Liver and Gallbladder
Question 1. Write laboratory diagnosis of hepatitis B.
Answer:
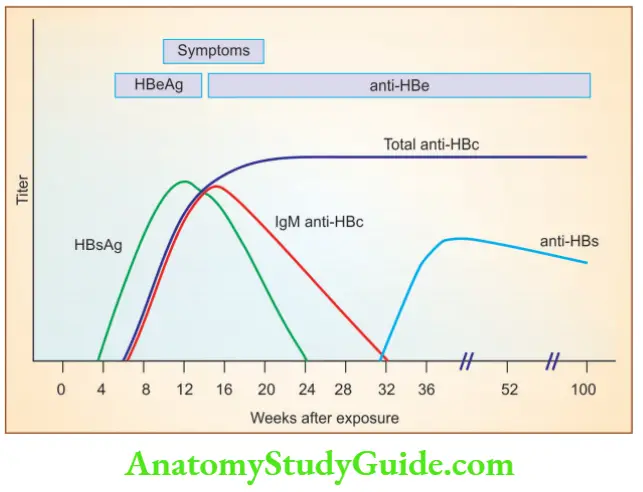
The natural course of hepatitis B
- HBsAg appears before the onset of symptoms and declines to undetectable levels in 12 weeks
- HBeAg, HBV-DNA, and DNA polymerase appear in the serum soon after HBsAg, and all signify active viral replication
- Anti-HBs antibody titers rise as the titers of HBsAg fall
- Anti-HBs may persist for life and is the basis for current vaccination strategies using noninfectious HBsAg
- Persistence of HBeAg is an important indicator of continued viral replication
- IgM anti-HBc antibody becomes detectable in the serum shortly before the onset of symptoms, which is replaced by IgG anti-HBc over a period of months
Read and Learn More Preparatory Manual of Pathology Question and Answers
Question 2. Write a note on CVC liver.
Answer:
Passive congestion and centrilobular necrosis
Right-sided cardiac failure
- This leads to passive congestion of the liver
- The liver is slightly enlarged, tense, and cyanotic
- Microscopically: Congestion of centrilobular sinusoids
Left-sided cardiac failure
- This leads to hepatic hypoperfusion and hypoxia
- Centrilobular necrosis is ischemic coagulative necrosis of hepatocytes in the central region of the lobule (around the central vein)
Centrilobular hemorrhagic necrosis (nutmeg liver)
- Due to a combination of hypo perfusion and retrograde congestion of the liver
- The liver takes on a variegated mottled appearance and resembles a nutmeg, hence named “nutmeg liver”
Question 3. Write a note on cirrhosis of the liver.
Answer:
Cirrhosis
- A condition marked by the diffuse transformation of the entire liver into regenerative parenchymal nodules surrounded by fibrous bands and variable degrees of vascular shunting
How is cirrhosis brought about?
- Cytokines and chemokines that play a role in cirrhosis of the liver include:
-
- Platelet-derived growth factor receptor β (PDGFR-β) results in the proliferation and activation of hepatic stellate cells into myofibroblasts
- Transforming growth factor β (TGF-β), results in the fibrogenic property of stellate cells
- Endothelin-1 (ET-1) results in the contraction of myofibroblasts
Microscopic feature of cirrhosis
- Thick bands of collagen separate rounded cirrhotic nodules
Clinical Features:
- Jaundice, encephalopathy, coagulopathy
- Pruritus (in patients with chronic jaundice)
- Palmar erythema and spider angiomas of the skin: Due to impaired estrogen metabolism and hyperestrogenemia in male patients with chronic liver failure
- Hypogonadism and gynecomastia in males due to hyperestrogenemia
Question 4. Write morphological features of chronic viral hepatitis.
Answer:
Chronic hepatitis
- Defined as symptomatic, biochemical, or serological evidence of continuing or relapsing hepatic disease for more than 6 months
Microscopy
- A characteristic feature is mononuclear inflammatory cell infiltrate around the portal tract
- Interface hepatitis: Inflammatory infiltrate is seen at the interface between the hepatocytes and portal tract
- The hallmark of progressive chronic liver damage is “scarring”
- With scarring, there is increased ductular reaction (increase in the number of bile ductules)
Chronic hepatitis B
- The diagnostic hallmark is the presence of “Ground-glass” hepatocytes, hepatocytes with endoplasmic reticulum swollen with HBsAg
Chronic hepatitis C
- Shows lymphoid aggregates or fully formed lymphoid follicles
- Fatty change of scattered hepatocytes
Question 5. Discuss in detail the etiopathogenesis and morphology of alcoholic liver disease.
Answer:
Three forms of alcoholic liver injury
- Hepatocellular steatosis or fatty change
- Alcoholic (or state-) hepatitis
- Steato-fibrosis, including cirrhosis in the late stages of the disease
Pathogenesis
1. Hepatocellular steatosis
- Increased generation of NADPH (lipid biosynthesis) by alcohol dehydrogenase and acetaldehyde dehydrogenase, resulting in impaired lipoprotein synthesis
2. Alcoholic hepatitis
- Alcohol ingestion leads to the production of reactive oxygen species (ROS) due to increased cytochrome P-450 metabolism
3. Steatofibrosis
- Alcohol stimulates endothelin release from endothelial cells, resulting in vasoconstriction and contraction of activated stellate cells
Morphology
1. Hepatic Steatosis (Fatty Liver)
- Grossly: Enlarged liver, can weigh as heavy as 4 to 6 kg, appears to be yellow and greasy
- Microscopy: Lipid droplets accumulate in hepatocytes, begin as small droplets that coalesce into large droplets and push the nucleus aside
2. Alcoholic (state) hepatitis
- Hepatocyte swelling and necrosis
- Mallory-Denk bodies: Eosinophilic material in hepatocytes, made up of tangled skins of intermediate filaments such as keratins 8 and 18 in complex with ubiquitin
- Neutrophilic infiltration of hepatocytes
3. Alcoholic steatofibrosis
- Occurs due to prominent activation of sinusoidal stellate cells and portal fibroblasts, with resultant fibrosis
- Chicken wire fence pattern: Scarring starts around the sinusoidal hepatocytes and spreads outward, encircling individual or small clusters of hepatocytes
- End-stage alcoholic liver disease is termed micro-nodular or Laënnec cirrhosis
Question 6. Discuss the pathogenesis and morphology of hemochromatosis.
Ans.
Hemochromatosis
- Caused by excessive iron absorption, which gets deposited in the liver and pancreas, heart, joints, and endocrine organs
- Total body iron pool ranges from 2 to 6 gm in normal adults; about 0.5 gm is stored in the liver
- In most severe forms of hemochromatosis, total iron accumulation may exceed 50 gm, more than one-third of which accumulates in the liver
Leads to
- Micronodular cirrhosis in all patients
- Diabetes mellitus
- Abnormal skin pigmentation
Pathogenesis
- The disease manifests when more than 20 gm of iron has accumulated
- Hepcidin secreted by the liver is the main regulator of iron absorption
- Hepcidin lowers plasma iron levels and its deficiency leads to iron overload
- An adult form of hemochromatosis is caused by mutations of the HFE gene, located on the short arm of chromosome 6
Morphology
- Deposition of hemosiderin occurs in (decreasing order of severity) the liver, pancreas, myocardium, pituitary gland, adrenal gland, thyroid, and parathyroid glands, joints, and skin
- . Cirrhosis
- Pancreatic fibrosis
Hematoxylin and eosin stain
- Iron becomes evident as golden-yellow hemosiderin granules in the cytoplasm of periportal hepatocytes
Prussian blue
- Gives blue color to hemosiderin-containing hepatocytes
Question 7. Write a note on the α1-antitrypsin deficiency.
Answer:
α1-Antitrypsin deficiency
- Autosomal recessive disorder of hepatocellular accumulation of misfolded proteins due to low levels of circulating α1-antitrypsin (α1-AT)
- α1-AT: Inhibits proteases, neutrophil elastase, cathepsin G, and proteinase 3, which are released from neutrophils at sites of inflammation
- α1-AT deficiency leads to the development of pulmonary emphysema (due to the increased proteases)
- α1-AT gene is located on chromosome 14 and has different genotypes
- PiMM is the most common genotype, seen in 90% of individuals
- The most common clinically significant mutation is PiZZ
- Homozygotes for PiZZ protein have circulating α1-AT levels that are only 10% of normal
- Mutant polypeptide α1-AT-Z is abnormally folded and polymerized, triggering an unfolded protein response, that may lead to apoptosis
- Also, there occurs an accumulation of misfolded proteins in the liver
- All individuals with the PiZZ genotype accumulate α1-AT-Z in the endoplasmic reticulum of hepatocytes
- Hepatocellular carcinoma develops in 2% to 3% of PiZZ adults
- α1-AT deficiency is the most commonly diagnosed inherited hepatic disorder in infants and children
Morphology
- The presence of round to oval cytoplasmic globular inclusions in the hepatocytes, which are strongly periodic acid–Schiff (PAS) positive and diastase-resistant
- Electron microscopy: Endoplasmic reticulum dilated by aggregates of misfolded proteins
Question 8. Write a note on hyperbilirubinemia.
Answer:
Causes of increased bilirubin levels
Unconjugated bilirubin
- Is insoluble in water and exists in complexes with serum albumin
- Hemolytic disease of the newborn (erythroblastosis fetalis) may lead to the accumulation of unconjugated bilirubin in the brain, which results in severe neurologic damage, referred to as kernicterus
Causes of unconjugated hyperbilirubinemia
1. Excess production of bilirubin
- Hemolytic anemia, resorption of blood from internal hemorrhage, ineffective erythropoiesis (for example pernicious anemia, thalassemia)
2. Impaired bilirubin conjugation
- Physiologic jaundice of the newborn (decreased UGT1A1 activity, decreased excretion)
- Genetic deficiency of UGT1A1 activity (Crigler-Najjar syndrome types I and II)
- Gilbert syndrome
- Diffuse hepatocellular disease (for example viral or drug-induced hepatitis, cirrhosis)
Conjugated bilirubin
- Is water-soluble, nontoxic, and can be excreted in urine
- Serum bilirubin levels in the normal adults vary between 0.3 and 1.2 mg/dl
- Jaundice becomes evident when serum bilirubin levels rise above 2 to 2.5 mg/dl
Causes
- Dubin-Johnson syndrome, rotor syndrome
Question 9. Write a note on cholestasis.
Answer:
Cholestasis
- Caused by impaired bile formation and bile flow with resultant accumulation of bile pigment in the hepatic parenchyma
- Caused by extrahepatic or intrahepatic obstruction of bile channels
Clinical and laboratory features
- Patients may have jaundice, pruritus, skin xanthomas (focal accumulation of cholesterol)
- Nutritional deficiencies of fat-soluble vitamins A, E, D, or K
- Characteristic laboratory finding is elevated serum alkaline phosphatase and γ-glutamyl transpeptidase (GGT), enzymes present on the apical (canalicular) membranes of hepatocytes and bile duct epithelial cells
Morphology
- Accumulation of bile pigment within the hepatocytes is seen
- Elongated green-brown plugs of bile are visible in dilated bile canaliculi
- Rupture of canaliculi leads to extravasation of bile, which is phagocytosed by Kupffer cells
- Droplets of bile pigment accumulate within the hepatocytes, which now appear fine and foamy, called “feathery degeneration”
Question 10. Write a note on primary biliary cirrhosis.
Answer:
Primary biliary cirrhosis (PBC)
- Autoimmune inflammatory disease with F: M ratio in excess of 6: 1
- Clinical features fatigue, pruritus, hepatomegaly, eyelid xanthelasmas, hyperpigmentation, inflammatory arthropathy, and cirrhosis in chronic cases
- Anti-mitochondrial antibodies are present in 90% to 95% of patients
- Elevated levels of alkaline phosphatase and γ-glutamyltransferase are seen
- Increased risk of developing hepatocellular carcinoma
Extrahepatic manifestations
- Sjögren syndrome, systemic sclerosis, thyroiditis, rheumatoid arthritis, Raynaud phenomenon, membranous glomerulonephritis, and celiac disease
Question 11. Classify hepatocellular adenomas.
Answer:
Hepatocellular adenomas
Risk factors: Oral contraceptives and anabolic steroids
Pathogenesis: 3 subtypes:
1. HNF1-α inactivated hepatocellular adenomas
- Most commonly found in women
- No risk of malignant transformation
- Inactivating mutations of HNF1-α are most commonly seen
2. β-Catenin activated hepatocellular adenomas
- High risk for malignant transformation
- Associated with oral contraceptive and anabolic steroid use
- Activating mutations of α-catenin are seen
3. Inflammatory hepatocellular adenomas
- Associated with non-alcoholic fatty liver disease (NAFLD)
- IL-6 mediates JAK-STAT signaling and leads to overexpression of acute phase reactants (C-reactive protein and serum amyloid A)
- Definitive risk for malignant transformation
Question 12. Enumerate the precursor lesions of hepatocellular carcinoma. Discuss etiopathogenesis and morphology of hepatocellular carcinoma.
Answer:
Precursor lesions of hepatocellular carcinoma
1. Cellular dysplasia (small cell change and large cell change)
- Seen in chronic liver disease
2. Low-grade and high-grade dysplastic nodules
Seen in cirrhosiS
Etiopathogenesis
1. Risk factors
- Viral infections (HBV, HCV) and toxic injuries (aflatoxin, alcohol)
- Hereditary hemochromatosis, α1-AT deficiency, Wilson disease, and metabolic syndrome (associated with obesity, diabetes mellitus, and nonalcoholic fatty liver disease)
2. Molecular changes seen in hepatocellular carcinoma
- β-catenin activation
- p53 inactivation
- IL-6/JAK/STAT signal pathway activation
Morphology
Gross
- Can be a unifocal or multifocal mass, varying-size nodules, or a diffusely infiltrative cancer
Microscopy
- Well-differentiated to highly anaplastic lesions
- Well-differentiated HCCs have cells resembling normal hepatocytes but with thickened trabecular structures or pseudo-glandular structures
Question 13. Write a note on cholangiocarcinoma.
Answer:
Cholangiocarcinoma
- Malignancy of the biliary tree, arising from bile ducts within and outside of the liver
- Risk factors
- Infestation by liver flukes (Opisthorchis and Clonorchis species)
- Chronic inflammatory disease of large bile ducts—example
- . primary sclerosing cholangitis
- Hepatitis B and C, and non-alcoholic fatty liver disease
Sites
- Can be intrahepatic or extrahepatic
- Klatskin tumors/extrahepatic tumors (perihilar) are located at the junction of the right and left hepatic ducts
Gross
- Extrahepatic cholangiocarcinoma appears as firm, gray nodules within the bile duct wall
- Intrahepatic cholangiocarcinoma occurs in the noncirrhotic liver
Microscopy
- Are typical adenocarcinomas and produce mucin
- Well to moderately differentiated with clearly defined glandular/tubular structures lined by malignant epithelial cells
Desmoplastic stromal response, lymphovascular and perineural invasion are common
Question 14. Write a note on the risk factors and pathological effects of gallstones.
Answer:
Two types of gallstones
- Cholesterol stones: Composed of cholesterol monohydrate
- Pigment stones: Composed predominantly of bilirubin calcium salts
Risk factors
1. Cholesterol stones
- 2Female sex hormones: Female gender, oral contraceptives, pregnancy
- Obesity and metabolic syndrome
- Rapid weight reduction
- Gallbladder stasis
- Hyperlipidemia syndromes
2. Pigment stones:
- Chronic hemolytic syndromes
- Biliary infection
- Gastrointestinal disorders: Ileal disease (for example Crohn’s disease), ileal resection or bypass, cystic fibrosis
Pathogenesis
- Conditions that lead to the formation of cholesterol gallstones
- Supersaturation of bile with cholesterol
- Hypomotility of the gallbladder
- Hypersecretion of mucus in the gallbladder
Conditions that lead to the formation of pigment stones (increased unconjugated bilirubin in bile):
- Chronic hemolytic anemia
- Severe ileal dysfunction
- Infection of the biliary tract with Escherichia coli, Ascaris lumbricoides or the liver fluke, Clonorchis sinensis
Leave a Reply