Bone, Joints, and Soft Tissue Tumors
Question 1. Write a note on Paget’s disease of bone.
Answer:
Paget disease
- Also called osteitis deformans
- Disorder of increased bone mass
- A new bone deposition is disordered
- Mutations in the SQSTM1 gene are seen in Paget disease
- The average age at diagnosis is 70 years
Read and Learn More Preparatory Manual of Pathology Question and Answers
3 phases
- Osteolytic stage
- Mixed osteoclastic osteoblastic stage, followed by a predominant osteoblastic phase
- Osteosclerotic stage
Morphology
- Microscopic hallmark is a mosaic pattern of lamellar bone, seen in the sclerotic stage
Question 2. Write a note on fracture healing.
Answer:
Steps involved in fracture healing
- At the site of fracture, there occurs hematoma formation, due to rupture of blood vessels
- Due to the release of PDGF, TGF-α, and FGF from inflammatory cells, there is the deposition of uncalcified tissue, called pro call us or soft tissue callus
- After 2 weeks, soft tissue callus changes into bony callus
- First woven bone is produced in the bony callus, which in two to three weeks’ time is replaced by lamellar bone
Complications: Non-union, malunion at the fracture site, or pseudoarthrosis
Question 3. Write a note on pyogenic osteomyelitis.
Answer:
Pyogenic osteomyelitis
- Organisms may reach the bone by
- Hematogenous spread
- Extension from a contiguous site
- Direct implantation
Etiology
- Staphylococcus aureus is the most commonly responsible agent
- Escherichia coli, Pseudomonas, and Klebsiella are isolated from individuals with genitourinary tract infections or from intravenous drug abusers
- Haemophilus influenza and group B streptococci are most common in neonates
- Sickle cell disease patients are predisposed to Salmonella infection
Morphology
- In the acute phase, bacteria proliferate and induce a neutrophilic inflammatory reaction
- Necrosis of bone cells and marrow occurs within the first 48 hours
- Dead bone is called a sequestrum
- A draining sinus can develop between the infected bone and the skin
- The new bone deposition is seen as time progresses, which is called involucrum
Question 4. Write a note on cartilage-forming bone tumors.
Answer:
Cartilage-forming tumors
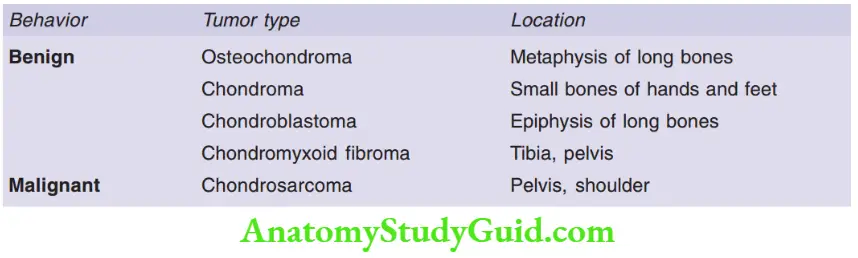
Question 5. Write a note on osteochondroma in relation to its gross and microscopy.
Answer:
Osteochondroma (exostosis)
- Most common benign bone tumor
- Mostly solitary
- Can be a part of multiple hereditary exostosis syndrome
- Site: Arises from the metaphysis near the knee joint
- Age group: 10–30 years
Morphology
Gross
- Osteochondromas are sessile or pedunculated lesions, ranging in size from 1 to 20 cm
Microscopy
- The cartilage cap is composed of benign hyaline cartilage and has the appearance of a disorganized growth plate
- Osteochondromas usually stop growing at the time of closure of the growth plate
Question 6. Discuss osteogenic sarcoma about its etiology, and radiological, clinical, and morphological features.
Answer:
Etiopathogenesis of osteogenic sarcoma
- Malignant tumor in which the cancerous cells produce osteoid matrix or mineralized bone
- Bimodal age distribution: 75% of patients are younger than 20 years of age, and the second peak occurs in older adults
- Predisposing factors: Paget disease, bone infarcts, and prior radiation
- The following mutations are noted in osteosarcoma: RB gene mutation, TP53 gene mutation, INK4a inactivation
Clinical features
- Site: Metaphyseal region of long bones, most commonly around the knee joint
- Clinical features: Painful, progressively enlarging mass or pathological fracture
Radiographic features of osteosarcoma
- Shows large destructive, mixed lytic and blastic mass with infiltrative margins
- Tumor breaks through the cortex and lifts the periosteum
- Codman triangle triangular shadow between the cortex and raised ends of periosteum seen radiographically
Morphology
- Most common subtype: Arises from the metaphysis and is a primary, intramedullary, osteoblastic, and high grade
Gross
- Tan-white tumor in the metaphysis and proximal diaphysis
- Tumor infiltrates the cortex, lifts the periosteum, and forms soft tissue masses on both sides of the bone
Microscopy
- Tumor cells vary in size and shape and have large hyperchromatic nuclei
- Bizarre tumor giant cells are common
- Formation of a fine, lacelike pattern of neoplastic bone produced by the tumor cells is diagnostic
- Abnormal mitotic figures are also seen
Question 7. Write a note on Ewing’s sarcoma.
Answer:
Ewing sarcoma
The second most common sarcomas after osteosarcomas in children
Age group
- Younger than 20 years, males are more commonly affected
- Site: Diaphysis of long bones especially femur and flat bones of pelvis
- Clinical features: Painful enlarging mass, fever, elevated erythrocyte sedimentation rate (ESR), anemia, and leukocytosis
- X-ray: It shows a destructive lytic tumor with a characteristic periosteal reaction in which the layers of the reactive bone are deposited in an onion-skin fashion
- Pathogenesis: t(11;22) Translocation resulting in the fusion of the EWS gene on chromosome 22 to the FLI1 gene
Morphology
- Composed of sheets of uniform small, round cells
- Tumor cells have scant clear cytoplasm (clear as it is rich in glycogen)
- Geographic necrosis may be a prominent
Question 8. Write a note on osteoclastoma (giant cell tumor).
Answer:
Giant cell tumor
- Due to the presence of multinucleated osteoclast-type giant cells, they are also called osteoclastoma
- More common in females, age group: 20–40 years
Pathogenesis
- Neoplastic cells of giant cell tumors are primitive osteoblast precursors
- A tumor is comprised mainly of non-neoplastic osteoclasts
- Neoplastic cells express high levels of RANKL, resulting in osteoclastic proliferation and hence resulting in destructive resorption of bone matrix
Site
- Arises in the epiphysis, most commonly around the knee joint (distal femur and proximal tibia)
- Solitary, can be multicentric (in distal extremities)
X-ray
- The lytic, expansile lesion in the epiphysis
Microscopy
- The tumor comprises sheets of uniform oval mononuclear cells (neoplastic) and numerous osteoclast-type giant cells
- The nuclei of the mononuclear cells and the osteoclasts are ovoid with prominent nucleoli
Question 9. Enumerate the differential diagnosis of giant cell tumor of bone.
Answer:
Differential diagnosis of giant cell tumor of bone
- Chondroblastoma, metaphyseal fibrous defect, non-ossifying fibroma, chondromyxoid fibroma, Langerhans cell histiocytosis, solitary bone cyst, osteitis fibrosis cystic, aneurysmal bone cyst, giant cell reparative granuloma, osteoid osteoma, osteoblastoma
Question 10. What is a pannus?
Answer:
Pannus
- In rheumatoid arthritis, destroyed joints are replaced by a mass (pannus) comprising edematous synovial tissue, inflammatory cells, granulation tissue, and fibroblasts that grow over the articular cartilage
- Pannus bridges the opposing bones, to form fibrous ankylosis, which over time ossifies and results in the fusion of bones called bony ankylosis
Question 11. Write a note on gout.
Answer:
Gout
- Transient attacks of acute arthritis initiated by the deposition of monosodium urate crystals within and around joints
- Primary gout: Unknown cause
- Secondary gout: Uric acid is increased because of underlying disease (and disease predominates clinical picture)
Pathogenesis
- Hyperuricemia (plasma urate level above 6.8 mg/dl) is necessary, but not sufficient, for the development of gout
- Hyperuricemia results from either overproduction or the reduced excretion of uric acid
Morphology
1. Acute arthritis
- Dense neutrophilic infiltrate in the synovium
- Monosodium urate crystals are found in the cytoplasm of neutrophils, which appear as long, slender, needle-shaped, and negatively birefringent
2. Chronic tophaceous arthritis
- Repetitive precipitation of urate crystals during acute attacks
- Synovium becomes hyperplastic, fibrotic, thickened, and forms pannus
3. Tophi at various sites
- Tophi are pathognomonic hallmarks of gout
- Aggregates of urate crystals surrounded by reactive fibroblasts, inflammatory cells, and giant cells
- Sites: Articular cartilage, ligaments, tendons, bursae, earlobes, fingertips, skin
4. Gouty nephropathy
- Urate crystals deposition in renal medullary interstitium or tubules
- Uric acid nephrolithiasis and pyelonephritis
Question 12. Write a note on liposarcoma.
Answer:
Liposarcoma
- Age group: 50–60 years
- Sites: Proximal extremities and in the retroperitoneum
Three morphologic subtypes
1. Well-differentiated liposarcoma
- Shows mature adipocytes and scattered spindle cells with hyperchromatic nuclei
2. Myxoid liposarcoma
- Proliferating lip-oblasts in different stages of differentiation, prominent anastomosing capillary network, and mucoid matrix
3. Pleomorphic liposarcoma
- Sheets of anaplastic cells, bizarre nuclei, and immature adipocytes (lip-oblasts)
- Shows S-100, actin and desmin positivity
Question 13. Write a note on rhabdomyosarcoma.
Answer:
Rhabdomyosarcoma
- Malignant mesenchymal tumor with skeletal muscle differentiation
- Subtypes: Embryonal, alveolar, and pleomorphic
- Alveolar and embryonal rhabdomyosarcoma: Most common soft tissue sarcoma of childhood and adolescence
1. Embryonal rhabdomyosarcoma
- Common in the head and neck region
- Gross: Soft gray infiltrative mass
- Microscopy: Sheets of primitive round and spindle cells in a myxoid stroma. Rhabdomyoblasts with visible cross-striations may be present
2. Alveolar rhabdomyosarcoma
- 10–25 years of age group
- Most common in the extremities
- Tumor cells are small, round, or oval and are firmly attached to fibrous strands (resembling pulmonary alveoli)
- Tumor cells can detach themselves, resulting in an alveolar or pseudo-glandular appearance
3. Pleomorphic rhabdomyosarcoma
- Seen predominantly in adults
- Common in extremities especially thigh
- Characterized by numerous large, multinucleated, bizarre eosinophilic tumor cells
- Confirmed by myogenin positivity
Question 14. Write a note on schwannoma.
Answer:
Schwannomas
- Benign tumors that exhibit Schwann cell differentiation and often arise from peripheral nerves
- The most common site cerebellopontine angle
- Associated with inactivating mutations in the NF2 gene on chromosome 22
Morphology: Well-circumscribed, encapsulated masses that abut the associated nerve without invading it
Gross
- Tumors form firm, gray masses
Microscopy
- Antoni A areas (appear as densely eosinophilic)
- Antoni B areas (appear as loose pale)
- Verocay bodies (anuclear zones in between Antoni A areas)
Question 15. Write a note on neurofibroma.
Answer:
Neurofibromas
- Benign nerve sheath tumor
- Composed of neoplastic Schwann cells admixed with perineural-like cells, fibroblasts, mast cells, and spindle cells
Morphology
- Localized cutaneous neurofibroma: Un-encapsulated nodular lesions arise in the dermis and subcutaneous fat
- Diffuse neurofibroma: Tumor cells diffusely infiltrate the dermis and subcutaneous connective tissue, entrapping the fat and appendage structures
- Plexiform neurofibroma
- Tumors grow within and expand the nerve fascicles
- Bland spindle cells are admixed with wavy collagen bundles resembling carrot shavings
Leave a Reply