Clef Lip and Clef Palate Introduction
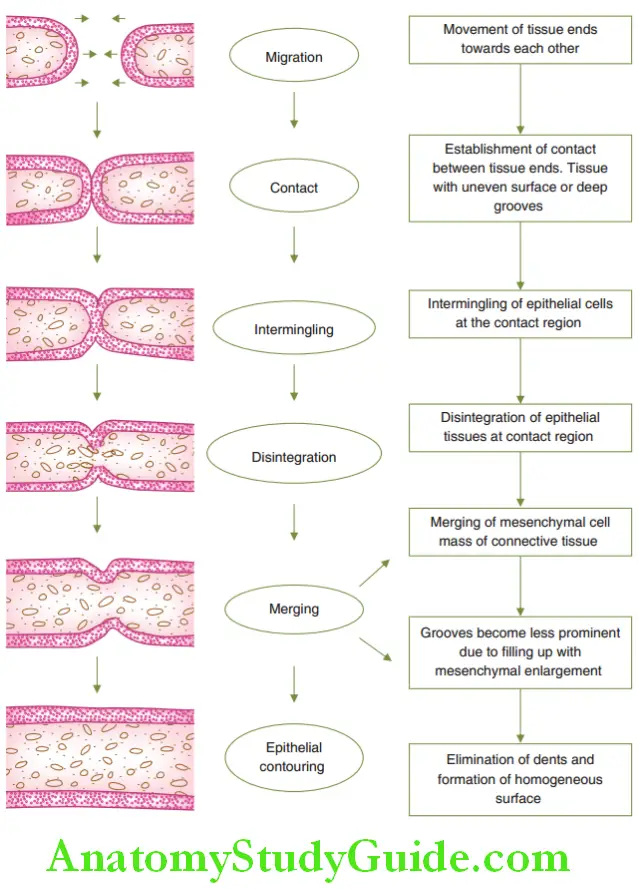
Fusion is a process of joining two or more things together to form a single entity. It can be described as merging when the joining or blending happens in gradual stages.
Table of Contents
Tissues of the body form by the process of fusion. The process of formation of tissues by fusion is depicted.
A clef is an opening or fissure or a ‘V-shaped indentation. In embryological terms, a clef is a fissure occurring during embryonic development.
Read And Learn More: Paediatric Dentistry Notes
The failure effusion of two ends of tissue to form a homogeneous structure creates a clef in that region.
The process is described as a prominence or projection on a structure. The face of the foetus develops by the fusion of four processes.
The failure of fusion of the four processes creates a cleft Various types of facial cleft occur depending upon the region, extent or time of failure of fusion of the four processes.
The extent of clefting varies from a mild notch to complete non-union of the processes.
Derivatives Of Facial Processes
The face of the foetus develops from four processes or ‘primordia’ during the fourth to seventh week of intrauterine life.
Structures of the face are formed by the fusion of these processes at a selective rate, pace and place as predetermined in nature.
The four primordia that form a face are as follows:
- Frontonasal process
- Right maxillary process
- Left maxillary process
- Mandibular process
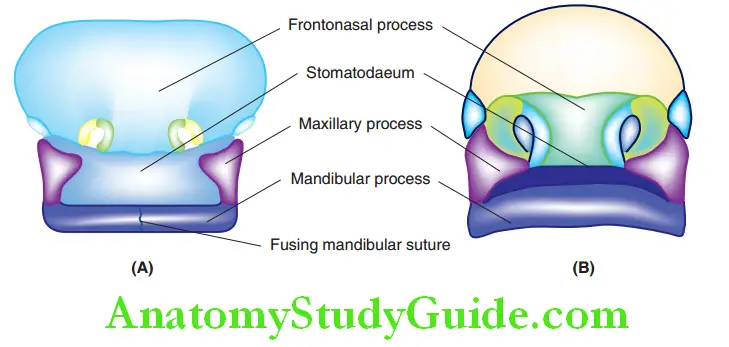
Stomatodaeum is a depression bounded by the frontonasal process cranially, maxillary processes on either side and the mandibular process caudally.
This is the future oral cavity. depicts the facial region of the foetus at around 4 and 6 weeks of intrauterine
Frontonasal Process:
This process develops mesenchymal proliferation to produce the median nasal process in the centre and two lateral nasal processes on the right and left sides.
The lateral aspect of the median nasal processes and the medial aspect of the lateral nasal processes form the external nares or nasal domes on either side.
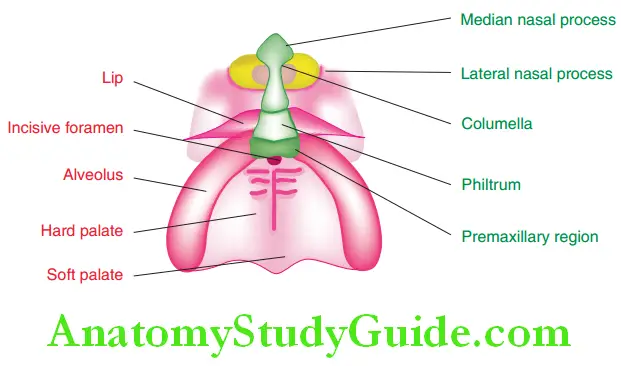
The median nasal processes of both sides unite to form the primary palate.
The primary palate accommodates the following structures:
- Philtrum or the median region of the upper lip.
- The anterior part of the alveolar process accommodating the four maxillary incisors
- Triangular premaxilla up to the incisive foramen
The columella of the nose and philtrum of the upper lip is also derived from the frontonasal process.
The skin overlying the philtrum is however derived from the maxillary process. The median palatine process is an extension of the frontonasal process towards the stomatodaeum.
The derivatives of the frontonasal process are labelled in green colour.
Right, And Left Maxillary Processes:
At the end of the sixth week of intrauterine life, each maxillary process gives rise to one lateral palatine process or lateral palatal shelf on its inner aspect.
Initially, the lateral palatine processes are oriented vertically as the tongue is present in between them.
When the tongue drops down along with the mandible, the two lateral shelves reorient in a horizontal plane.
The two lateral palatine shelves fuse in the midline and with the premaxilla to form the palate.
They fuse with the single median palatine process (derived from the frontonasal process) at the region of the incisive foramen.
The fusion proceeds distally from the incisive foramen to form a complete palate up to the posterior part.
Intramembranous ossification occurs in the anterior part of the palate forming the hard palate and the rest of the portion remains as the soft palate.
The derivatives of maxillary processes are labelled in pink colour.
Mandibular Process:
In the beginning, the mandibular process exists as right and left processes. They fuse with each other by the fourth week of intrauterine life to form a single mandibular process.
The mandibular process gives rise to the lower jaw or the mandible and the lower lip.
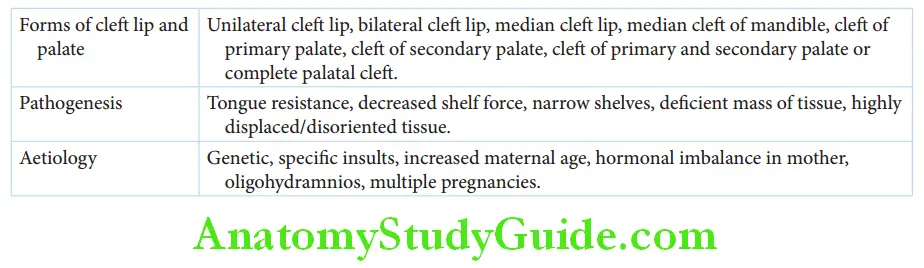
Pathogenesis:
The failure of fusion of the four facial processes during the development of the foetus can lead to the formation of various orofacial clefts.
This chapter describes cleft lip and cleft palate in detail as they are of most significance in endodontic practice.
The following reasons are proposed as causes of a cleft lip or cleft palate. None of these reasons could be proved beyond doubt.
1. Tongue resistance: The tongue has to drop down to enable palatal shelves on both sides to move towards each other. This downward movement of the tongue may be prevented. The tongue may lie in between the palatal shelves.
2. Decreased shelf force: The palatal shelves may lack the potential to move towards each other for fusion.
3. Narrow shelves: Narrow-sized palatal shelves may not fuse completely in spite of lack of any other hindrance.
4. Deficient mass of tissue: Lack of physical mass of tissue prevents fusion of palatal shelves.
5. Highly displaced/disoriented: tissue in space.
Aetiology:
Hereditary factors and gene mutation are the major factors that cause cleft lip and palate. Some specific insults during the first trimester of pregnancy can affect embryonic craniofacial development.
The following factors that can occur in a pregnant woman have been identified to cause cleft lip and cleft palate in her fetus:
- Exposure to teratogens
- Irradiation
- Viral infections such as rubella
- Physical or mental trauma
- Nutritional factors: Folate deficiency, hypervitaminosis A
- Increased maternal age
- Hormonal imbalance
- Oligohydramnios: Intrauterine growth retardation
- Multiple pregnancies
Teratogens are drugs or any other substances capable of interfering with the development of a fetus.
The following teratogens can cause cleft lip or cleft palate:
- Aspirin
- Cigarette smoking
- Dilantin
- Antimetabolites
- Ethyl alcohol
- Cytotoxic drugs
Clinical Presentation:
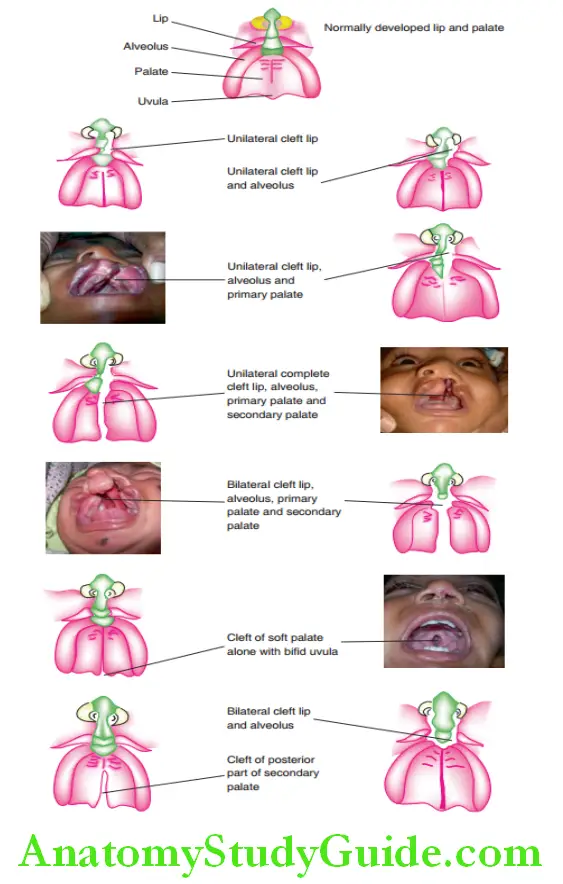
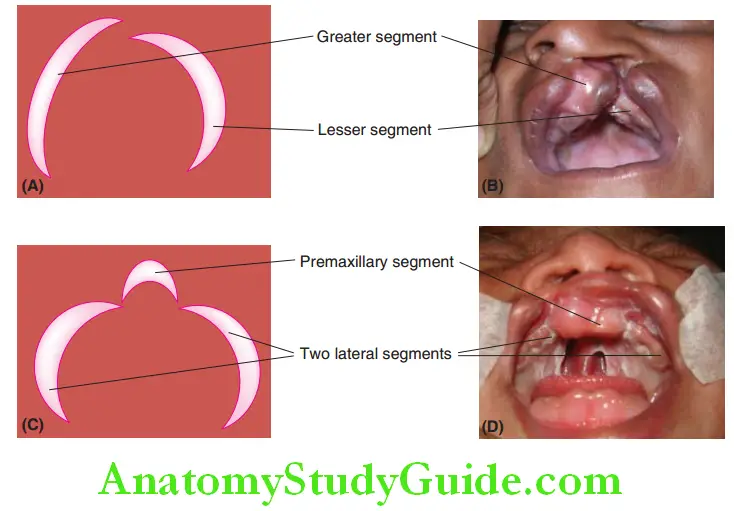
The clef may be a mild notch in the lip or extend as a complete bilateral clef of the lip, alveolus, primary palate, hard palate, and soft palate.
Clinical presentation of the clef depends on where the fusion of processes has failed. It may extend into the floor of the nose also.
The clef can be unilateral or bilateral and can occur in any combination.
A unilateral cleft lip occurs due to the failure of fusion of the median nasal process and maxillary process of one side.
A bilateral cleft lip occurs when the median nasal process and maxillary process do not unite on both sides.
A median cleft lip is a rare condition that occurs when median nasal processes of both sides fail to fuse partially or totally.
Median clef of the mandible is another rare occurrence. It occurs when mandibular processes of both sides fail to fuse in the fit week of intrauterine life.
Cleft of primary palate occurs when the lateral palatine process fails to fuse with the median palatine process.
Cleft of the secondary palate, posterior to the incisive foramen, occurs due to partial or complete failure of fusion of right and left lateral palatine processes.
Cleft of the primary and secondary palate or complete palatal cleft is a result of a lack of fusion between the three palatine processes with each other and with the nasal septum. The severity depends on the extent of the cleft.
Bifid uvula is due to non-union of the distal end of both the lateral processes.
Depicts schematic illustrations ofgeneral types ofclef lip and palate with actual clinical pictures for a few cases.
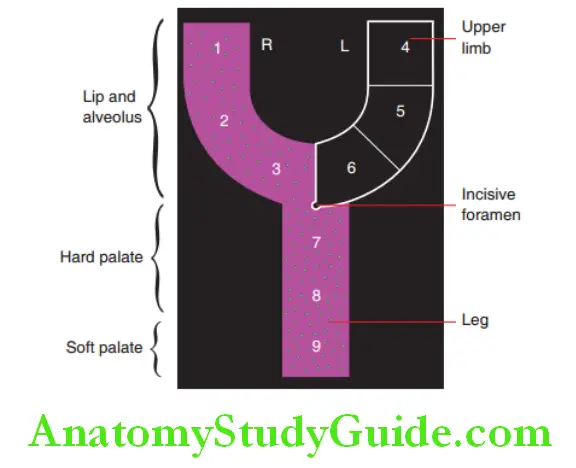
Kernahan’S ‘Y’ Graphical Method
The ‘Y’ graphical method by Kernahan is a popularly used method to classify cleft lip and palate. A pictorial view of the deformity can be obtained through this classification.
The design, in the shape of the alphabet ‘Y’, with two free upper limbs and one leg and is divided into nine parts.
The parts are numbered from 1 to 9 and each numeral denotes an area ofthe lip, palate or alveolus. The region where the clef occurs is marked by stippling or with bands.
The free upper limbs are numbered from 1 to 6 and represent the lip and alveolus.
Parts 1 and 4 denote the area of fusion between the medial nasal process, lateral nasal process, and maxillary process at the root of the nose.
This area forms the lip. Parts 2 and 5 denote the area of fusion between the maxillary process and medial nasal process. This forms a part of the lip and alveolus.
Parts 3 and 6 denote the area of fusion of the maxillary process and medial nasal process forming the alveolus anterior to the incisive papilla.
Parts 7, 8, and 9 form the leg part of the ‘Y’ design. The incisive papilla is depicted by a dot at the junction of the upper limbs and the leg.
It is in between parts 3, 6, and 7. Parts 7, 8, and 9 denote the area of fusion of lateral processes and the median palatal process.
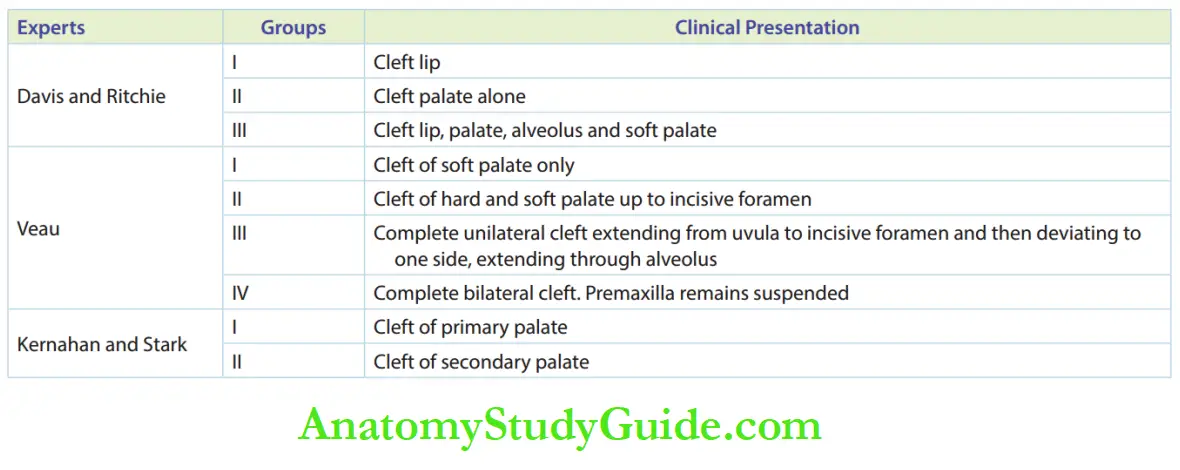
Parts 7 and 8 form the area of the hard palate posterior to the incisive foramen. Part 9 forms the soft palate. Other experts have classified the orofacial cleft as in Table.
Age-Related Sequelae Of Cleft Lip And Cleft Palate
Patients having cleft lip and/or cleft palate suffer from different problems at various age levels.
The patient may suffer from defective oral functions, compromised speech, poor facial aesthetics, and the resultant psychosocial ill effects.
Presently, with improved health care and increasing awareness, clef patients are identified and treated early.
Sequelae Of Clefts In Neonates:
A child is described as a neonate up to 6 months from birth.
The following problems are identified in a neonate suffering from cleft lip and/or cleft palate:
Regurgitation of milk is likely due to lack of palatal partition between the nasal and oral cavities.
The control of the flow of milk is likely to be affected in the absence of a palatal shelf. There is a possibility of aspiration, sometimes endangering life.
Compromised suckling of milk in cleft palate patients leads to malnutrition and growth retardation.
As the nasal cavity is in direct contact with the oral cavity, frequent upper respiratory tract infection occurs in the patients. This has adverse effcts on the general growth ofthe neonate.
Patients with Pierre Robin syndrome suffer from cleft palate and micrognathia mandible. This leads to glossoptosis or fallback of the tongue. There is a possibility of the tongue obstructing the airway of the neonate.
Sequelae Of Clefts In Toddlers
A child is described as a toddler between 6 months and 3 years of age. A toddler suffers from all the problems faced by a neonate along with auditory and speech problems.
Abnormal insertion of the palatal muscles such as the levator veli palatini and tensor veli palatini causes dysfunction of the auditory tube. Frequent upper respiratory tract infections also affct the auditory tube.
Velopharyngeal incompetence is the failure of liftng of velum (sof palate) to contact the pharyngeal wall.
This occurs due to lack of palatal continuity. The quality of voice is altered due to this velopharyngeal insufficiency.
Excessive emission of air through the nose leads to increased resonance of sounds such as ‘n’ and ‘m’. This causes a characteristic hypernasality in the speech of a cleft palate patient.
Sequelae Of Clefts In Early And Late Childhood Years:
Children suffering from cleft lip and/or cleft palate can have dental and skeletal disturbances as they grow.
This can lead to compromised functions of the oral structures Swallowing, mastication and speech is affected due to poor occlusion and the inability to produce the required negative pressure to perform these functions.
Factors such as poor facial aesthetics and speech and hearing problems damage the individual’s self-image and affct the patient psychologically.
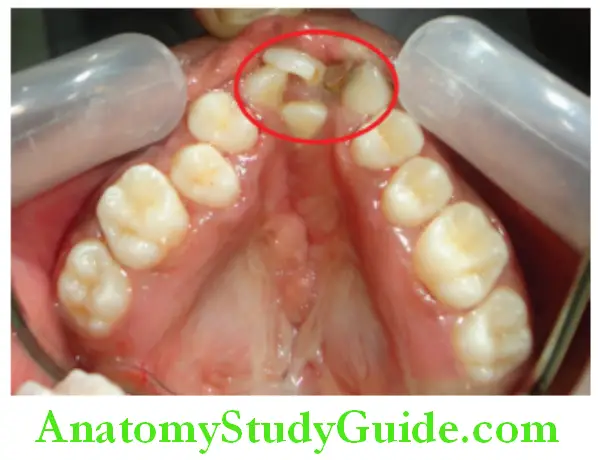
Dental Disturbances:
A clef in the alveolus can cause discontinuity in the alveolar arch. The discontinued alveolus causes disruption of the dental lamina.
The dental follicles arising from the dental lamina at the site of the clef are disturbed. The number, size, and shape of both the primary and permanent teeth are altered.
Various aberrations such as missing, hypoplastic, dilacerated, malformed, and supernumerary teeth can occur in the clef region of the alveolus. Ectopic eruption of teeth belonging to the clef region is also witnessed.
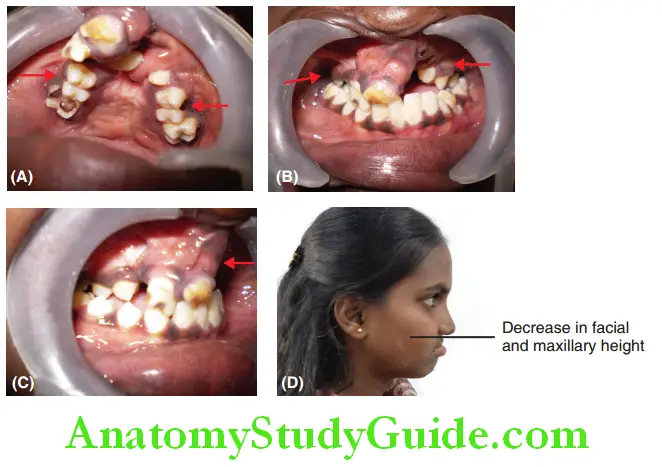
Skeletal Disturbances:
Clef lip or cleft palate can cause growth retardation of the maxilla in all three dimensions.
- Anteroposterior deficiency results in a concave profile, class III skeletal problem with a normal mandible and skeletal anterior crossbite.
- Vertical deficiency results in short columella causing widening of nares.
- Transverse deficiency results in collapsed arches and skeletal posterior crossbite.
Depicts a clef palate case with defiiency in the growth of maxilla in all the three dimensions. Anteroposterior defiiency can be noticed as anterior crossbite.
Transverse plane defiiency can be noticed as posterior crossbite. Vertical defiiency can be noticed as a decrease in facial and maxillary height.
Sequential Protocol Of Management
Prenatal identification of a facial cleft in the fetus can be done as early as 15 weeks of pregnancy. Ultrasound scanning can detect facial cleft, if any.
Three-dimensional ultrasonography is a new technology that helps in viewing the fetal face with good clarity.
If investigations reveal a facial clef in the fetus, psychological counseling of the expecting parents becomes highly essential.
It allows the parents to accept the situation and avoid disappointment and guilt. It also gives them an opportunity to investigate other structural or chromosomal abnormalities in the fetus.
The parents should be provided with thorough knowledge about neonatal care and feeding and surgical requirements of the baby aftr delivery to handle the situation properly.
The cleft of the lip and/or palate is a craniofacial anomaly that has to be managed by a team of specialists listed in Box.
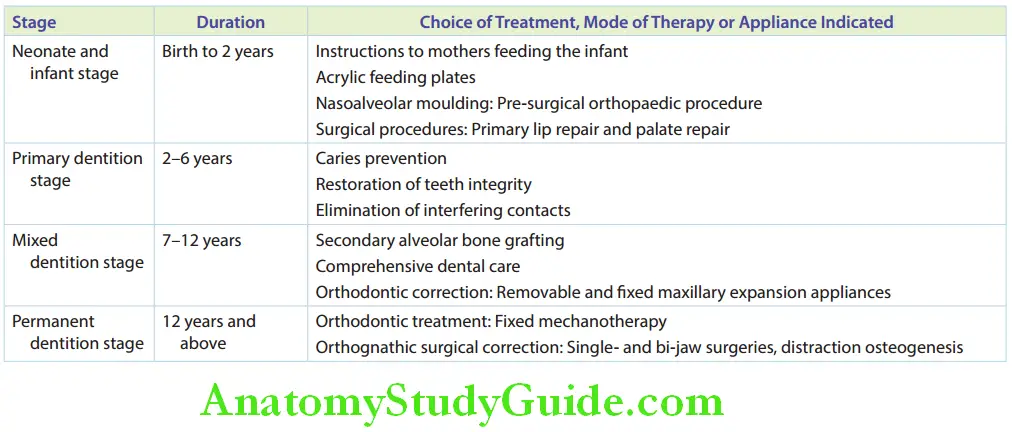
The treatment is provided across four distinct developmental periods. The reason for managing the clef in separate phases is to have a time-bound framework for achieving definitive objectives.
The four stages in which treatment is provided are as follows:
- Neonate and infant stage
- Primary dentition stage
- Mixed dentition stage
- Permanent dentition stage
Neonate And Infant Stage:
This stage extends from the birth of the child up to 2 years of age.
The treatment in this period includes the following procedures:
- Instructions to mothers feeding the infant
- Acrylic feeding plates
- Naso-alveolar molding (NAM)
- Surgical procedures
Instructions to Mothers Feeding the Infant:
The following are the specific instructions given to mothers feeding a child with cleft lip and/or cleft palate:
- Infants should be supported at 45°–60° to prevent nasal regurgitation.
- The nipple should be directed at any intact part of the palate.
- The bottle should be tilted gently to maintain liquid in the nipple.
- Mild pressure must be applied on the lower jaw of the infant to encourage feeding.
- The infant must be made to burp after a feed of every half to one ounce.
- Lengthy feeding should be avoided as it only tires the infant and burns more calories than the intake.
In conditions where feeding by the mother is difficult, she can opt to feed expressed breast milk at regular intervals. Feeding bottles with modified nipples are useful in some cases.
A nipple with a cross-cut is also suggested. The size of the cross-cut can be customized as per the volume of flow required.
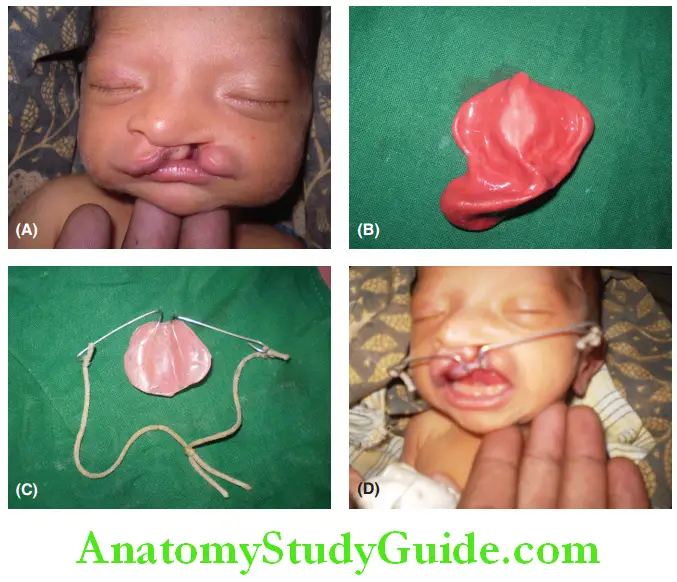
Acrylic Feeding Plates:
The negative pressure created in the oral cavity enables swallowing. This happens when the soft palate elevates to seal the nasopharynx from the oropharynx.
Swallowing is compromised in an infant with a cleft palate as this negative pressure is not created. Breastfeeding of such infants is generally difficult or not successful as it can lead to nasal regurgitation.
Suckling action is equally inefficient in the case of alveolar cleft
An acrylic feeding plate is indicated to cover the cleft in the palate. It acts as the palate and compartmentalizes the nasal and oral cavities.
This helps in creating the negative pressure required for suckling and swallowing.
The feeding plate is constructed on a model cast of the infant’s upper jaw.
It is held on the palate with the help of soft elastic cords around the infant’s head. Small non-interfering hooks are provided on the anterior part of the plate for engaging the elastic cord.
Naso-Alveolar Moulding (NAM):
NAM is a maxillary pre-surgical orthopedic procedure aimed at aligning the displaced lip and palatal segments back to their arch form.
It is indicated in the case of the cleft of the alveolus and the palate. The procedure begins on the first day of birth of the infant and is completed within 6–8 weeks of birth.
Clef divides the alveolus into segments. These segments are displaced either towards or away from the midline.
Nasoalveolar molding gradually brings the segments to an arch form and in proximity to each other.
Impression of the newborn’s upper alveolus is recorded with utmost care and an acrylic plate is fabricated. The plate is strapped to the cheeks with the help of adhesive tapes.
The plate is reshaped every week to guide and bring the alveolar segments to an acceptable form. Th plate also serves as feeding plate.
At an appropriate time, a nasal stent is added to the plate to re-establish the contour of the nose on the clef side.
The NAM procedure approximates the ends of the lips, alveolar segment, and palate. Th surgical repair of the lip, alveolus and palate follows this procedure.
NAM reduces the tension across the sutures placed during surgical repair. Ths decreases the chances of postsurgical scarring, dehiscence and related complications.
Surgical Procedures:
Th surgical protocol for treating cleft lip and cleft palate is one of the most controversial topics.
The opinion of practitioners regarding the age at which the surgery can be performed varies with different treatment centers.
The decision regarding the technique to be adapted also depends upon the team of specialists involved in the management.
The surgeries involved in managing cleft lip and cleft palate have been discussed briefly. The description of individual surgeries is beyond the scope of this book.
The reader is advised to refer to appropriate surgical textbooks for further details.

Primary Lip Repair:
The general health condition of a child decides the age of the indication of primary lip repair.
According to Milliard’s rule of ten, a child is fit for cleft lip repair surgery when the age of the infant is 10 weeks, the weight of the infant is 10 lb and the hemoglobin level is 10 g.
Primary lip and anterior palate repair can be performed at around 3 months of age.
This is considered a safer age because the growth of the infant allows easier surgical repair and lesser anesthetic complications.
The common surgical approaches for lip repair are as follows:
1. Lip adhesion: The procedure involves an incision in the anterior vestibular sulcus area. The soft tissues on the external surface of the maxillary segment are undermined.
This procedure is indicated to reduce lip tension.
2. Collito–Walker (CW) technique: It is a lip repair procedure without undermining of soft tissues.
3. Millard rotation advancement flap: This procedure is more commonly followed to achieve acceptable lip morphology.
C-flops or small triangular flaps are made at the base of the columella and the edges are appropriately sutured. Z-plastic is done on the vestibular side.
Tennison unilateral cleft lip incision: This is a procedure indicated for bilateral cleft lip repair.
Other less commonly followed surgical approaches for primary lip repair are as follows:
- Manchester’s method
- Skoog’s method
- Wynn’s method
- Spina’s method
- Barsky technique (Veau II)
Cleft Palate Repair:
The infant’s fitness, age, and type of clef determine the surgical technique for clef palate. Palatal repair is considered necessary before speech development.
Consultation with an audiologist and an ENT specialist is advised at around 12–14 months of age to assess hearing and articulating ability.
The first surgical closure of the cleft palate is the primary palatoplasty. It can be performed by 12–18 months of age.
A revision of this procedure is secondary palatal management. Pharyngoplasty or pharyngeal flp surgery may be indicated later on.
The other surgical approaches are as follows:
- Von Langenbeck mucoperiosteal flap
- Von Langenbeck procedure with levator reconstruction
- V-Y pushback procedure
- Veau–Wardill–Kilner procedure
Primary Dentition Stage:
This stage extends from 2 to 6 years of age. The cooperating ability of the child is limited at this age. Hence, active orthodontic treatment proves futile at this stage.
The position and presence of primary teeth may be aberrant in the region of the cleft.
The treatment provided in this stage includes the following:
- Caries prevention
- Restoration or rehabilitation of the integrity of primary teeth
- Elimination of interfering contacts in the case of functional shifts due to anterior crossbite
Mixed Dentition Stage:
This stage extends from 7 to 13 years of age. The following procedures are indicated in this stage:
- Bone grafting
- Pediatric dental care
- Orthodontic correction
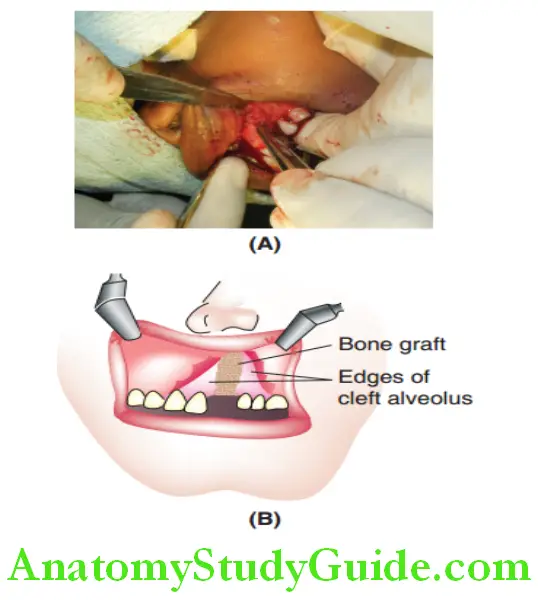
Secondary Alveolar Bone Graft:
Thre is discontinuity of bone at the site of the clef in the alveolus. The missing alveolar bone is restored in the mixed dentition stage with a secondary alveolar bone graft.
The continuity of the alveolar ridge is essential to allow teeth to erupt in place. It also provides the medium of bone for orthodontic movement of malposed teeth into appropriate places.
The ideal time to perform the bone grafting procedure depends on the location of the cleft If the clef is mesial to the lateral incisor, the graft has to be done before its eruption time, which is around 8 years of age.
If the clef is mesial to the canine, then the grafting is done at around 10 years of age.
A cancellous bone graft is preferred over cortical bone due to better osteogenic potential. The bone for grafting can be harvested from the ilium, cranium, or mandibular symphysis.
A mucoperiosteal flap is raised on either end of the clef to expose the bony edges. The graf is packed into the clef between the bony edges.
The flaps are sutured over the graf to reconstruct the arch form.
The bone grafting procedure offers the following advantages:
- Support to unerupted teeth and teeth near cleft
- Closure of oronasal fistula
- Support and elevation of the alar base
- Continuity of the arch form and alveolar ridge
- Stabilisation of premaxilla
Comprehensive Dental Care:
The patient and the parents are educated about oral hygiene practices. Prosthodontic replacement for missing anterior teeth is very important for the psychological benefit of the patient.
The decayed teeth around the clef region are restored before graft procedures are performed.
Consultationwithaspeechtherapistprovesbenefiial at this stage, especially with the alveolar graf in place.
Orthodontic Correction:
Permanent teeth in the clef region are generally missing. These teeth adjacent to the clef are rotated, malformed, or misplaced.
The following appliances are indicated in this stage to correct the malocclusions:
Minor irregularities are corrected with the help of a sectional fixed appliance using two molar tubes and brackets on four incisors.
- Maxillary expansion appliance with hyrax screws is indicated to produce skeletal expansion of the maxilla.
- Removable expansion appliances using slow expansion screws can be provided in the anterior and posterior segments to correct an anterior and posterior crossbite, respectively.
- Fixed appliances are preferred as they do not depend on the cooperation of the patient. Selective expansion is achieved by providing field appliances such as slow-expansion tri-helix and quad-helix appliances.
- Reverse-pull headgear is indicated to correct the anteroposterior deficiency of the maxilla. It delivers a tractional force to protract the maxilla forwards and downwards.
- A palatal spider expansion appliance is indicated to correct the transverse maxillary deficiency. It produces differential expansion in the premolar and canine regions.
Permanent Dentition Stage:
The growth spurt and the remaining skeletal growth resolve the facial skeletal and dental discrepancies.
Maxillary deficiency and comparative prominence of the mandible become more evident. Occlusal disturbances may also surface as teeth erupt.
A comprehensive treatment plan has to be derived depending on the severity of the underlying problem and the patient’s informed choice. Treatment options are as follows:
- Orthodontic treatment
- Orthognathic surgical correction
Orthodontic Treatment:
Orthodontic treatment is suggested to camouflage the skeletal disproportion. It involves regular fixed appliance therapy to bring positive overjet, overbite, and acceptable occlusal settling.
The teeth adjacent to the clef region are aligned with fixed orthodontic mechanotherapy. Space is provided for prosthodontic replacement of missing teeth in the region of cleft
Orthognathic Surgical Correction:
Orthognathic surgical procedures involve single or bi-jaw surgeries. Le forte procedure is performed to reposition the maxilla in the forward and downward directions.
Bi-jaw surgeries reposition the maxilla along with mandibular setback. Distraction osteogenesis is a more stable maxillary advancement procedure.
Distraction Osteogenesis:
In this procedure, corticotomy or osteotomy is performed at the site of intended bone formation. A distraction device is found at the surgical site. Healing of the region occurs in a few days.
When healing is initiated, tractional force is exerted by the distraction device at the surgical site. This leads to the formation of new bone and associated tissues in the healing site.
The device is activated such that it promotes new tissue formation at the rate of 1 mm per day.
The magnitude and vector of bone formation are controlled by activating the device for a required number of days.
Relapse of the problem is minimal after this procedure as actual bone formation occurs along with the soft-tissue matrix.
The cleft lip and palate patient needs to be periodically reviewed until skeletal maturity and a few years further on, to check if treatment results are stable.
Summarises the sequential protocol to be followed in the management of cleft lip and/or cleft palate.
However, since no two clef cases are similar, treatment has to be customized as needed. Results are equally varying, depending on many factors.
Summary
1. The face develops from four processes or four ‘primordia’ during the fourth to seventh week of intrauterine life, namely the frontonasal process, right maxillary process, left maxillary process, and mandibular process.
2. Cleft lip and cleft palate occur due to a lack of merging or fusion of these processes.
3. There exist various forms of cleft lip and cleft palate:
4. Ultrasonic scanning after 15 weeks of pregnancy can detect facial clefts if present.
- Patients with cleft face problems at all age levels with regard to function, speech, and aesthetics.
- Retardation of growth occurs in the dentofacial region.
5. Dental aberrations are seen frequently: Teeth being malformed in size and shape, hypoplastic, absent, dilacerated, ectopically erupted teeth, and supernumerary teeth.
6. The cleft team: The cleft craniofacial anomaly is best managed with a team of specialists.
Treatment: The timing and sequencing of treatment are divided into four distinct developmental periods.
Neonate stage: Feeding plate, neonatal ‘naso-alveolar molding’ (NAM)
Primary dentition stage: Initiating orthodontic treatment: caries control, eliminate tooth interference leading to jaw shifts.
Mixed dentition stage: Alveolar bone grafts, sectional fixed appliance, reverse-pull headgear, and expansion with hyrax screws.
Permanent dentition stage: Orthodontic treatment to camouflage skeletal disproportion, distraction osteogenesis, and orthognathic surgical correction.
Leave a Reply