Management of Medically Compromised Children Introduction
Children with an underlying chronic medical illness need special attention during dental therapy.
Table of Contents
The reasons for the requirement for this special attention are as follows:
1. Monitoring vital systems: A medical illness may compromise vital systems that need appropriate attention during dental therapy, for example, cardiac abnormalities such as ventricular septal defect, auricular septal defect and valvular lesions.
Read And Learn More: Paediatric Dentistry Notes
2. Drug dosage modification: Chronic medication for the underlying disease may require dosage modification by the physician.
For instance, children on oral steroids have decreased stress tolerance.
Hence, the steroid dose has to be doubled during dental treatment visits.
3. Drug contraindication: Certain medical conditions may contraindicate the routine drugs used during/after dental treatment.
For example, adrenaline in local anaesthetic is contraindicated in children with hyperthyroidism.
As thyroxin sensitises the myocardium to catecholamines (such as adrenaline), the heart rate increases with a bizarre rhythm causing arrhythmia.
NSAIDs have to be safely prescribed in children with renal failure.
4. Specific behaviour management: A medical illness may be associated with decreased intellectual maturity or IQ.
The behaviour management of such children needs special attention during the procedure.
For example, a hypothyroid child may have a low IQ.
5. Dental treatment contraindication: Dental therapy may be contraindicated in certain medical conditions.
Abnormally high glucose levels in juvenile diabetes and a decrease in platelet count in leukaemic children are examples of such conditions.
6. Pre-medication: Certain illnesses require pretreatment medication to allow safety during dental procedures.
Antibiotic prophylaxis is required against infective endocarditis in children with cardiac abnormalities.
Factor VIII concentrate infusion is a must in haemophiliacs before starting dental procedures.
Caution while performing oral procedures:
Procedures such as extraction have to be performed cautiously in certain medically compromised
children.
Oral prophylaxis in children with gingival leukaemic infiltrates and primary molar extraction in haemophiliac children are some examples.
All medical conditions require pre-treatment assessment by the consulting physician of the child.
The physician’s consent on the child’s fitness to undergo the procedure, the precautionary measures and the medications to be avoided or sought have to be recorded and followed meticulously.
This will make the dental treatment strategically, morally and ethically correct.
The medical conditions that give the status of special attention to a suffering child are as follows:
- Cardiac abnormalities
- Bleeding disorders
- Diabetes mellitus
- Leukaemia
- Neurological disorders
- Respiratory diseases
- Endocrine disorders
- Renal disease
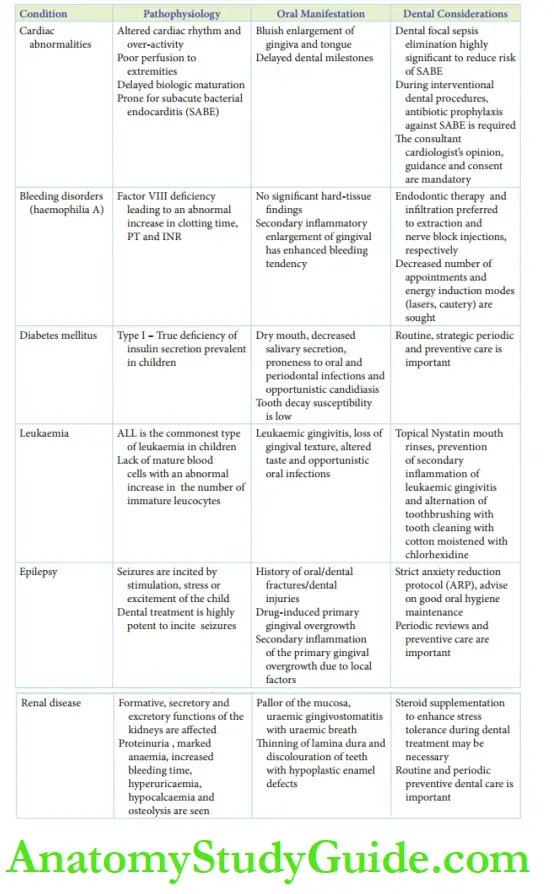
The oral manifestations and points of special mention during the dental treatment of the listed conditions.
Cardiac Abnormalities
The common congenital cardiac abnormalities encountered are ventricular septal defect (VSD), atrial septal defect (ASD), valvular stenosis, valvular regurgitation (mitral valve and tricuspid valve) and mitral valve prolapse.
The less common cardiac abnormalities are patent ductus arteriosus, tetralogy of Fallot and transposition of vessels.
Apart from these congenital cardiac abnormalities, valvular stenosis and regurgitation may be acquired following acute rheumatic fever.
Generally, children manifest increased heart rate, increased low-volume pulse rate, altered cardiac rhythm and hypertrophy of the myocardium.
The anatomic defect of the heart leads to inefficient blood circulation and increased myocardial activity.
The circulation is not efficient enough to perfuse to the extremities leading to stagnation of deoxygenated blood in the extremities.
Cyanosis is seen in the extremities such as lips, fingers and toes.
Due to increased muscular contractile activity of the heart, children do not gain body weight.
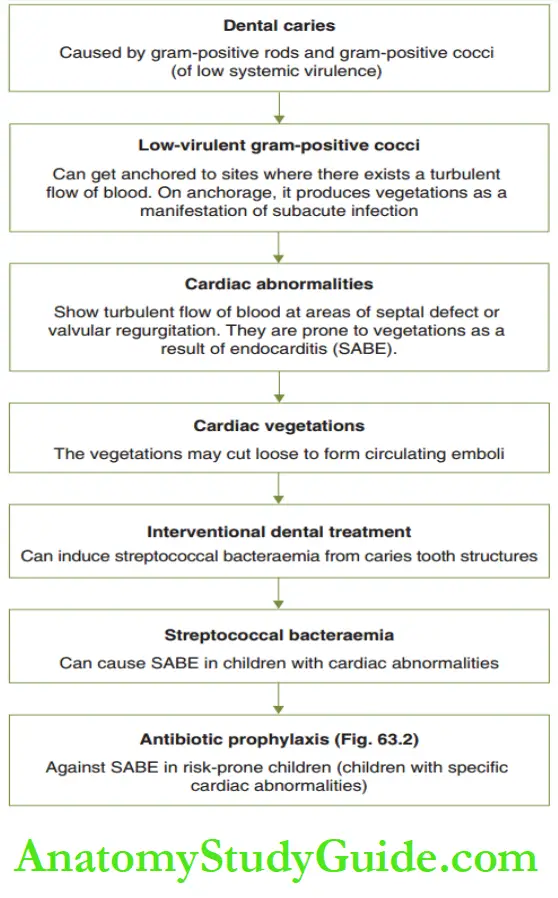
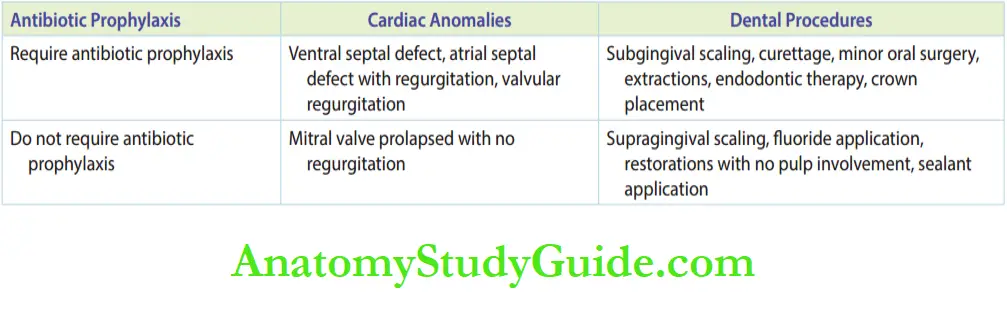
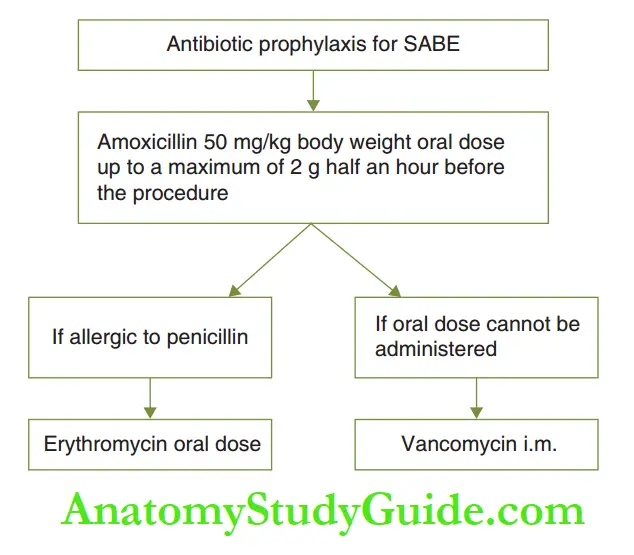
The antibiotic prophylaxis indications and the drugs used are respectively.
While treating dental foci, the objective is to eliminate the dental infection in toto.
It implies the fact that if endodontic therapy of a pulpal-involved molar cannot be successfully carried out, then extraction is preferred.
Any treatment should be carried out on the basis of guidance/communication with the cardiologist of the child.
The anxiety reduction protocol is highly significant as anxiety increases the heart rate further.
Sedation or general anaesthesia may be employed when comprehensive dental care is required in anxious children.
Bleeding Disorders
The bleeding disorders that are most common in children are haemophilia A and thrombocytopenia.
Von Willebrand disease, parahaemophilia, factor deficiency and other minor coagulopathies are less common.
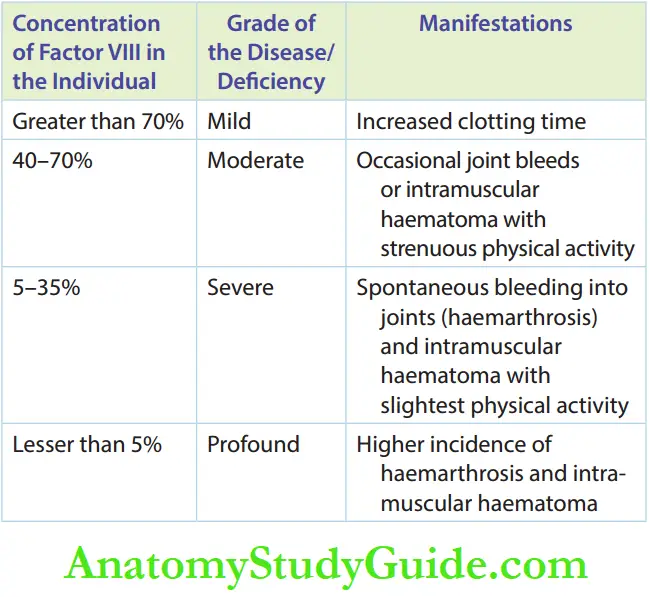
Haemophilia A is the deficiency factor VIII (antihaemophilic factor).
Its concentration in a normal adult is 95–100%. Deficiency of the factor implies that its concentration is decreased to a range of 0–95%.
The severity of the disease and its manifestations. The abnormal increase in clotting time is a significant point that demands special attention during dental treatment.
Oral Manifestations:
Children suffering from bleeding disorders manifest no significant findings on teeth.
Occasional hypoplastic spots and enhanced decay susceptibility due to poor oral hygiene may be observed.
The gingival enlargement, present due to poor oral hygiene, may demonstrate a spontaneous bleeding tendency.
Ecchymoses may be evident in the oral mucosal tissues. It requires no intervention.
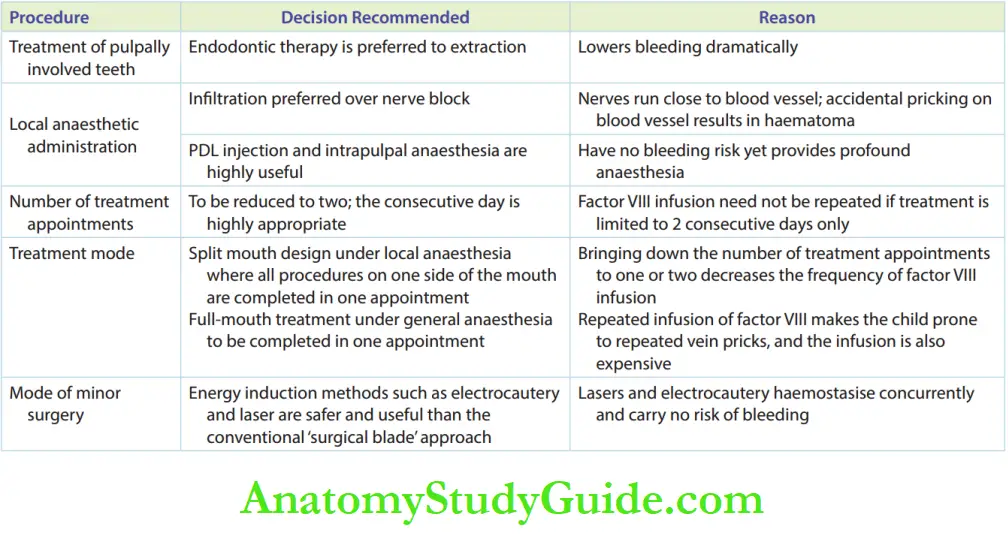
Dental Treatment Considerations:
Apart from referral to a physician for obtaining fitness, a primary blood investigation is necessary to assess the international normal range (INR), prothrombin time (PT) and activated partial thromboplastin time (a-PTT).
The values of these investigations give a clear picture of finalising the treatment plan.
All dental treatments have to be carried out after pre-treatment factor VIII infusion upon the guidance of the treating physician.
Some intraoral procedures can be amended as per the haemophiliac patient.

Diabetes Mellitus
Type I or insulin-dependent diabetes mellitus is seen in children.
It is also referred to as juvenile diabetes. There is a deficiency in the secretion of insulin by the beta islets of Langerhans of the pancreas.
The therapy constitutes parenteral insulin. Affected children will have polyuria, polydipsia and polyphagia when the disease is left untreated.
Th risk ofdiabetic ketoacidosis is higher.
Oral Manifestations:
Children will have dry mouths and decreased salivary secretion when the systemic condition is untreated.
They are more prone to oral soft tissue infections, opportunistic candidiasis, burning mouth and signs of periodontal degeneration.
Tooth decay susceptibility is decreased due to diet restriction on sugar intake.
Dental Treatment Considerations:
Maintenance of the systemic condition and oral health is primarily important to avoid dental complications.
Routine oral prophylaxis, assessment of periodontal condition, reinforcement of oral hygiene instructions at every visit and periodic review form the protocol of dental management in these children.
Leukaemia
Leukaemia is a hematologic disorder with an abnormally high number of leucocytes with the presence of immature precursor cells of the myeloid hematopoietic series.
It is associated with a concomitant decrease in the number of erythrocytes and platelets.
Acute lymphocytic leukaemia (ALL) is the most common type of leukaemia in children.
The children have signs of anaemia, increased risk of acute bacterial infections as well as bleeding disorders in lieu of a decrease in the effective number of mature blood cells.
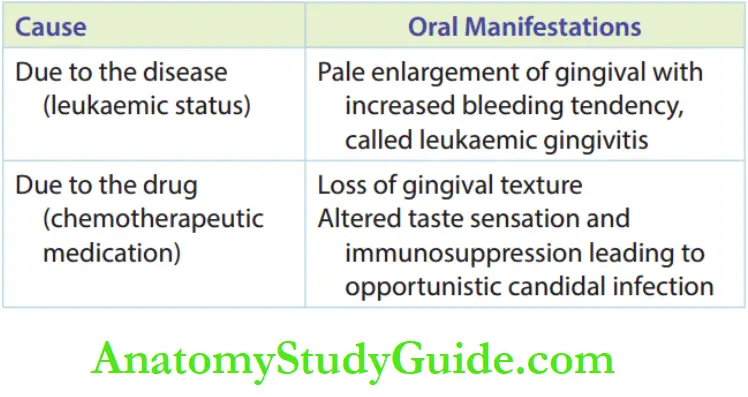
Oral Manifestation:
Leukaemia-infected children have oral manifestations either due to systemic alteration or chemotherapeutic medication prescribed for the disease.
Dental Treatment Consideration:
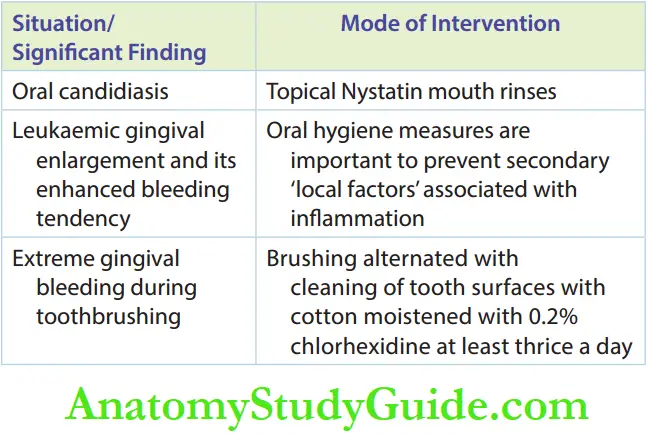
Dental treatment is carried out only when the child is in a controlled leukaemic status.
A physician’s guidance and consent are mandatory. Specific modes of intervention of oral leukaemic manifestations.
Neurological Disorders
Convulsive disorders (epilepsy) are the most common neurological disorders encountered in children.
They may vary in degree and presentation.
Convulsions are incited when the children are stressed, anxious or excited.
Dental treatment includes a variety of stimuli that can disturb and excite children. Thse may precipitate convulsions.
Children are under chronic medication with anticonvulsants for such conditions.
Anti-convulsant drugs such as phenytoin and sodium valproate promote gingival enlargement.
Oral Manifestations:
Children may manifest a history of oral/facial/dental fractures due to a fall/injury during a seizure episode.
Other dental injuries such as luxation and avulsion may also be demonstrated.
Laceration injuries (healed with scarring) of the lip and tongue may also be manifested due to persistent biting of lips/tongue during a seizure episode.
Drug-induced gingival overgrowth involving the attached gingival and interdental papilla leads to the formation of pseudo-pockets.
This leads to decreased clinical crown height and sometimes causes complete submergence of teeth by gingival overgrowth.
When this overgrowth is associated with poor oral hygiene and local factors, it leads to secondary inflammatory involvement which results in an increased bleeding tendency of the fibrous overgrowth.
Dental Treatment Considerations:
Dental treatment should be carried out after obtaining consent and precautionary guidance from the treating physician.
A strict anxiety reduction protocol should be followed.
Familiarisation with instruments, technique (systematic desensitisation) and modelling can effectively bring down the anxiety of the patient.
Advice on good oral hygiene maintenance is important to prevent secondary inflammatory involvement of the primary erotic drug-induced gingival enlargement.
Periodic reviews and oral prophylaxis are necessary.
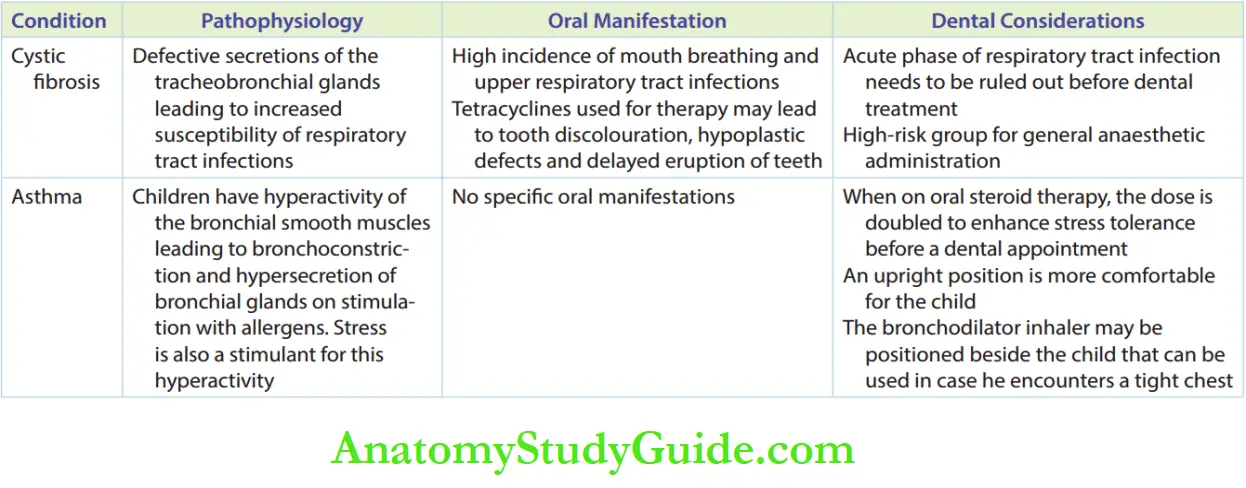
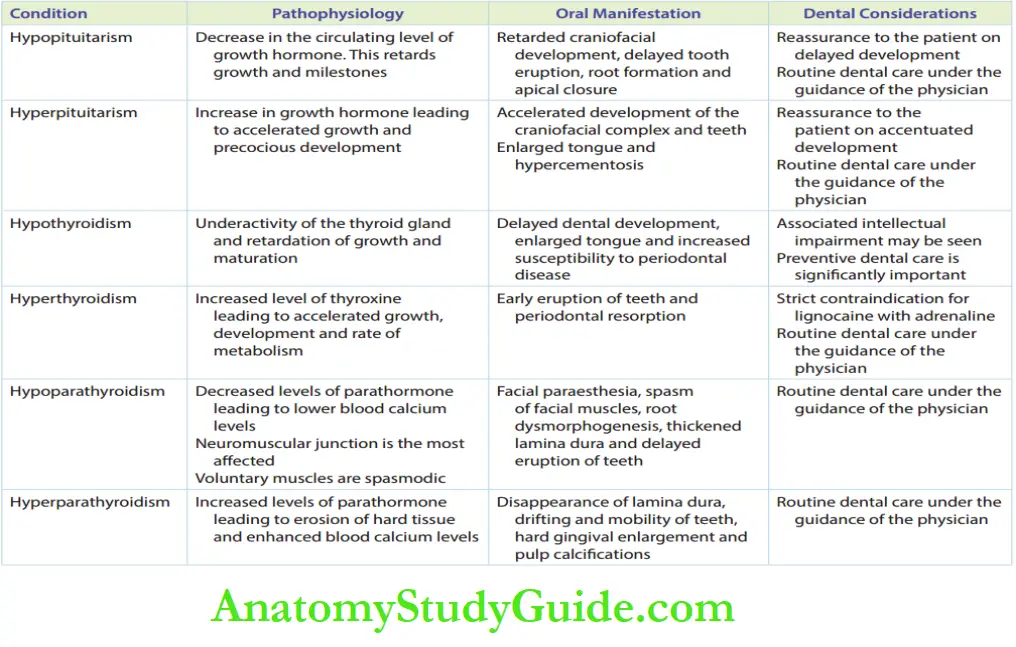
Respiratory Disorders And Endocrine Disorders
Respiratory disorders and endocrine disorders, respectively
Renal Disease
The formative, secretory and excretory functions of kidneys are affected in renal diseases.
RBC maturation, vitamin D synthesis, platelet maturation and reabsorption of calcium and phosphorous are formative/secretory functions of the kidney.
The excretion of endogenous metabolites and drugs is the excretory function of the kidney.
Renal disease is associated with proteinuria, marked anaemia, increased bleeding time, enhanced uraemic levels hypocalcaemia and osteolysis.
Oral Manifestations:
Marked anaemia with the pallor of the mucosa is seen. A decrease in platelets causes spontaneous gingival bleeding.
Gingiva is spongy and characteristically inflamed; this is called ‘uraemic gingivostomatitis’.
Uraemic breath is sensed in children.
Thinning of the lamina dura, discolouration of the teeth in lieu of chronic medications and hypoplastic enamel defects are other intraoral hard-tissue findings.
Dental Treatment Considerations:
Dental treatment needs to be carried out under the physician’s guidance and consent.
All drugs prescribed have to be intimated to the physician.
Steroid supplementation during dental treatment to enhance stress tolerance may be required for children on chronic steroid therapy.
Routine preventive dental care and periodic reviews are emphasised.
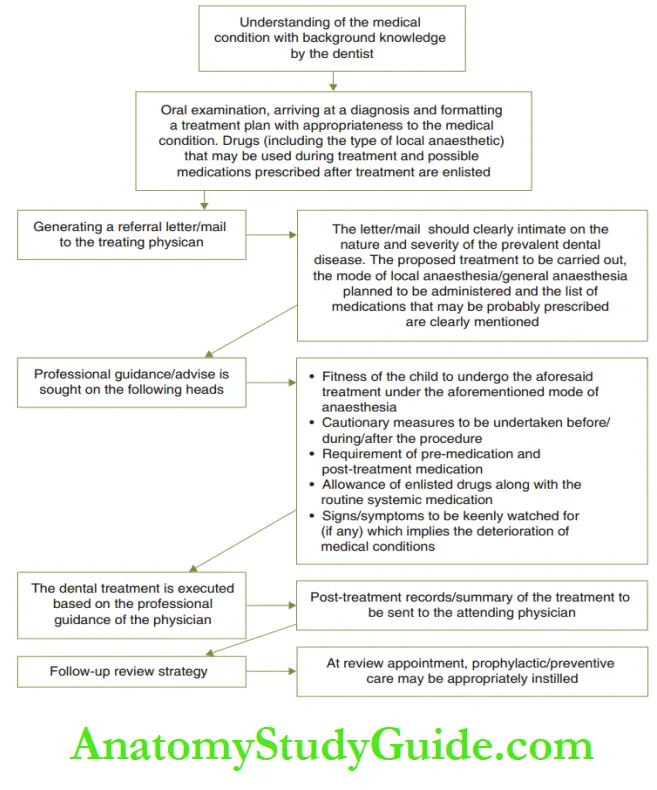
Outline Of Dental Management Of Medically Compromised Children
A medically compromised child needs the highest quality of dental treatment with enhanced safety.
It may be executed by mutual communication between the paediatric dentist and the treating physician.
The outline of management.
Management of Medically Compromised Children Summary
1. Children with an underlying chronic medical illness need special attention during dental therapy due to the following reasons:
- Monitoring vital systems
- Drug dosage modification
- Drug contraindication
- Specific behaviour management
- Dental treatment contraindication
- Pre-medication
Caution while performing oral procedures All medical conditions that require pre-treatment assessment by the consulting physician of the child.
2. The oral manifestations and points of special mention during the dental treatment of certain medical conditions are as follows:
3. Respiratory and endocrine disorders.
4. The outline of the management of medically compromised children.
Leave a Reply