Diet And Dental Caries Introduction
Several clinical studies and scientific data are available to document the clinical correlation between diet and dental caries. The risk of occurrence of caries can be assessed by the diet consumed by the individual. The strategies of preventing caries are employed accordingly.
Table of Contents
Epidemiologic studies have shown that the incidence of dental caries differs immensely among different populations, depending on their native diet. The prevalence of caries in a population consuming a diet with a significantly lower refined carbohydrate content is much lower than that in developed countries consuming more refined food.
During World War 2, there were harsh restrictions on the consumption of refined carbohydrate sugars and confectionaries. The incidence of caries had come down considerably at that time. As the sugar restrictions were lifted after the war, dental caries became prevalent once again.
Read And Learn More: Paediatric Dentistry Notes
Institutional studies are the most popular studies on diet and dental caries. These studies prove a direct association between diet and dental caries.
- Vipeholm study: A study was conducted with 456 adult inmates in an institution for the mentally challenged at Vipeholm Hospital in Lund, Sweden. The diet provided in the institution contained very little sugar and there were no snacks in between meals for the patients. The investigations revealed that the rate of dental caries was relatively low. The conclusions made from the study are listed.
- Conclusions from Vipeholm Study
- An increase in carbohydrates (mostly sugar) definitely increases the caries’ activity
- The risk of caries occurrence is greater if the sugar is consumed in a form that will be retained on the teeth surface
- The risk of sugar increasing the caries activity is greatest if the sugar is consumed in between meals and in a form that tends to be retained on the surfaces of the teeth
- Upon withdrawal of sugar-rich foods, the increased caries activity rapidly disappears
- Carious lesions may continue to appear despite the avoidance of refined sugar and maximum restriction on natural sugars and dietary carbohydrates
- A high concentration of sugar solution and its prolonged retention on the tooth surfaces leads to increased caries activity
- The clearance time of the sugar corresponds closely to the caries activity
- Th Vipeholm study clearly revealed the fact that the physical form of carbohydrates, that is stickiness, oral clearance time and frequency of intake are much more important in producing caries than the total amount of sugar consumed.
- Conclusions from Vipeholm Study
- Hopewood House children: The dental status of children between 3 and 14 years of age residing at Hopewood House, Bowral, New South Wales, was studied longitudinally for 16 years. The children consumed a nutritionally adequate vegetarian diet. No meat was provided but the children ate egg yolk occasionally. There was a rigid restriction on refined carbohydrates. The diet was referred to as a ‘Spartan diet’ by authors as it seemed like a ‘military menu’. The Hopewood House children were compared with the children amongst the general population with reference to caries incidence and prevalence. The first assessment was done after 10 years of the commencement of the study comparing 13-year-old children of the institution with those of the general population. The comparison and results of this assessment are listed. The children leave the house when they turn 13. They mingle with the urban population and are exposed to an urban-refried diet. The DMFT score of these children was tested after 5 years and compared with the general population. The conclusions of the study point that the type of diet has an influential role in determining the decay susceptibility of the individual. An increase in the caries index leading to deleterious effects on dental health can be because of a strongly cariogenic diet. Another fact was that the teeth that were caries-free in childhood however did not acquire any permanent immunity towards caries.
- Conclusions from the Hopewood House Study
- Very low decay incidence in children on the ‘Spartan diet’: 53% of the 13-year-old institutionalised children were decay free as compared to 0.4% of the general population of the same age group
- Prevalence of decay amongst 1/10th of the general population: 13-year-old Hopewood House children had a mean DMFT of 1.6 whereas the value for the same age group of the general population was 10.7 (greater than 10 times)
- Low decay incidence and prevalence were reported among children with poor oral hygiene: In contrast to the very low decay incidence, the Hopewood House children had poor oral hygiene with 75% prevalence of gingivitis, which points to the fact that caries reduction is solely because of DIET
- Hopewood House children who consumed a normal urban diet for 5 years from age 13 to 18, had almost the same DMFT as that of the general population: This proved that the cariogenic-refined diet influences decay and that earlier abstinence from taking urban, refined diet had brought no immunity against dental decay.
- Conclusions from the Hopewood House Study
- Turku sugar studies: The Turku sugar studies were a series of collaborative studies carried out in Turku, Finland, by Scheinin and Makinen. The study was conducted to test the effects of the chronic consumption of three different sugars, namely sucrose, fructose and xylitol, on dental and general health. 125 subjects were classified into three groups – sucrose, fructose and xylitol. Each individual of the group was given any type of diet with only that particular sugar. This implies that an individual of the sucrose group had no exposure to fructose and xylitol. The study was done after 2 years of strategic exposure of one group of sugar to subjects. The results drawn and conclusions made from this study are listed.
- Conclusions from Turku Sugar Studies
- The sucrose group had the maximum incidence of decay: Sucrose is the ‘arch criminal’ of dental caries
- Fructose had caries incidence similar to sucrose for the first year but demonstrated lesser decay incidence in the second year: Fructose is cariogenic but to a lesser extent than sucrose
- Dramatic reduction in the incidence of dental caries in the xylitol group: Xylitol is non-cariogenic.
- Conclusions from Turku Sugar Studies
Another part of the study tested the efficiency of chewing xylitol bubble gums in between meal times for decay prevention. Any sugar is metabolised in the oral cavity by a corresponding dehydrogenase enzyme. This metabolism produces lactic acid through glycolysis, which promotes the demineralisation of enamel and causes tooth decay. The dehydrogenase enzyme for xylitol, xylitol dehydrogenase, is absent in saliva. Hence, this polyhydric alcohol is not metabolised in saliva. There is no lactic acid formation; hence, it is noncariogenic.
It was concluded that chewing xylitol bubble gums in between meal times reduced the number of carious lesions, with remineralisation of early carious lesions. This effect was demonstrable with any individual chewing more than 2.5 chewing gums a day. Thus, xylitol was concluded to be anti-cariogenic.
Cariogenicity Of Foods
Sucrose has been labelled as the ‘arch criminal’ of dental caries. The biochemical explanation given for this unique role of sucrose is that the free energy of hydrolysis of sucrose when expressed as calories per mole is about 6700 compared to about 3000 for lactose or maltose. The high-energy bond linkage between the C-1 of glucose and the C-2 of fructose is believed to be particularly suitable for microbial production of extracellular dextrans and levans. Mixtures of glucose and fructose are as cariogenic as sucrose. The influence of trace elements on the prevalence of dental caries is a subject of continuous and expanding research.
- Trace Elements
- The inverse relationship between caries prevalence and fluoride (F) intake is widely recognised. This prompted investigators to look into the effects of other trace elements. It is thought that molybdenum (Mo), selenium (Se), vanadium (V), strontium (Sr) and a variety of other elements may have an influence on the prevalence of caries in man. There is evidence to prove that ingestion of selenium during tooth formation actually increased dental caries in human beings and experimental animals. Cariostatic effects have been claimed, but not proven, for a number of these trace elements.
- Caries-Inhibiting Foods
- Sugars are cariogenic foods. Similarly, there is food stuff that inhibits dental caries. These are called caries inhibitor foods. Food products that contain calcium and phosphates and fats inhibit caries. The mode of action of calcium/phosphates and fats to prevent dental decay is listed.
- Ways of Caries Inhibition by Calcium and Phosphates and Fat
- Calcium and phosphates
- Reduce the rate of dissolution of hydroxyapatite
- Decrease the fall in plaque pH by buffering acids produced by bacteria
- Enhance remineralisation
- Modify the composition of pellicle and plaque
- Fats
- Replace carbohydrates that are relatively more cariogenic
- Form a high surface-tension protective barrier on enamel
- Inhibit glycolysis in dental plaque
- Calcium and phosphates
- Ways of Caries Inhibition by Calcium and Phosphates and Fat
- Calcium and phosphates are present in multiple plant and animal sources such as milk, egg, pulses, dal and meat. A balanced diet (discussed later in the text) contains fat in minor amounts, which is adequately useful as an anti-cariogenic.
- Sugars are cariogenic foods. Similarly, there is food stuff that inhibits dental caries. These are called caries inhibitor foods. Food products that contain calcium and phosphates and fats inhibit caries. The mode of action of calcium/phosphates and fats to prevent dental decay is listed.
- Sucrose Alternates Sucrose alternates may be artificial sweeteners or sugar substitutes. These are non-cariogenic sugars and can be suggested in the diet of diabetic patients as well. Artificial sweeteners are called non-caloric sucrose alternates. Non-caloric sweeteners, also referred to as intense sweeteners, are much sweeter than sugar. Thy yield little or no energy and provide no bulk. They are used in very small quantities, especially in drinks, or blended with sugar substitutes in food and snacks. Non-caloric sweeteners commonly used are aspartame, cyclamate, saccharine and acesulphame-K. Sugar substitutes are referred to as caloric or nutritive sugar substitutes or as carbohydrate sugar substitutes because they are carbohydrate or carbohydrate derivatives. The most important group of sugar substitutes is called polyhydric alcohols or polyols. They can be metabolised to yield energy and they add to the bulk of food products. As they are less sweet than sucrose, they often require blending with intense sweeteners. Their main commercial value lies in products for diabetic patients and non-cariogenic diets. Caloric sweeteners commonly used are Lycasin, Sorbitol, Xylitol, Lactitol, Mannitol, Maltitol and Palatinol. Xylitol is a non-cariogenic sugar. The dehydrogenase enzyme required for the metabolism of xylitol is absent in saliva. So, it is an anti-cariogenic sugar also.
Balanced Diet
Carbohydrates, proteins, fats, vitamins, minerals and fibre (roughage) are the various classes that constitute a diet. The ideal proportion of the various classes is demonstrated by a pictographic representation simulating a pyramid. This is termed a food pyramid. A strategic diet that follows the principles depicted in the food pyramid is called a balanced diet.
The Food Guide Pyramid for young children was designed by the US Department of Agriculture to promote healthy nutrition in children from the age of 2–6 years.
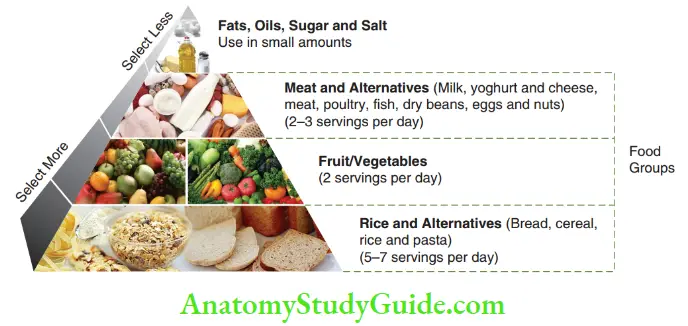
The main emphasis of the food pyramid is on the five major food groups, all of which are required for good\ health. The volume of area allotted to a particular class of food depicts its share in the diet. The food given at the base should be in higher quantities and that at the apex should be consumed least.
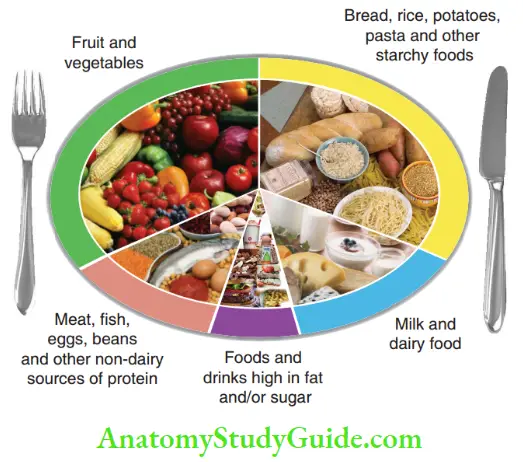
The balanced diet is also pictographically represented by an ‘Eatwell plate’ in Figure. The plate is divided into three parts. One-third is covered with rice and other carbohydrate sources. Fruits and vegetables cover another one-third. The remaining one-third is divided into three parts, covering milk and dairy (14%); meat, pulses and egg (14%); and fat, oil and sweet (6%), respectively.
Diet History
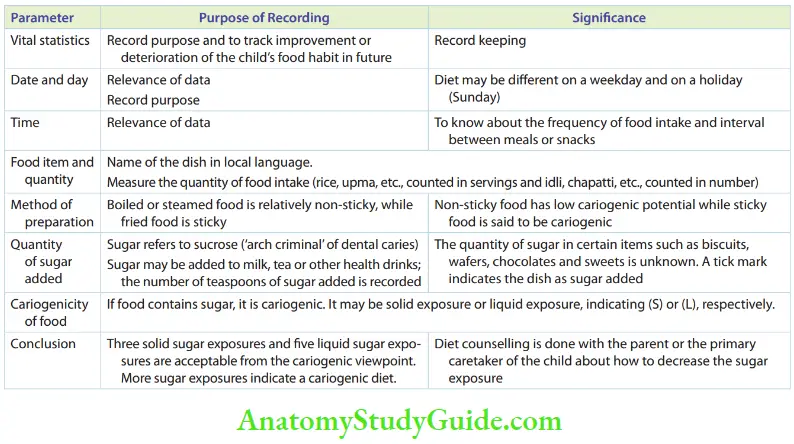
Since diet is one of the primary aetiologic parameters of dental caries it is important to study the dietary intake of a child, especially the one who demonstrates a high caries index. Recording of the dietary intake of the child is referred to as ‘diet history’. Table lists the necessary parameters recorded in a diet history. The diet history may be recorded as a 1-day diet chart, 3-day diet chart, 5-day diet chart, 1-week diet history or 1-month diet diary. The diet history is obtained from the mother or the primary caretaker of the child.
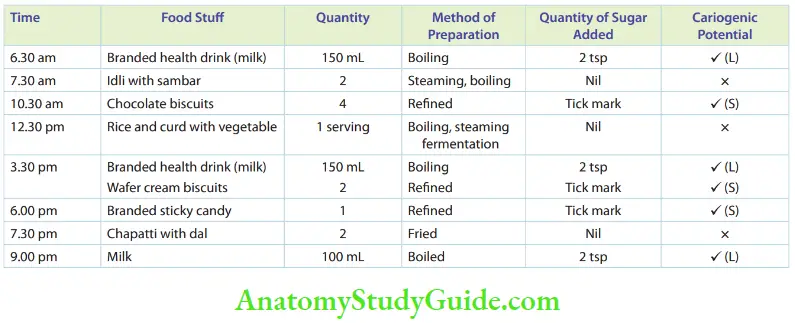
A model of a 1-day diet chart of a 7-year-old boy is given in Table.
Diet Counselling
The best nutrition advice that can be given to keep a child healthy includes the following:
- Eat a variety of food
- Balance the food taken with physical activity
- Choose a diet with plenty of grain products, vegetables and fruits
- Choose a diet low in fat, saturated fat and cholesterol
- Choose a diet moderate in sugars and salt
- Choose a diet that provides enough calcium and iron to meet the growing body’s requirements
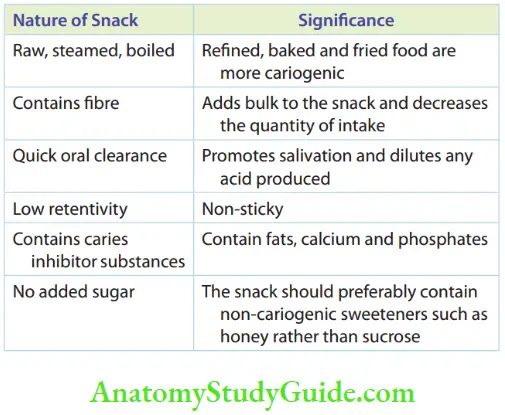
- Ideal Snack The main cariogenic potential of a child’s diet in most cases is because of the snacks taken by the child. Snacking is the consumption of food in between meals. It is not a healthy regimen. As it has become common in today’s life, one should focus on consuming healthy snacks than junk food. One sugar exposure decreases the oral pH making it acidic which is conducive to tooth decay. After ingestion of food, the oral pH ascends from the acidic to the neutral level in about 1½–2 hours. Meanwhile, one exposure of sugar (through snacks) prevents the oral pH from returning back to the neutral level. The pH stays in the acidic range. This enhances the caries susceptibility of the child. However, when snacks cannot be avoided, the choice of the snack should be such that it makes a negligible or no increase in caries susceptibility. An ideal snack that does not increase caries susceptibility is discussed in Table. Preferable or relatively acceptable snacks include boiled chana, boiled groundnuts, dry fruits, raw cut fruits, baked potato wafers and baked rice items. The worst choice of snacks with regard to tooth decay includes caramel chocolates, cream biscuits, chips, sticky candy and conventional Indian sweets such as laddu, Mysore pak and rasagullas. Since snacking is an indispensable part of a child’s diet, the choice of an appropriate snack should be presented to the parent during diet counselling.
Diet And Dental Caries Summary
- The clinical correlation between diet and dental caries has been well documented with the following scientific data/clinical studies:
- Epidemiological studies comparing primitive diets
- Wartime diet analyses
- Institutionalised studies
- Vipeholm study
- Hopewood House study
- Turku sugar study
- Cariogenicity of foods: Sucrose is the ‘arch criminal’ of dental caries. It is a highly cariogenic sugar. Phosphates and fats are caries-inhibiting foods. Xylitol is a non-cariogenic sugar.
- Sucrose alternates: They may be sugar substitutes or artificial sweeteners. Sugar substitutes are also referred to as caloric or nutritive sugar substitutes or as carbohydrate sugar substitutes. Artificial sweeteners are noncalorific sucrose alternatives.
- Balanced diet: A strategic diet that includes an ideal proportion of carbohydrates, proteins, vitamins, minerals, fat and fibres constitutes a balanced diet. It is pictographically depicted by a food guide pyramid.
- Diet history: It is a record of the dietary intake of a child obtained from the parent or the primary caretaker. The parameters recorded for diet history and an example of diet history are listed in Tables 27.1 and 27.2, respectively.
- Diet counselling: It is the nutrition advice given for the child to be healthy. It is important to discuss about ideal snacks during diet counselling. An ideal snack should be less caries conducive.
Leave a Reply