing
- Wide fluctuations in pulmonary function tests
- Poor compliance by the patient and/or family.
- The high degree of allergy and severe attacks after exposure to indoor or outdoor allergens
- Significant emotional problems: depression, anger, acting out, or family disruption
- Using asthma to manipulate, and poor self-care.
Most asthma mortality studies have found that the main cause of asthma morbidity and mortality is a tragic delay by the patient or family to seek immediate care during an ongoing asthma crisis.
This patient or family is advised to immediately contact their primary physician or asthma specialist or to go to the emergency room when the following symptoms occur:
- Extreme breathlessness, inability to speak, blue discoloration (cyanosis) of the lips or fingers, severe neck or chest pain
- Asthma that is unresponsive to adrenaline-like inhalers, theophylline, cromolyn, or the cortisone inhalers
- The need for more extra doses of an adrenaline-like inhaler or extra inhalation treatments every two to three hours
- A persistent decrease in peak flow readings
Studies have shown that the two most important factors in asthma relapses that lead to an asthma death are complacency on the part of the patient, family, and even physicians when the above events occur combined with a failure to use a cortisone drug such as prednisone in the early stages of an asthma relapse.
If physician contact is impossible or transport is difficult, the patient should take a dose of oral prednisone (30 to 60 milligrams) and then seek immediate medical care. Patients or parents should keep this plan and a list of current asthma medications available at all times (especially when traveling).
They should carry a Medic Alert card or bracelet as well as an Ana-Kit or EpiPen. Whenever possible, these patients should be taken to a hospital familiar with the severity of their asthma and capable of delivering intensive respiratory care.
Severe asthma relapses and asthma deaths can be prevented by following a comprehensive asthma crisis plan. Emergency room physicians who are unfamiliar with the patient’s asthma should contact the primary physician or asthma specialist when these patients are seen in the emergency room.
Most, if not all, of these relapsing high-risk asthma patients will require a cortisone drug such as prednisone before they are discharged from the emergency room.
Nocturnal Asthma
Nighttime or early morning asthma, commonly called nocturnal asthma, was first recognized in 1698 by Sir John Floyer, who stated in his “Treatise on Asthma,” “I have often observed the Fit always to happen after Sleep in the Night when Nerves are filled with windy Spirits and Heat of the Bed has rarefied the spirits and Humours.”
Thomas Willis, another famous English physician, felt that nocturnal asthma was due to overheating of the blood by one’s bedclothes. Numerous surveys have shown that 90 percent of asthmatics wake up coughing or wheezing sometime during the night, more commonly between 3:00 and 5:00 A.M.
Many patients are unable to return to sleep without specific asthma treatment. The major consequence of nocturnal asthma is loss of sleep, resulting in deterioration of one’s daytime performance at school or work. In families with a child with asthma, sleeplessness affects all members of the household.
Nocturnal asthma attacks are more dangerous than daytime episodes, as asthma death studies have shown that a majority of asthma deaths occur unexpectedly between midnight and 8:00 A.M.
Plausible explanations for nighttime asthma include a fall in circulating cortisone and epinephrine levels, gastric reflux regurgitating food or acid from the stomach), high allergen exposure (animal dander and dust mites), and small changes in the tone of the nervous system’s control of the airway.
Recent studies show that airway inflammation is more severe in persons in the prone position than in persons in the upright position, suggesting that recumbency or lying down is one cause of nocturnal asthma.
Some or all of these factors produce an increase in the hyperresponsiveness of the airway, which causes a cough or wheezing severe enough to awaken a sleeping patient. Dr. Margaret Turner- Warwick of Brompton Hospital in London, England, collected data on 7,729 asthma patients who reported nocturnal wheezing.
Sixty- four percent wheezed three out of seven nights, and more than one-third wheezed every night. The surprising finding of her study was that nearly 25 percent of subjects considered their asthma to be mildly wheezed every night, and nearly 50 percent were awakened three times a week.
Dr. Turner-Warwick concluded that being awakened at night by asthma symptoms was very common, despite the fact that patients often overlooked these nocturnal episodes. Healthcare providers should be aware that peak expiratory flow meters can record the severity of night-time asthma and response to treatment.
Those patients who are morning diapers are more susceptible to nocturnal asthma. Additional studies of nocturnal asthma find that wheezing in the latter third of the night (from 3:00 to 5:00 A.M.) is often more severe than asthma that occurs in the evening or early morning (from 10:00 PM. to 3:00 A.M.).
Patients who are subject to respiratory arrest are those with large swings in peak flow rates over a twenty-four-hour period, and the majority stop breathing between midnight and 6:00 A.M.
What is the best drug for the control of nocturnal asthma? Most authorities feel that nocturnal asthma is a typical late-phase asthma response, and thus it makes sense to use an anti-inflam- matory drugs such as cromolyn or cortisone in all patients with nocturnal asthma.
When these late-phase drugs fail to control nocturnal asthma, a slow-release theophylline drug may work quite nicely. Some patients stop wheezing in the middle of the night when they take a longer-acting oral beta agonist.
The inhaled beta agonist drugs currently available in the United States have not been shown to be very effective in preventing nocturnal asthma, as their duration of action is less than four hours, yet inhaled beta-agonists are the best drugs for relieving a nighttime attack.
One of the problems with the treatment of nocturnal asthma is that most bronchodilators (except theophylline) do not provide full twelve-hour protection. This supports the concept that improving the duration of action of inhaled beta-agonist drugs may be a major advance for the alleviation of nocturnal asthma.
Gastroesophageal Reflux
The opening of the esophagus (food pipe), which leads to the stomach, is guarded by a small muscle, or sphincter. When this sphincter relaxes (opens up), small amounts of food or gastric acid are regurgitated up into the esophagus and can be aspirated into the lungs or bronchial tubes.
This is called gastroesophageal reflux (GER). There is a growing body of evidence that GER may play an important role in many cases of asthma. Interest in the inter-relationship between asthma and GER waxes and wanes.
Evidence has been gathered that shows that nearly three of four asthmatic patients have heartburn or reflex independent of their use of bronchodilators. Several studies have reported significant improvement with postural GER therapy (using two or three pillows), antacids, and anti-gastritis-ulcer preparations.
In addition, recent surgical studies have suggested that surgical correction of GER results in dramatic improvement of asthma. Unfortunately, there is no real diagnostic method available that confirms the presence of GER-induced asthma.
The University of Washington researchers studied ninety patients with laboratory evidence of gastroesophageal reflux. These patients were randomly assigned to receive the antiulcer drug cimetidine, to receive a placebo drug, or to undergo surgery for reflux.
At six months, all groups improved somewhat, particularly those who received cimetidine or underwent surgery. There was no significant change in pulmonary function studies, and when cimetidine was discontinued, many asthma patients relapsed.
Over a long-term follow-up (average of seventy-seven months), the surgically treated group improved the most. Many of these patients were followed for more than five years, and this study.
Strongly implied that GER plays a significant role in asthma and that doctors should no longer ignore the coexistence of wheezing and indigestion. I am now using more antacid and ulcer medications in my patients with asthma who complain of chronic heartburn or indigestion.
Obviously, there is a need for additional studies to sort out the role GER plays in asthma.
When To Taper Asthma Medicines
The NHLBI guidelines precisely outline the need for asthma medicines when the patient is coughing and wheezing. One of the more difficult tasks in treating asthma is deciding when and how to adjust or taper the asthma medication program when the patient is relatively asymptomatic.
The decision is more difficult for patients with moderate asthma, whose needs can vary from day to day, week to week, season to season, and year to year. At certain times of the year, particularly during the change of seasons, patients may require medication on a daily basis.
Whereas at other times of the year (midsummer and midwinter), they may revert to an as-needed schedule. My approach to patients with moderate asthma who have varying needs for medications is as follows: if they are taking their asthma medications on a regular basis, say, three times a day.
I tell them to taper twice a day once they have been symptom-free or have had normal peak flow readings for three to four weeks.
If they are symptom-free for another month, they can go to once-a-day dosing, and if they continue to be symptom-free, they may be able to stop their medications completely and revert to an as-needed schedule.
If asthma recurs or peak flow readings fall while patients are tapering medicines, patients are instructed to revert to the previous dose schedule that controlled their symptoms or returned their peak flow reading to normal.
When they get a chest cold or a respiratory infection, they are told to resume their full program of medications. In essence, I try to instruct the patients to be their own asthma doctors.
Patients are taught to contact their primary physician or our office in the early stages of an asthma relapse that may require antibiotics or prednisone. Not every patient or family can be handled in this manner, as self-management requires a certain level of patient motivation, judgment, and intelligence.
No one should attempt to follow these directions without the advice and consent of a personal physician or asthma doctor.
The Noncompliance Problem
Medical jargon for failing to follow a list of instructions is called “noncompliance.” Fifty to 90 percent of all patients who are given a simple ten-day course of oral penicillin for strep throat do not complete it.
The required course of therapy! Similarly, one-half to two-thirds of all asthmatics do not take their medicines as prescribed by their primary physician or asthma doctor.
Non- compliance is a very common problem in adolescents with asthma, as peer pressures and the need not to be different or sickly lead to a total disregard for asthma medications. Inhaler overuse is the biggest threat in this age group.
Sometimes poorly informed school personnel actively contribute to noncompliance when they make it difficult for the student to take asthma medications at school or prior to gym classes or sports activities.
A failing memory and a confusing medication schedule are common causes of non-compliance in elderly patients.
How can compliance be improved? I use the following instructions to improve compliance:
- Ask your doctor for a written list of medications and their doses at each visit.
- Learn the names of your asthma medicines! Avoid using terms such as “the. yellow inhaler and the pink pill.”
- Keep a diary of symptoms and use of medications.
- If you are elderly, keep accurate pill counts. Use a pillbox and arrange for a relative or visiting nurse to look in on you if you live alone.
- Monitor refills of your pocket inhalers, especially if you are a young adult.
- Review your instructions on proper inhaler usage.
- Obtain educational material on asthma and enroll in self-help asthma programs.
Goals In Exercise Induced Asthma
Knowledgeable asthmatics who have a good understanding of their condition know there is no reason to avoid healthy exercise. Using medications correctly is the best way to avoid asthma while exercising. Remember, many Olympic champions and professional athletes have exercise-induced asthma.
Exercise-induced asthma will be minimized or completely averted by adhering to the following guidelines:
- Take one or two puffs of your puffer or beta agonist inhaler fifteen minutes prior to exercise.
- If this is not successful, take an additional two puffs of the Intal inhaler fifteen to thirty minutes after using your beta agonist inhaler.
- Warm up before engaging in vigorous activities.
- Cover your mouth and nose with a mask or scarf when exercising outdoors in colder weather.
- Avoid strenuous exercise when you have a cold or an up- per respiratory infection.
- Follow workouts with a ten-minute cooling-down period by walking or doing stretching exercises.
- If exercises constantly provoke asthma, consider activities such as swimming and yoga.
Asthma Education Programme
Research led to the development of many new spectacular asthma drugs in the 1970s. The 1980s witnessed the growth of successful patient education or self-help asthma programs.
Some health professionals now prefer the term cooperative care over self-help to avoid the implication that self-care or self-help permits patients to manage asthma by themselves.
The overall purpose of patient education is to involve the patient, family, doctor, school nurse, educators, and allied health personnel fully in a total asthma-care program.
These educational programs foster a better understanding of asthma and reduce the negative impact this disease can have on patients and their families. Such programs also reduce asthma morbidity and mortality.
Their mission is to teach patients and their families to recognize asthma symptoms, reduce exposure to asthma triggers, and properly use asthma medications.
These programs stress the need to allow patients with asthma and their families to learn how to handle asthma in a responsible manner. Some of the more successful asthma programs are described in the following sections.
Leave a Reply