Intraoral Radiographic Techniques Essay Questions
Question 1. Discuss in detail the principle and technique of paralleling periapical radiogra¬phy.
(or)
Describe in detail about long cone technique.
Answer:
Table of Contents
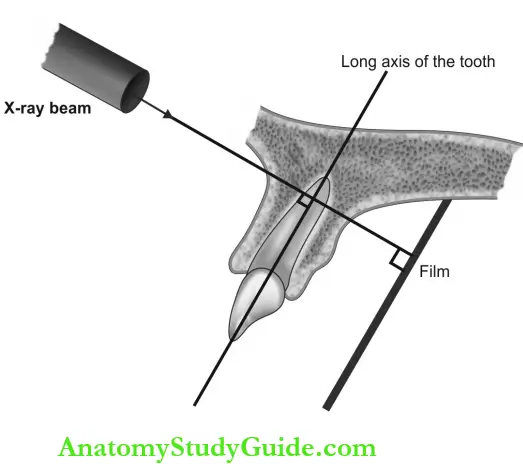
Principle of Paralleling Technique:
- It is based on the rule of parallelism such that the long axis of the film is placed parallel to the long axis of the tooth.
- The central beam is directed perpendicular to both film and tooth hence also called the right-angle technique. Thus the image of the tooth seen in the radiograph is the actual size of the tooth. X-ray source to object distance is more to achieve the parallelism hence also called the long cone technique.
Read And Learn More: Oral Medicine and Radiology Question And Answers
Intraoral X-ray machine—Exposure para-meters: 8 mA or 10 mA, 60-70 kVp.
Patient positioning: The patient must be protected with lead aprons with thyroid collars and instructed to remove the ornaments.
- The occlusal plane should be aligned parallel to the plane of the floor.
- The median sagittal plane should be perpendicular to the floor.
Maxillary projections: Patient is instructed to sit erect with back straight such that the ala-tragus plane is parallel to the maxillary occlusal plane
Mandibular projections: The patient’s head is tilted slightly backward to align the occlusal plane parallel to the floor.
Film placement:
- The film holder is essential to align the long axis of the film and the long axis of the teeth in a parallel plane.
- The exposure side of the film is placed facing the teeth surface.
- The identification dot should face an occlusal or incisal surface.
- Vertical film positioning for anterior teeth.
- Horizontal film positioning for posterior teeth.
- Teeth under examination should be in the center.
Paralleling Technique Cone Placement:
Maxillary projections
Mandibular Projections
Paralleling Technique Indications:
- To detect:
- Pulpal lesions [Dental caries (DC), frac¬ture, attrition, abrasion, erosion, pulp calcification, and pulp stones]
- Traumatic injuries in teeth and jaws
- Periapical lesions (apical periodontitis, periapical abscess, periapical granuloma, dental cyst, and radiopaque lesions like odontoma, condensing osteitis, etc.)
- Periodontal lesions (horizontal and vertical bone loss).
- Pericoronal lesions like dentigerous cysts
- Impacted or unerupted teeth and supernumerary teeth.
- Dental anomalies like dens invaginatus, dentin dysplasia, ghost teeth, etc.
- Structural alterations of teeth like Pamela- genesis and dentinogenesis imperfecta.
- In endodontics to determine pulp involvement and to identify the root length in the root canal treatment.
- Age estimation in forensic odontology.
Paralleling Technique Advantages: Accuracy is more with less chance for image distortion. The image is very representative of actual tooth size with maximum details and definition.
Paralleling Technique Disadvantages:
- The film holder is mandatory, and these devices in some cases cause lot of discomfort by impinging on oral tissues.
- Film placement is difficult in child patients or adults with a shallow palate and smallmouth.
Question 2. Explain in detail the bisecting angle technique.
(or)
Describe in detail about short cone technique.
Answer:
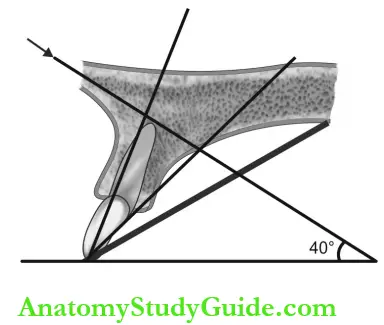
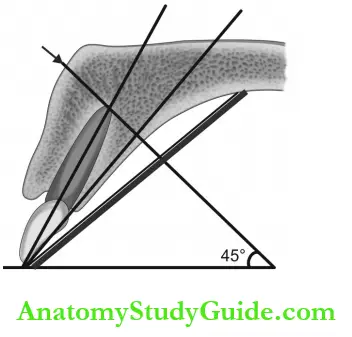
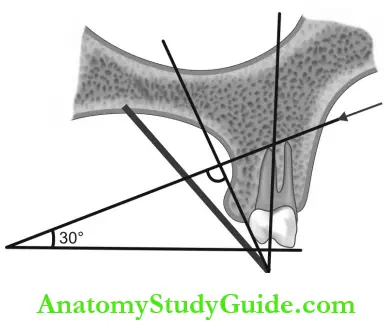
Principle of Bisecting Angle (Short Cone) Technique:
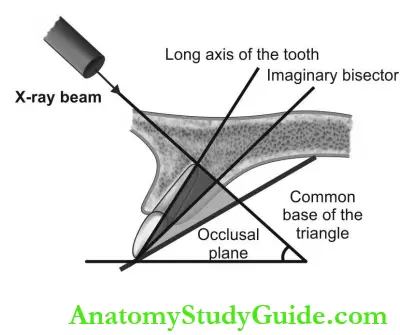
- Bisecting angle technique is based on Cieszynski’s rule of isometry which states that two triangles are equal when they share a common side and have two equal angles.
- The film is placed as close to the lingual surface of the tooth such that the plane of the film and the long axis of the tooth forms an angle at the apex.
- An imaginary bisector bisects this angle and represents the common side of the two triangles.
- The central beam is directed perpendicular to the bisector and forms the third side of both triangles.
Short Cone Technique: Intraoral X-ray machine—exposure para-meters: 8 mA or 10 mA, 60-70 kVp .
- Patient positioning: Patients are instructed to remove ornaments and wear lead aprons with thyroid collars for radiation protection.
- Maxillary projections: Patient is instructed to sit erect with back straight such that the ala-tragus plane is parallel to the maxillary occlusal plane
- Mandibular projections: The patient’s head is tilted slightly backward to align the occlusal plane parallel to the floor.
- Film placement (general guidelines): The exposure side of the film is placed facing the teeth surface with the identification dot facing occlusal or incisal aspects.
- The film is placed vertically for anterior teeth and horizontally for posterior teeth.
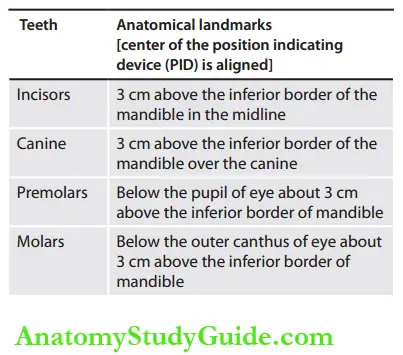
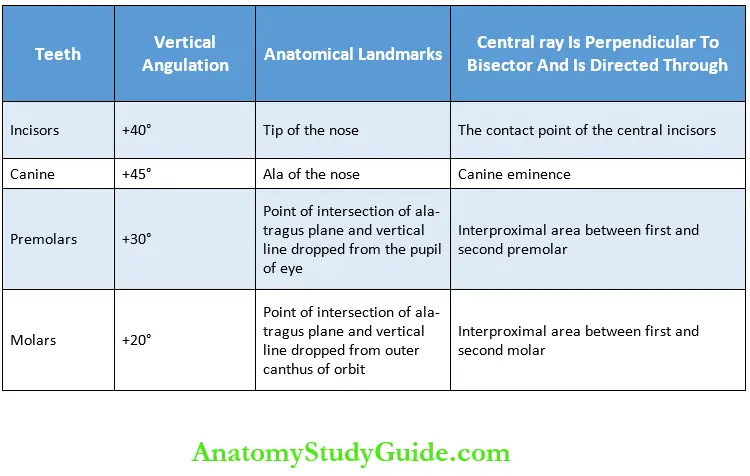
Position or Beam Indicating Device Placement (Pid or Bid):
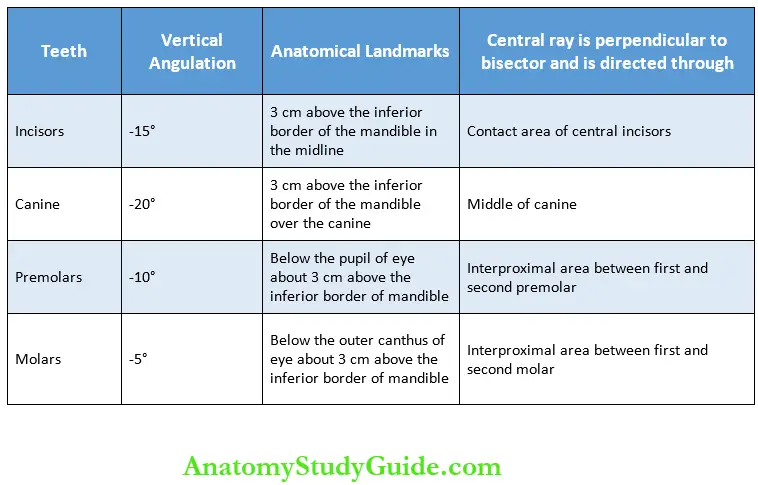
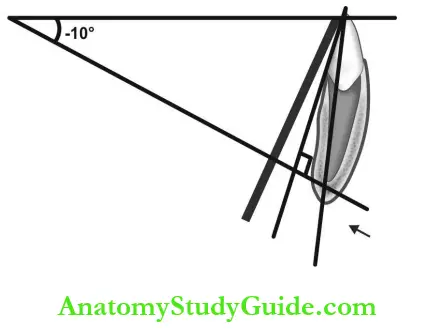
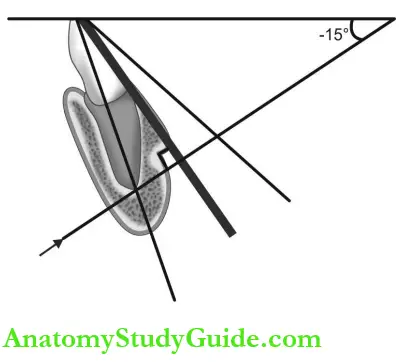
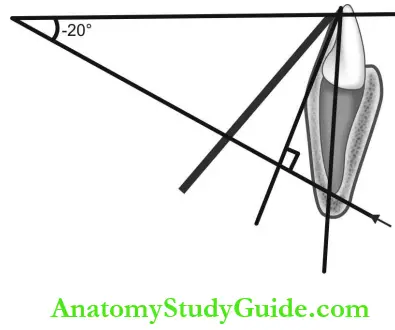
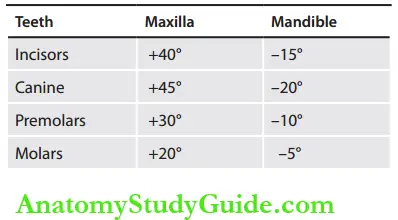
- In bisecting angle technique, vertical angulation is the angle that directs the central beam perpendicular to the imaginary bisector and is different for different teeth.
- Horizontal angulation is formed when the central beam is directed through the contact points of teeth to be examined, and it is usually at right angles to the buccal or facial surface of teeth in each region.
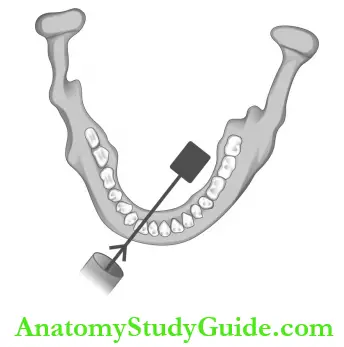
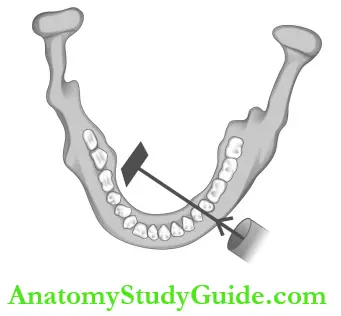
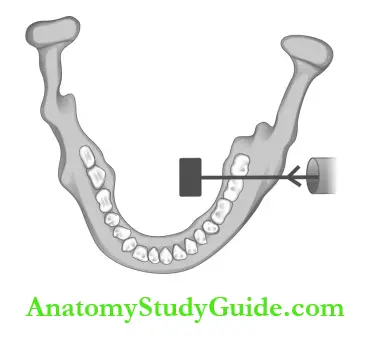
Maxillary Projections:
Mandibular Projections :
Bisecting Angle Technique Indications:
- To detect
- Pulpal, periapical and periodontal lesions.
- Dentoalveolar fracture.
- Impacted or unerupted teeth and supernumerary teeth.
- Dental anomalies like dens invaginatus, dentin dysplasia, ghost teeth, and structural alterations of teeth like amelogenesis, and dentinogenesis imperfecta.
- Some systemic diseases (loss of lamina dura in hyperparathyroidism, symmetric widening of PDL space in scleroderma)
- Dental age estimation in forensic odontology.
Bisecting Angle (Short Cone) Technique Advantages:
- The film holder is not essential.
- Radiation exposure is less due to the use of short PID.
Bisecting Angle (Short Cone) Technique Disadvantages: Image distortion and cone cut.
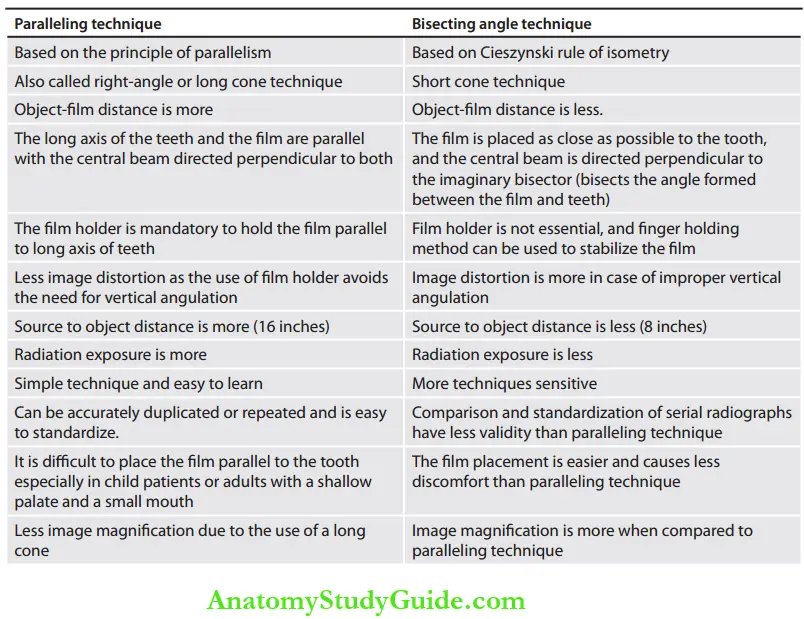
Question 3. Differences between paralleling and bisecting angle techniques.
(or)
Describe in detail the principle, technique, advantages, and disadvantages of the long cone and short cone technique.
Answer:
Question 4. Explain in detail the various projections in bitewing radiography.
Answer:
Bitewing Radiography: It is also called the interproximal technique used to examine the crowns of both maxillary and mandibular teeth, the interproximal areas, and crystal bone on the same radiograph.
Bitewing Film: An intra-oral periapical film with a bitewing tab attached becomes a bitewing film.
- Size 1: Intra-oral periapical film is used for anterior bitewing
- Size 2: Intraoral periapical film is commonly used
- Size 3: Intraoral periapical film is used when premolar and molar bitewing are taken in one film.
Bitewing Film Holder: Rinn XCP bitewing film holder with collimator is recommended.
Projections Premolar Bitewing Patient Preparation:
- Instructed to remove ornaments like nose studs
- The patient’s occlusal plane should be made parallel to the floor.
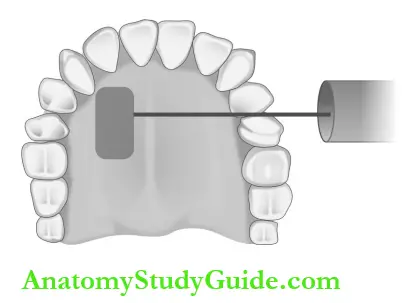
Projections Premolar Bitewing Patient Preparation Film Placement: The film is placed between the tongue and teeth, and the patient is instructed to bite on the tab with the anterior end of the film aligned to the middle of the mandibular canine, and the film is centered on the second premolar.
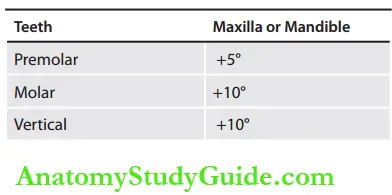
Projections Premolar Bitewing Patient Preparation Cone Placement:
- Middle of position indicating device at the level of the occlusal plane
- Vertical angulation: +5°
- Horizontal angulation: Central beam is the directed center of the film through the premolar contact areas.
Molar Bitewing Patient Preparation:
- Instructed to remove the ornaments
- The patient’s occlusal plane should be made parallel to the floor.
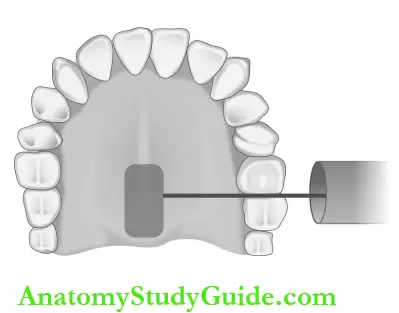
Molar Bitewing Patient Preparation Film Placement: The film is placed between the tongue and teeth and the patient is instructed to bite on the tab with the distal end of the film aligned 2 mm beyond the most posterior erupted molar.
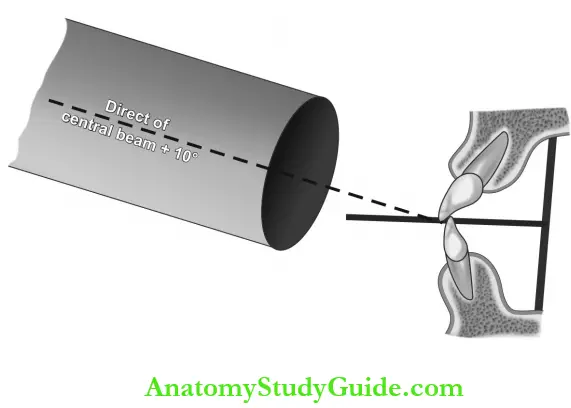
Molar Bitewing Patient Preparation Cone Placement:
- Middle of position indicating device at the level of the occlusal plane
- Vertical angulation: +10°
- Horizontal angulation: Central beam is the directed center of the film through the first and second molars below the lateral canthus of the eye at the level of the occlusal plane.
Vertical Bitewing:
- The long axis of the film is placed in a vertical direction
- The film is centered vertically.
- A longer bitewing tab is used, and the patient is instructed to bite such that the teeth meet the tab in the end-end position.
- Vertical angulation: +10°
- Horizontal angulation: Central beam is directed through the interproximal surfaces of the teeth.
- It is used mainly to assess bone loss in post-treatment cases.
Full Mouth Bitewing:
- In the case of anterior bitewing, a total of three projections are taken (two for canines on both sides and one for the incisor region).
- In the case of posteriors: One premolar and one molar projection for the right side. One premolar and one molar projection for the left side.
Indications of Bitewing Radiography:
- To detect proximal caries
- To detect secondary caries below restoration
- To identify the height of the alveolar crest
- To check the interproximal areas for calculus deposition.
Bitewing Radiography Advantages:
- Less radiation exposure when compared to full mouth intraoral periapical films (half the radiation exposure).
- Good perspective of alveolar bone crest than IOPA
- Bitewing radiography assures accurate assessment of changes in bone height.
Bitewing Radiography Disadvantage: Periapical lesions cannot be seen.
Question 5. Discuss in detail about occlusal radiography.
Answer:
Occlusal Radiography: Intraoral radiography is used to display large segments of the upper and lower dental arch which cannot be covered in periapical radiography.
Bitewing Radiography Occlusal Film:
- Film size: 5.7 x 7.6 cm or 3 x 2.3 inches.
- The white side of the film should be positioned towards the jaw to be examined between the occlusal surface of the maxillary and mandibular teeth.
- The film is stabilized by the patient biting the surface of the film.
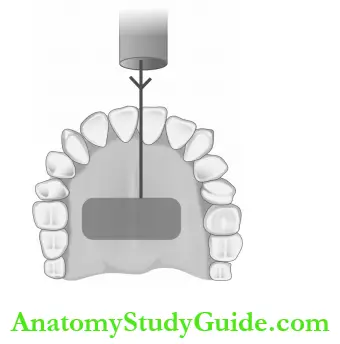
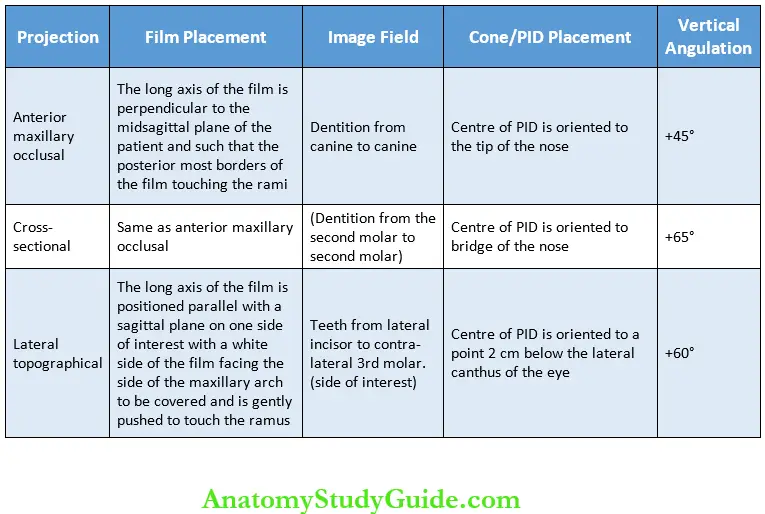
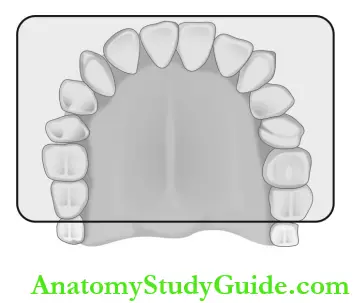
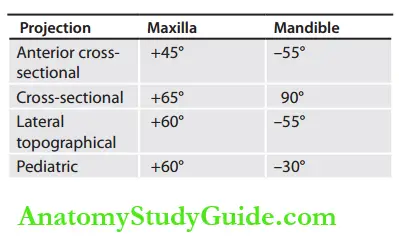
Maxillary Occlusal Projection:
- Patient preparation: The patient is positioned upright in the dental chair such that the occlusal plane is parallel to the floor and the midsagittal plane is perpendicular to the floor.
- Equipment preparation: 65 kVp, 10 mA, and 15 impulses are the exposure parameters, and 8 or 16 inches PID can be used.
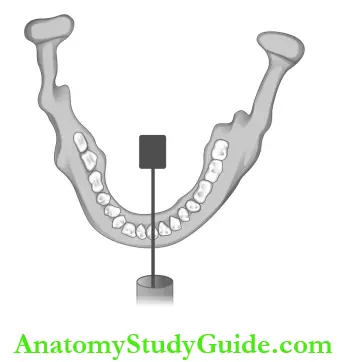
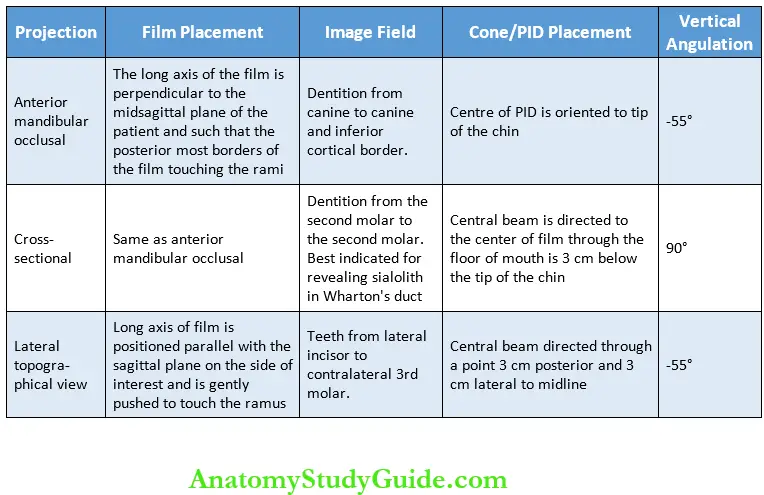
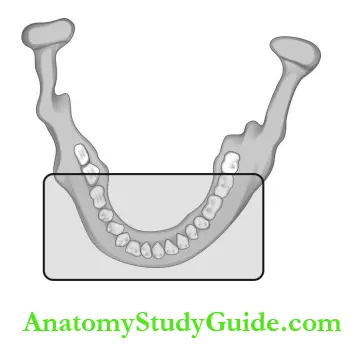
Mandibular Occlusal Projection:
- Patient preparation: The patient’s head is reclined and positioned such that the ala-tragus line is 45° above the horizontal and the occlusal plane is perpendicular to the floor.
- Equipment preparation: 65 kVp, 10 mA, and 15 impulses are the exposure parameters, and 8 or 16-inch PID is recommended.
Occlusal Projection Indications:
- To get a larger view than periapical radio-graphs as it includes a larger segment of the dental arch and in trismus cases where periapical radiograph cannot be taken.
- Used along with periapical radiography in Miller’s technique for object localization in three dimensions.
- To locate roots, supernumerary teeth, un-erupted and impacted teeth. Foreign bodies and calculus in ducts of submandibular and sublingual glands.
Evaluation of:
- Anterior, medial, and lateral outline of the maxillary sinus.
- Extent and displacement of fracture in the maxilla or mandible.
- The buccolingual extent of osteomyelitis, cysts, and malignancies of jaws
Intraoral Radiographic Techniques Short Notes
Question 1. Enumerate the various intraoral projections.
Answer:
- Periapical Radiography:
- Bisecting angle technique
- Paralleling technique
- Bitewing Radiography
- Premolar bitewing
- Molar bitewing
- Vertical bitewing (anterior)
- Occlusal Radiography Maxillary Projections
- Anterior maxillary cross-sectional
- Cross-sectional
- Lateral topographical view
- Mandibuar Projections
- Anterior mandibular cross-sectional
- Cross-sectional
- Lateral topographical view.
Question 2. Indications of periapical radiography.
Answer:
- To detect pulpal lesions (DC, fracture, attrition, abrasion, erosion, pulp calcification, and pulp stones).
- In endodontics (to determine pulp involvement and to determine root length in root canal treatment).
- To determine traumatic injuries in teeth and jaws (dentoalveolar fracture).
- To evaluate periapical lesions (apical periodontitis, periapical abscess, periapical granuloma, dental cyst, and radiopaque lesions like odontoma, condensing osteitis, etc.).
- To assess periodontal lesions (horizontal and vertical bone loss).
- To assess pericoronal lesions like dentigerous cysts.
- Age estimation: Intraoral periapical radio-graphs help in dental age and in personal identification in forensic odontology.
- To detect impacted or unerupted teeth and supernumerary teeth.
- To detect dental anomalies like dens in vagi- natus, dentin dysplasia, ghost teeth, etc.
- To determine structural alterations of teeth like amelogenesis-and dentinogenesis imperfecta.
- Intraoral periapical radiographs also help in revealing many hidden systemic diseases.
Periapical radiography Examples: Loss of lamina dura in hyperparathyroidism, and symmetric widening of PDL space in scleroderma.
Question 3. Indications of occlusal radiography.
Answer:
- To get a larger view than periapical radio-graphs as it includes a larger segment of the dental arch.
- Used along with periapical radiography in Miller’s technique for object localization in three dimensions.
- To locate roots, supernumerary teeth, unerupted and impacted teeth.
- To locate foreign bodies and calculus in ducts of submandibular and sublingual glands.
- Evaluation of anterior, medial, and lateral outlines of the maxillary sinus.
- In patients with trismus where periapical radiographs cannot be taken due to limited mouth opening.
- Evaluation of location, extent, and displacement of fracture in maxilla or mandible.
- Evaluation of the buccolingual extension of osteomyelitis, cysts, and malignancies of the jaws and their extent in the palate in case of the maxillary lesion and floor of the mouth in the mandibular lesion.
Question 4. Discuss pediatric intraoral radiography.
Answer:
General Considerations:
- Shallow palate and floor of the mouth in children cause difficulty in film placement.
- Children are apprehensive and can be allayed by familiarising the procedure by briefly explaining.
- Reduce the exposure parameters due to the small surface area of exposure.
- 10 years of age: 50% reduction in mA
- 10-15 years of age: 25% reduction in mA
- Lead aprons and fast films to ensure radia¬tion protection.
- Small size mouth can also result in increased incidence of gag reflex which can be managed by asking the child to breathe through the nose or by distracting their attention.
Intraoral Periapical Radiography:
- The principle technique is the same as adults.
- Pediatric precision or XCP film holder can be used.
3-6 Years of Age
- IOPA film Size: 0 is used
- The total number of IOPA taken for the full mouth survey is 4 (two in each maxilla and mandible).
Mixed Dentition: 7-12 years of age IOPA film size: 1 is used.
- Full mouth survey: Two incisors (one for maxilla and one for mandible)
- Four canine (right and left maxilla and right and left mandible)
- Four posteriors (right and left maxilla and right and left mandible)
- Total: 10.
Bitewing Radiography: Principles and techniques are the same as the adult procedure. Vertical angulation is +5-10° and horizontal angulation is through the interproximal surface.
3-6 Years of Age:
- IOPA film size: 0 with the paper loop is used.
- The total number of posterior bitewing taken for the full mouth survey is 2 (one on each side).
Mixed Dentition: 7-12 Years of Age
- Size 2 IOPA film is used with a bitewing tab attached.
- The total number of posterior bitewing is 2-4
Occlusal Radiography:
- The procedure is similar to adults except for the film size and exposure parameters.
- Exposure parameters: 65 kVp, 10 mA, 10 impulses or 90 kVp, 10 mA, three impulses are recommended.
- Size 2 IOPA film is used.
- The exposure side should face the jaw of interest with the patient biting the film in end-end bite relation.
- The long axis of the film should be posi¬tioned on side to side direction with the PID device directed to the middle of the film through the midline of the arch. For maxillary projection, the central beam is directed through the tip of the nose.
- For mandibular occlusal radiography, the patient is instructed to tip the head back so that the occlusal plane is 25° above the plane of the floor. The central beam is directed through the tip of the chin to the midline of the film.
Question 5. Discuss the vertical occlusal radiography.
Answer:
- Vertex occlusal projection: Plan view of tooth-bearing portion of maxilla from above.
- Vertical occlusal radiography Indication: Mainly used for assessment of the buccopalatal position of unerupted canine.
Vertical occlusal radiography Procedure:
- The patient is seated with the head supported, and the occlusal plane parallels to the floor.
- The film is placed such that the long axis of the film is placed anteroposteriorly and the patient is asked to bite on it.
- X-ray tube head is positioned above the patient’s head in the midline aiming downwards through the vertex of the skull such that the X-ray beam is directed down the long axis of the root canals of the upper incisors.
Vertical occlusal radiography Disadvantages:
- Long exposure time
- Radiation exposure to the eye.
- Superimposition of a shadow of the frontal bones may obscure the anterior part of the maxilla.
Question 6. Vertical angulation is used for various intraoral radiographic techniques.
Answer:
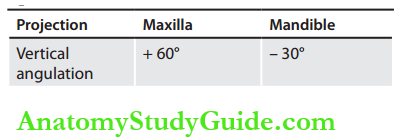
Vertical angulation in bisecting angle tech
Vertical Angulation in Occlusal Technique
Intraoral Radiographic Techniques Multiple Choice Questions
Question 1. Cieszynski’s principle of isometry is followed in.
- Bisecting angle technique
- Long cone technique
- Paralleling technique
- SLOB technique
Answer: 1. Bisecting angle technique
Question 2. The film is placed as close as possible to the lingual surface of the teeth in.
- Short cone technique
- Long cone technique
- Paralleling technique
- SLOB technique
Answer: 1. Short cone technique
Question 3. The imaginary bisector in the short cone technique forms the.
- Apex of triangle
- The longest side of the equal triangles
- The common base of the equal triangles
- The common side of the equal triangles
Answer: 4. Common side of the equal triangles
Question 4. A central beam perpendicular to the imaginary bisector forms the.
- Apex of triangle
- The longest side of the equal triangles
- The common base of the equal triangles
- The common side of the equal triangles
Answer: 3. Common base of the equal triangles
Question 5. The overlapping of tooth images at the inter-proximal spaces is caused due to.
- Improper film placement
- Patient movement
- Improper vertical angulation
- Improper horizontal angulation
Answer: 4. Improper horizontal angulation
Question 6. Elongation and foreshortening of images occur due to
- Improper film placement
- Patient movement
- Improper vertical angulation
- Improper horizontal angulation
Answer: 3. Improper vertical angulations
Question 7. The use of the film holding device, such as XCP along with a rectangular collimator helps in reducing patient exposure.
- Film placement
- Enhancing the object-film orientation
- Reducing the patient exposure
- Controlling the X-ray beam size
Answer: 3. Reducing the patient exposure
Question 8. Positioning of the tube head such that the central beam is directed downward from the hori¬zontal in the vertical plane is described as.
- Zero horihontal angulation
- Positive vertical angulation
- Negative vertical angulation
- Neutral zone
Answer: 2. Positive vertical angulation
Question 9. Positioning of the tube head such that the central beam is directed upward from the horizontal in the vertical plane is described as negative vertical angulation.
- Zero horihontal angulation
- Positive vertical angulation
- Negative vertical angulation
- Neutral zone
Answer: 3. Negative vertical angulation
Question 10. Maxillary distal oblique molar projection in periapical radiography is usually indicated for evaluation of.
- Maxillary sinus
- Zygomatic arch
- Impacted teeth
- Coronoid process
Answer: 3. Impacted teeth
Question 11. Central beam directed 3 cm above the exter¬nal maxillary notch on the inferior border of the mandible in mandibular distal oblique molar projection.
- Lateral topographic occlusal projection
- Mandibular distal oblique molar projection
- Postero-anterior mandible projection
- Vertex occlusal projection
Answer: 2. Mandibular distal oblique molar projection
Question 12. Proximal caries are best diagnosed with bite¬wing radiographs.
- Periapical radiographs
- Bitewing radiographs
- Orthopantomogram
- Occlusal radiographs
Answer: 2. Bitewing radiographs
Question 13. The use of a film holder in the bitewing technique reduces the incidence of.
- Cone-cut images
- Film fog
- Unwanted patient exposure
- Image noise
Answer: 1. Cone-cut images
Question 14. Intraoral technique in which both maxillary and mandibular teeth are seen is.
- Vertical occlusal radiograph
- Cross-sectional occlusal radiograph
- Bitewing radiograph
- Orthopantamograph
Answer: 3. Bitewing radiograph
Question 15. The following IOPA size film is recommended for bitewing projection of both premolar and molar in one film is.
- Size 2
- Size 3
- Size 4
- Size 5
Answer: 2. Size 3
Question 16. In pediatric bitewing projection to cover both the premolar and molar of each side the following film size is recommended.
- Size 2
- Size 3
- Size 4
- Size 5
Answer: 1. Size 2
Question 17. Which of the following radiographic techniques is indicated to evaluate the bucco- lingual extent of a lesion in the jaw is bone?
- Occlusal radiography
- Orthopantomography
- Bitewing radiography
- Lateral oblique view
Answer: 1. Occlusal radiography
Question 18. Which mandibular occlusal projection is best indicated to detect stones in the duct of the submandibular gland is.
- Horizontal view
- Cross-sectional view
- Paralleling view
- Lateral view
Answer: 2. Cross-sectional view
Question 19. The intraoral radiographic technique best indicated in the case of trismus is.
- Paralleling technique periapical view
- Bitewing view
- Occlusal view
- Bisecting angle technique periapical view
Answer: 3. Occlusal view
Question 20. The exposure required for edentulous patients is approximate.
- 50% more than the dentulous ridge
- 50% less than the dentulous ridge
- 25% more than the dentulous ridge
- 25% less than the dentulous ridge
Answer: 4. 25% less than the dentulous ridge
Question 21. The total number of films required for a full mouth survey of edentulous patients is.
- 8
- 14
- 10
- 16
Answer: 2. 14
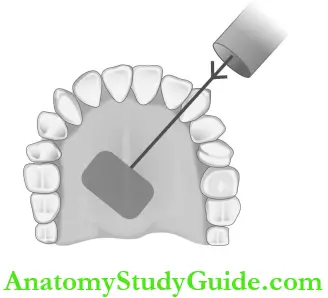
Question 22. In which occlusal projection zygomatic process of maxilla superimposes over the tooth of molar teeth in lateral maxillary occlusal.
- Cross-sectional maxillary occlusal
- Lateral maxillary occlusal
- Cross-sectional mandibular occlusal
- Lateral mandibular occlusal
Answer: 2. Lateral maxillary occlusal
Intraoral Radiographic Techniques Viva Voce
Question 1. Indications of bitewing radiography.
Answer:
- To detect proximal caries
- To detect secondary caries below restoration
- To detect the height of the alveolar crest
- To detect calculus deposits in interproximal areas.
Question 2. Advantages of bisecting angle technique.
Answer:
- The film holder is not essential.
- Less radiation exposure due to the use of a short cone.
- Film placement is simple and comfortable for the patients.
Question 3. What is vertical angulation in periapical radiography?
Answer:
- In bisecting angle technique, the central beam is directed perpendicular to the imaginary bisector (bisects the angle formed between the film and teeth).
- It is the angle formed between the central beam passing through the apex of teeth with that of the occlusal plane.
- The vertical angulation is the angle that directs the central beam perpendicular to the imaginary bisector and is different for different teeth.
- It is positive for the maxilla and negative for the mandible.
Question 4. What is horizontal angulation in periapi¬cal radiography?
Answer:
- Horizontal angulation is formed when the central beam is directed through the contact points of the teeth to be examined.
- It is usually at right angles to the buccal or facial surface of teeth in each region.
Question 5. Enumerate the film holders used in the paralleling technique.
Answer:
- Extension cone paralleling (XCP) instru¬ments.
- Precision rectangular collimating device.
- Snap-A-ray intraoral film holder.
- Hemostat and rubber bite blocks.
- Stabe disposable film holder.
Question 6. Reason for less image magnification and increase definition in paralleling technique.
Answer:
- Long source-object distance with a reduc¬tion in the size of the apparent focal spot.
- The central beam is directed perpendicular to both the film and the tooth.
Question 7. Disadvantages of the finger-holding method of film placement in bisecting angle technique.
Answer:
- Radiation exposure to the patient’s finger.
- Overbending of the film is due to the excessive force exerted by some patients to stabilize the film.
- The film may slip without the patient’s knowledge resulting in an improper image field.
- Increased incidence of a cone-cut as there is a possibility for the misalignment of the cone to that of the film in the absence of an external guide.
Question 8. Special considerations to avoid gag reflexes during intraoral radiography.
Answer:
- Ask the patient to breathe through the nose.
- Deviate the attention of the patient as when their concentration is not about the procedure as it helps in reducing the gag reflex.
- Avoid film placement such that the borders touch the soft palate as it may trigger the gag reflex.
- Instruct the patient that during film placement the tongue should be relaxed and positioned well to the floor of the mouth.
- In extreme cases, topical anesthetic mouth-washes/sprays can be used to produce temporary numbness of the tongue and palate.
Question 9. Special consideration for stabilizing the film in edentulous patients.
Answer:
- The placement of film becomes complicated due to its tipping into the voids due to missing teeth.
- Cotton rolls are placed between the ridge and the film holder to support the film holder and prevent its tipping.
Question 10. Special considerations for periapical radiography in endodontic practice.
Answer:
Problems faced in endodontic practice: Film placement is difficult due to the presence of rubber dams and clamps.
- Root canal assessment becomes problematic in distorted images like foreshortened and elongated images.
- Identification and separation of root canals in multirooted teeth becomes difficult.
Possible remedies:
- Tapping the intraoral film packet to one end of a wooden tongue spatula is held in place by the patient.
- Specialized endodontic film holder like endoray (a small basket is present in the bite platform area to accommodate the handles of all endodontic instruments while still maintaining parallelism between the teeth and film).
Intraoral Radiographic Techniques Highlights
- Dental radiographs demand adequate information for accurate diagnosis. Film-based radiographic images require the use of particular techniques and precautions to maximize the diagnostic and interpretative value of the radiograph.
- Minimizing the patient’s exposure to radiation and obtaining high-quality radiographs depends on applying precise techniques in film placement, central ray angulation, maintaining the film- object-central beam orientation, exposure parameters, and film processing.
Leave a Reply