Introduction To Endodontics
Endodontics is the branch of dentistry which deals with diseases of the dental pulp and periradicular tissues. En is a Greek word for “inside” and odont is the Greek word for “tooth.” Endodontics is the branch of dentistry which deals with morphology, physiology, and pathology of human pulp and periradicular tissues.
Table of Contents
The study of endodontics involves basic knowledge of pulp biology, etiology, diagnosis, treatment, and prevention of the diseases and injuries of the pulp and associated periradicular tissues.
Read And Learn More: Endodontics Notes
Scope Of Endodontics
- Diagnosis and differential diagnosis of orofacial pain of pulpal and periradicular origin
- Vital pulp therapy like pulp capping, pulpotomy, apexogenesis, and apexification
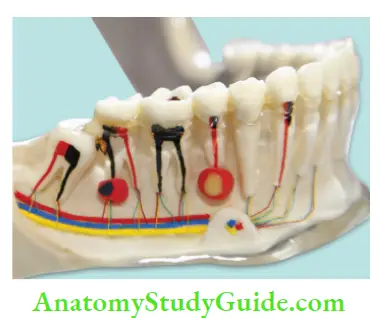
- Nonsurgical treatment of root canal system
- Surgical removal of periapical pathology of pulpal origin
- Bleaching of discolored teeth
- Re-treatment of endodontic failure cases
- Restorations of endodotically treated teeth with coronal restoration and post and core
- Intentional replantation
- Replantation of avulsed tooth
- Hemisection, bicuspidization and root resection
- Endodontic implants
History Of Endodontics
Endodontics has been practiced as early as 2nd or 3rd century BC. Th history of endodontics begins in 17th century, and since then, many advances, developments, and research work has been done continuously.
Advances in endodontics have been made continuously, especially after Pierre Fauchard (1678–1761) (founder of modern dentistry) described the pulp very precisely in his textbook “Le Chirurgien Dentiste.” Later in 1725, Lazare Riviere introduced the use of clove oil as sedative, and in 1746, Pierre Fauchard demonstratedthe removal of pulp tissue.
Dr. Grossman, the pioneer of endodontics, divided the evolution of endodontics in four eras from 1776 to 1976, each consisting of 50 years.
Prescience – 1776–1826
Age of discovery – 1826–1876
Dark age – 1876–1926
The renaissance – 1926–1976
Innovation era – 1977–till date

Prescience (1776–1826):
In this era, endodontic therapy was concerned with crude modalities like abscesses being treated with poultices or leeches and pulps being cauterized using hot instruments.
Age of discovery (1826–1876):
In this era, the development of anesthesia, gutta-percha, and barbed broaches happened. Th medications were created for treating pulpal infections, and the cements and pastes were discovered to fil them.
Dark age (1876–1926):
Inspite of introduction of X-rays and general anesthesia, extraction of tooth was the choice of treatment than endodontics because theory of the focal infection was the main concern at that time.
Th renaissance (1926–1976):
In this era, endodontics was established as science and therapy, forming its golden era. It showed the improvement in anesthesia and radiographs for better treatment results.
The theory of focal infection was also fading out, resulting in more of endodontics being practiced. In 1943, because of growing interest in endodontics, the AAE, that is, the American Association of Endodontists was formed.
Innovation era:
It is the period from 1977 onwards in which tremendous advancements at very fast rate are being introduced in the endodontics. Th better vision, better techniques of biomechanical preparations, and obturation are being developed resulting in the simpler, easier, and faster endodontics with more predictable results.
Also the concept of single visit endodontics is now globally accepted in contrast to multiple visits.
Contemporary Endodontics
Over the past two decades, knowledge of endodontic disease has improved like microbial biofims, etiology of persistent infection and factors affcting prognosis of endodontic treatment.
Management and prognosis in endodontics has improved because of advancements in materials, equipment, and techniques including nickel–titanium fies, apex locators, obturating materials, magnifiation, and endodontic microsurgery.
Contemporary culture-independent molecular techniques have exposed a more diverse microflra along with microflra of endodontic failure cases. Now, it has been established that rubber dam is mandatory for endodontic procedures.
If patient or dentist is allergic to latex, alternatives to latex like silicone-based dams are recommended. Modern endodontic diagnostic and treatment procedures utilize magnifiation, like dental loupes, microscopes, and endoscopes, which can provide magnifiation of up to ×25 times.
Magnifiation helps to
- Locate and negotiate root canals
- Visualize calcifid root canals
- Detect missed canals and remove fractured instruments
- Visualize tooth fractures
- Perform endodontic microsurgery
Conventional pulp tests (cold, heat, and electrical tests) assess conduction of nerves in the pulp, so these are not vitality but sensibility tests. Th results from thermal and electric tests are not quantitative and do not indicate the level of health or disease of the pulp.
But contemporary tests assess pulpal blood flw (laser Doppler flwmetry test), or oxygen saturation levels in the blood (pulse oximetry). Nowadays, digital radiography comes with many advantages like reduced radiation dose to patient, quick viewing of images, data storage, elimination of developing/fiing procedures, etc.
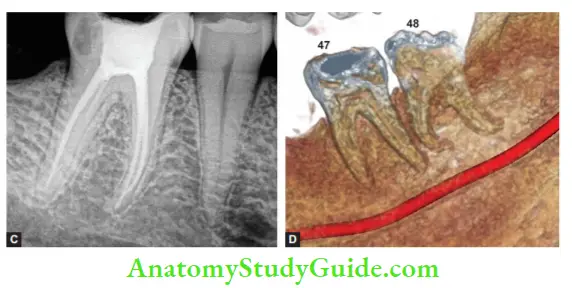
Cone beam computed tomography (CBCT) is a threedimensional imaging technique designed to overcome the limitations of radiographs. It produces undistorted and accurate images of target area. CBCT detects endodontic lesions before they become visible on conventional radiographs.
Earlier, pulp capping involved the use of calcium hydroxide, but now it is being replaced with mineral trioxide aggregate (MTA) which has better sealing characteristics, biocompatibility and form more predictable reparative dentine bridge than calcium hydroxide.
For cleaning and shaping, newer rotary NiTi files are replacing 2% stainless steel files. These files have different cross-sectional shape, taper, tip sizes, and presence or absence of radial lands. These are used in crown-down technique to
- Prevent pushing debris and necrotic tissue apically
- Eliminate coronal interferences, thus reducing the risk of iatrogenic errors
- Facilitate irrigants to reach apical area
Traditionally, working length was determined by radiograph, paper point method, etc., but now, electronic apex locator (EAL) are used which give consistently reliable results.
Earlier, silver points and lateral compaction technique was preferred for obturation, but nowadays, contemporary warm gutta-percha and thermoplasticized technique are employed to obturate the root canals.
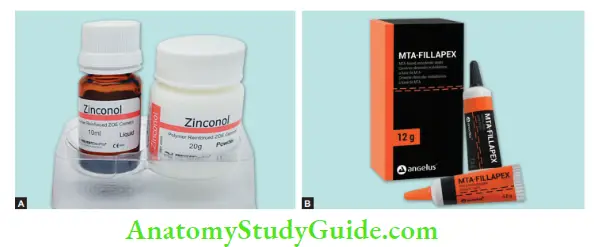
Since ages, zinc-oxide–eugenol-based sealers have been used in endodontics but now a days new adhesive, silicone and calcium phosphate-based root canal sealers have tried with desirable results .
Earlier, prognosis of endodontic treatment was evaluated as a “success” or a “failure.” These terms can be vague as they may be defined differently by the patient or the clinician. For example, a patient may feel symptom free endodontic treatment; however, a sinus may be present with periapical radiolucency.
Contemporary endodontics uses the terms “healed,” “healing,” or “diseased” to describe the outcome of treatment depending upon radiographic, clinical, and histological evaluation. Chance of a healed outcome after contemporary surgical endodontics can be as high as 95%.
Leave a Reply