Ludwig’s angina
Introduction: It is cellulitis (inflammation of the fascia) of the floor of the mouth.
1. Site: A swelling appears below th chin and inside the mouth. It is deep to mylohyoid.
2. Boundaries: It is limited
Table of Contents
- Laterally by two halves of mandible, and
- Posteriorly by hyoid bone. This is because of the attachments of investing layer of deep cervical fascia to the base of mandible and hyoid bone.
Read And Learn More: Head Anatomy Notes And Important Questions With Answers
3. Cause: It is usually secondary to caries of molar teeth.
4. Complications: If infection spreads backwards, it causes oedema of glottis. It may result into asphyxia.
5. Applied anatomy: The abscess is drained by a deep incision below the mandible by dividing the mylohyoid muscle.
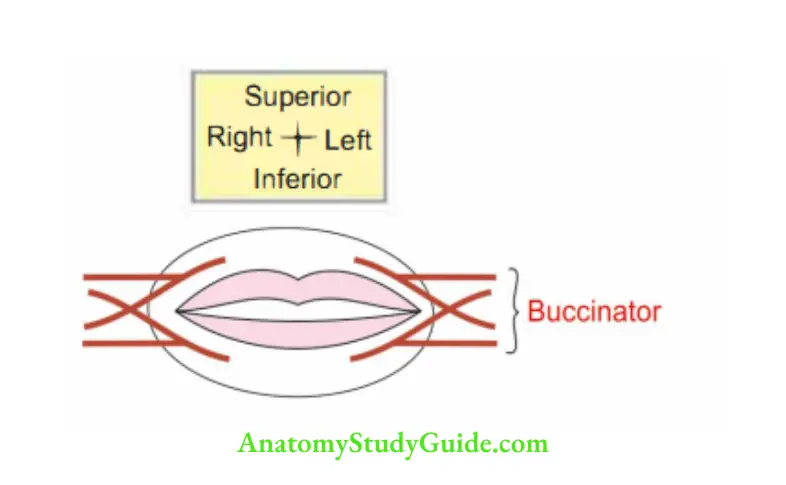
Buccinator
Introduction: It is an accessory muscle of mastication. It is indispensable for the return of bolus from the vestibule to the oral cavity .
1. Action
- Accessory muscle of mastication.
- It is useful in blowing.
2. Development: It is developed from the mesenchyme of 2nd branchial arch.
3. Proximal attachments:
- It has bony origin from the bone above and below the oral cavity, i.e. maxilla and mandible.
- Fibrous band from pterygomaxillary ligament.
- Raphe part from pterygomandibular raphe.
4. Distal attachments:
- Upper and lower fibres to the respective lip.
- Middle fibres decussate and push to the lips.
5. Peculiarities: It is pierced by parotid duct opposite th crown ofupper 2nd molar tooth It has double nerve supply.
6. Nerve supply
- Proprioceptive by buccal branch of mandibular division of trigeminal nerve (Vth cranial nerve).
- Motor by buccal branch of facial nerve (Vllth cranial nerve).
Uvula (small grape)
1. Definition: It is conical projection hanging from inferior surface of soft palate.
2. Folds: Two curved folds of mucous membrane extend laterally and downwards.
- Anterior fold: Palatoglossal arch or anterior pillar of fauces. It contains palatoglossus.
- Posterior fold: Palatopharyngeal arch or posterior pillar of fauces. It contains palatopharyngeus.
Pas savant’s ridge
1. Definition: Palatopharyngeus is a longitudinal muscle of pharynx.
The upper fibres of both sides encircle and form a circular bundle. They act as a sphincter.
They give an elevated appearance called Passavant’s ridge.
2. Relations: Internal to the superior constrictor.
3. Site: Posterior wall of nasopharynx.
4. Function: Prevents entry of food in nasopharynx.
5. Applied anatomy
- It is hyprtrophied in cases of complete cleft palate.
- In case of paralysis of the ridge, the food regurgitates into nasopharynx.
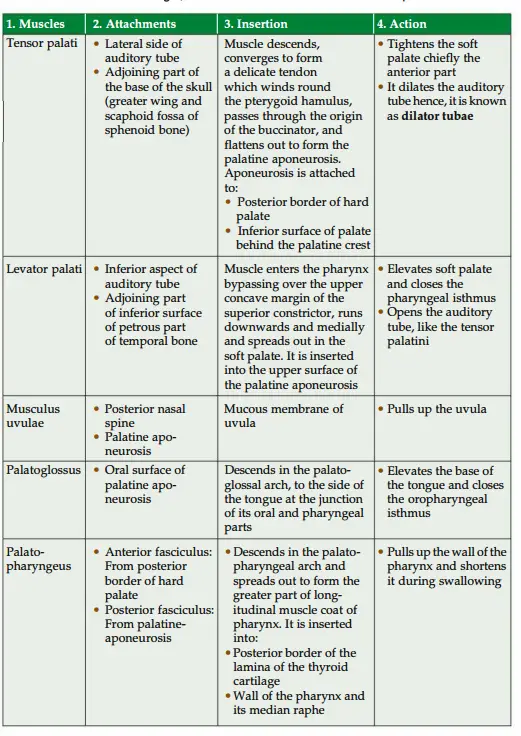
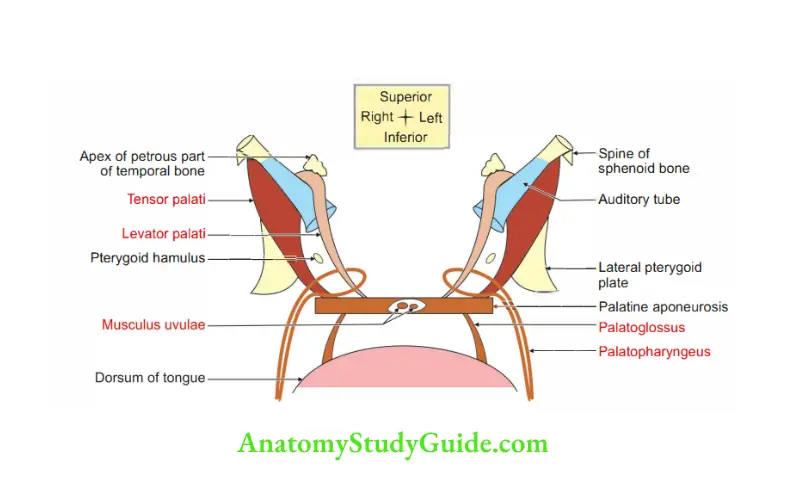
Question 1: Describe muscles of soft palate under the following heads:
1. Muscles,
2. Attachments,
3. Insertion,
4. Action,
5. Nerve supply, and
6. Blood supply
Answer:
5. Nerve supply
1. Motor nerves: All muscles of the soft palate are supplied by pharyngeal plexus except tensor palatini, which is supplied by the mandibular nerve.
The fibres of this plexus are derived from the cranial part of the accessory nerve (through vagus).
2. General sensory nerves are derived from
- Lesser palatine nerves, which are branches of the maxillary nerve (through the pterygopalatine ganglion) and from the
- Glossopharyngeal nerve.
3. Special sensory (gustatory) nerve: The fibres travel through the greater petrosal nerve-geniculate ganglion of the facial nerve-nucleus of the solitary tract.
4. Secretomotor nerves: Lesser palatine nerves. They are derived from the superior salivatory nucleus and travel through the greater petrosal nerve.
6. Blood supply of soft palate
1. Arterial supply
- Greater palatine, branch of maxillary artery.
- Ascending palatine, branch of facial artery.
- Palatine artery, branch of ascending pharyngeal artery.
All these arteries anastomose freely in the soft palate.
2. Venous drainage: Most of the venous blood is drained laterally through wall of pharynx.
The veins are paratonsillar veins which open into pharyngeal venous plexus and the pterygoid plexus.
Palatine aponeurosis
Introduction: It is expanded tendon of insertion of tensor veli palatini muscle.
1. Features
- Attachments: Anteriorly, posterior border of hard palate.
- Structure: It is thin, firm fibrous sheet.
- Encloses musculus uvulae.
2. Functions
- It supports the muscles of soft palate.
- It gives strength to soft palate.
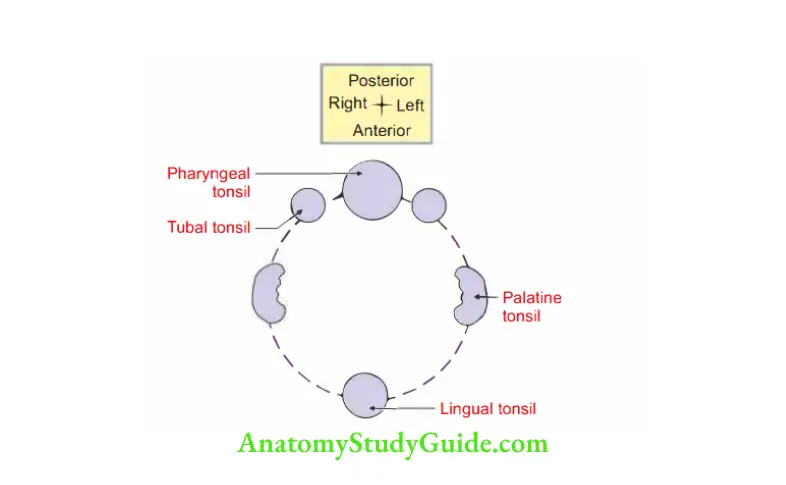
Waldeyer’s ring
It is a ring of submucosal lymhoid tissue which surrounds the begi ni respiratory and gastrointestinal tracts.
1. Formation
- In front and below: Lingual tonsil.
- On each side: Palatine tonsil.
- Above and on each side: Tubal tonsil.
- Above and behind: Nasopharyngeal tonsil.
The internal ring of Waldeyer drains into precervical chain of lymph node and deep cervical lymph node which together constitute the “external ring of Waldeyer”.
2. Functions
- It filters tissue fluid coming from inner surface of oral cavity.
- It prevents the entry of organisms from outside and thereby acting as a guard.
- It serves as the first line of defense and protects the body against ingested and inspired bacteria byproducing antibodiesagaint such invadinorganisms. When the tonsil itself becomes infected, it becomes a source for the spread of infection.
3. Applied anatomy
- Waldeyer’s ring forms a strong defense system to prevent the spread of infection from the oral and nasal cavities into the lower respiratory tract consisting of larynx, trachea, bronchi and lungs
- The lymphatic ring helps in defensive mechanism of the respiratory and alimentary systems by destroying the entry of microorganisms from the external environment.
- In pre-antibiotic era: Enlargement of the lymphoid follicle in the Waldeyer’s ring was blocking the respiratory tract.
Palatine tonsil
1. Gross: Tonsils are collection of lymphoid tissue situated bilaterally in the lateral wall of oropharynx.
1. Situation: Tonsillar sinus between palatoglossal and palatopharyngeal folds.
2. Dimension: 2 cm
3. Capsule: Capsule is condensed connective tissue present on the lateral side. It can easily be separated from the pharyngeal muscular wall except at its C anteroinferior part.
4. Morphology
- Two surfaces: Medial and lateral.
- Two borders: Anterior and posterior.
- Two ends: Upper and lower.
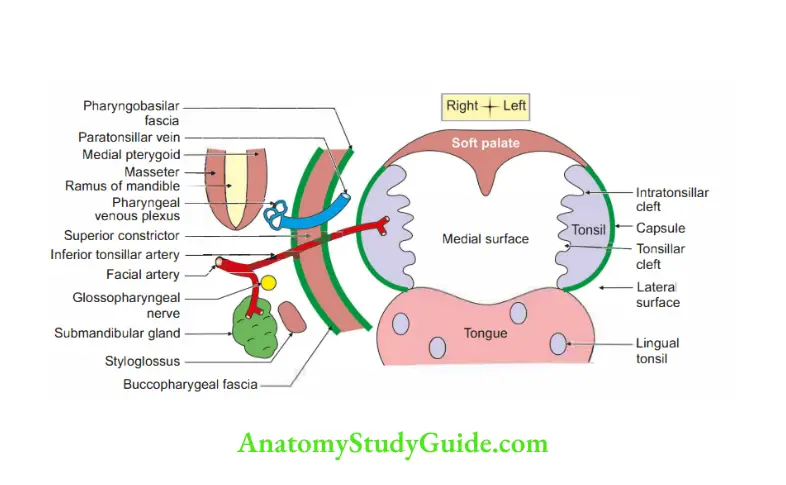
2. Relations
1. Surface
- Medial: Presence of 8-12 crypts.
- Lateral: Bed of tonsi
- Capsule of tonsil
- Peritonsillar space which contains paratonsillar vein.
- Superior constrictor which is lined by pharyngobasilar fascia inside and buccopharyngeal fascia outside.
Artery
- Facial artery and its branches
- Ascending palatine and Tonsillar
- Ascending pharyngeal artery.
- Muscle
Styloglossus muscle, - Medial pterygoid muscle, and
- Posterior belly of digastric.
- Glosspharyngeal nerve
- Gland: Submandibular and parotid gland.
Border
- Anterior: Palatoglossus.
- Posterior: Palatopharyngeus.
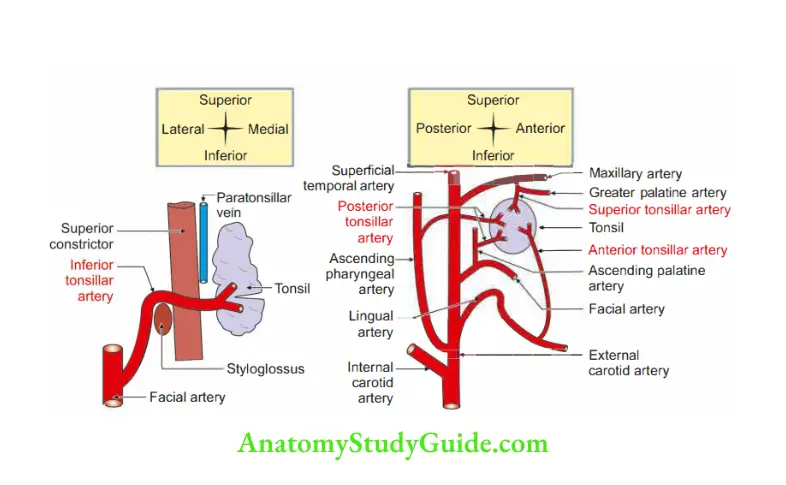
3. Blood supply
1. Arterial supply
1. Main source: Inferior tonsillar branch of facial artery. It enters the tonsil from its lateral surface.
2. Additional sources:
- Anterior tonsillar, a branch of lingual artery.
- Posterior tonsillar, a branch of
Ascending palatine branch of facial artery
Ascending pharyngeal artery - Superior tonsillar, a branch of descending palatine.
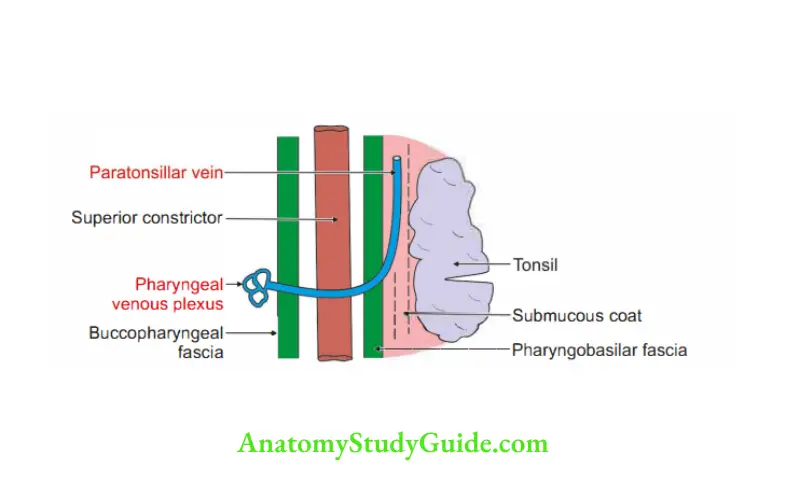
2. Venous drainage
- Into the pharyngeal venous plexus.
- Principal drainage is by the paratonsillar vein, which opens into pharyngeal venous plexus.
4. Nerve supply: Glossopharyngeal nerve.
5. Development
1. Chronological age: It develops in the 4th week of intrauterine life.
2. Genn layer: The epithelium develops from the endoderm of the 2nd pharyngeal pouch and remaining structures from the local mesenchymal tissue.
3. Source:
- Tonsillar fossa develops from ventral part of the 2nd pharyngeal pouch.
The endodermal cells proliferate outwards as solid buds which are subsequently canalized to form tonsillar pits and crypts. Lymphocytes either develop from mesoderm of adjoining arches or from circulating lymphocytes. - Tonsil is aggregation of lymphocytes. It belongs to lymphatic system which develops from secondary mesoderm. It is called neural crest cells.
4. Site: On the lateral side of oral cavity.
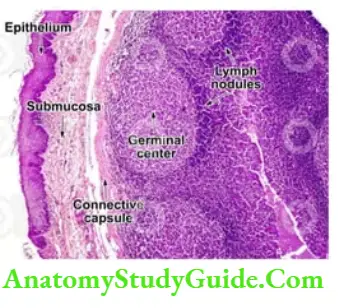
6. Histology: It is lymphoid organ consisting of
Stratified squamous non-keratinized epithelium covering the free surface.
With crypts
Fibrous capsule on the outer side, and
Lymphoid tissue (diffuse and lymph nodule)
7. Applied anatomy
- Referred pain from the infected tonsil extends to the middle ear, because both are supplied by the glossopharyngeal nerve.
- The capsule of the tonsil is removed during tonsillectomy because it is attached to deep surface of the tonsil and extends to form septa which conduct nerves and vessels.
- After tonsillectomy, all clots in the tonsillar fossa are removed. It prevents the interference of retraction of blood vessels.
- Quinsy is infection of peritonsillar space (peritonsillar abscess.)
- Rupture of paratonsillar vein is most common cause of tonsillar haemorrhage in tonsillectomy procedure.
After tonsillectomy and after postpartum haemorrhage are the areas where clot formation is prevented.
Such removal of clots is also done in uterus after delivery to prevent postpartum haemorrhage.
8. Lymphatic drainage: Tonsilis notfully coveredby a capsule. Thereis no subcapsular sinus or afferent lymphatics.
Dense plexuses of the fine lymphatic vessel surround each follicle and form efferent lymphatics.
They drain into jugulodigastric lymph nodes.
9. Site: It is present below and behind angle of mandible.
It is . .ar interval between the junction of internal jugular vein, facial vein and posterior belly of digastric.
This is considered principal lymph node of tonsil since it is primarily enlarged in tonsil.
Pharyngeal tonsil
1. Features
- It is also called ‘the adenoids’.
- It consists of a collection of lymphoid tissue beneath the epithelium of the roof and posterior wall of the pharynx.
- It is one of the important members of Waldeyer’s ring.
- It is unpaired organ.
- It is prominent in children.
- It usually undergoes atrophy after puberty.
2. Applied anatomy
1. Marked hyprtrophy of adenoids blocks the posterior nasal openings.
It makes the patient to snore loudly at night and to breathe through the open mouth.
2. In chronic inflammation, it may
- Block the nasopharynx and cause mouth breathing.
- Block the auditory tube and cause deafnss and middle ear infection.
- Inflammation of the pharyngeal tonsils (adenoids) is called adenoiditis.
- Sometimes the palatine and pharyngeal tonsils are removed during the tonsillectomy and adenoidectomy operation.
Question 2: Describe pharynx under the following heads:
1. Parts,
2. Structure of pharynx,
3. Muscles of pharynx,
4. Blood supply,
5. Nerve supply, and
6. Applied anatomy
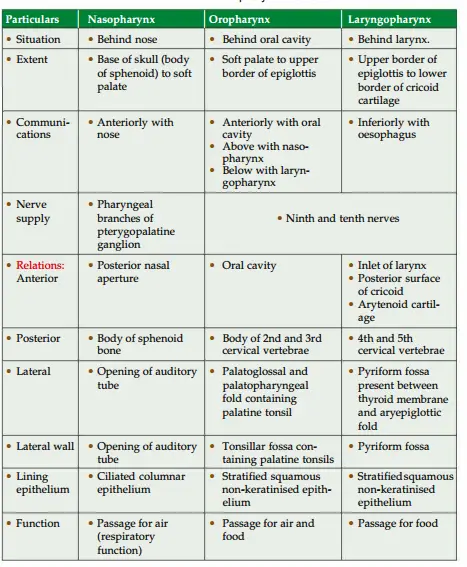
Anawer: 1. Parts: It is a wide, muscular tube situated behind the nose, mouth and larynx. It is divided into three parts:
- Nasopharynx,
- Oropharynx, and
- Laryngopharynx.
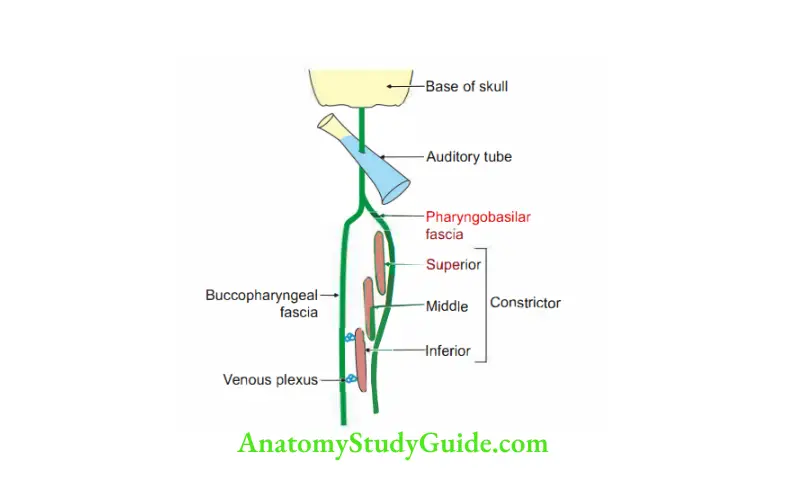
2. Structures of pharyx
- Mucosa.
- Submucosa.
- Pharygobasilar fascia: Fibrous sheet filling the gap extending from base of skull to upper margin of superior constrictor muscle.
4. Muscular coat
1. Outer circular muscle consists of
- Superior constrictor,
- Middle constrictor, and
- Inferior constrictor.
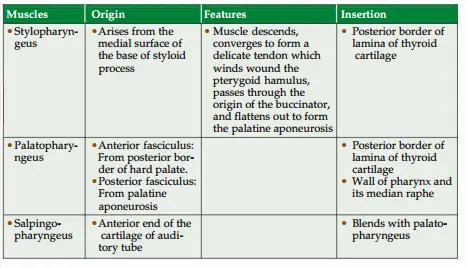
2. Inner longitudinal layer consists of
- Stylopharyngeus.
- Salpingopharyngeus.
- Palatopharyngeus.
3. Muscles of pharynx are described as inner longitudinal and outer circular.
The circular muscles of pharynx are described as follows
1. Proximal attachments
1. Superior constrictor: It has four parts
1. Pterygopharyngeus arises from
- Posterior border of medial pterygoid plate, and
- Pterygoid hamulus.
2. Buccopharyngeus arises from pterygomandibular raphe.
3. Mylopharyngeus arises from posterior end of mylohyoid line of mandible.
4. Glossopharyngeus arises from side of tongue.
2. Middle constrictor
1. Chondropharyngeusarises from
- Lower part of stylohyoid ligament, and
- Lesser cornu of hyoid bone.
2. Ceratopharyngeus arises from upper border of greater cornu of hyoid bone.
3. Inferior constrictor arises from
1. Thyropharyngeus (propulsive part):
- From oblique line of thyroid cartilage, and
- The tendinous band across the cricothyroid muscle.
2. Cricopharyngeus (sphincter part: From side of the cricoid)
2. Distal attachments
- Pharyngeal tubercle, and
- Median pharyngeal raphe.
2. Longitudinal muscles of pharynx are described in Table 14.3.

4. Blood supply
1. Arterial supply
- Ascending pharyngeal, branch of external carotid artery.
- Ascending palatine (branch of facial artery)
- Tonsillar artery
- Dorsal lingual branch of lingual artery
- Greater palatine branch of maxillary artery.
2. Venous drainage: Form a plexus which drains into internal jugular and facial veins.
3. Lymphatic drainage
- Retropharyngeal, and
- Deep cervical group of lymph nodes.
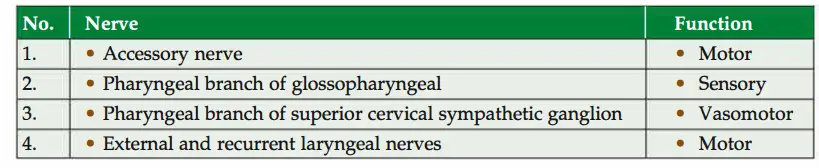
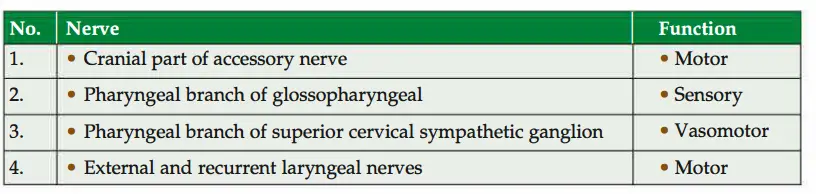
5. Nerve supply: Pharyngeal plexus which is formed by
1. Sensory
- General: Pharyngeal branch of glossopharyngeal nerve.
- Special: Taste fibres through internal laryngeal nerve, a branch of superiorlaryngeal nerve, branch of vagus nerve. “
2. Motor
- Somatomotor: Pharyngeal branch of vagus-chiefly motor.
- Secretomotor: Fibres from greater petrosal nerve.
- Vasomotor: Pharyngeal branch of superior cervical sympathetic ganglion.
6. Applied anatomy
- Dysphagia: Difficulty in swallowing.
- Killian’s dehiscence.
Question 3: Describe inferior constrictor muscles under
1. Gross anatomy
2. Applied anatomy
1. Gross anatomy
Answer: 1. Inferior constrictor: It is the thickest of the three constrictor muscles and is usually described in two parts.
Thyropharygeus
- Proximal attachment: It arises from oblique line of the lamina of thyroid cartilage.
- Distal attachment: Pharyngeal raphe
- Arrangement of fibres: The upper muscle fibres of inferior constrictor overlap middle constrictor.
- Nerve supply: Cranial root of accessory nerve (pharyngeal plexus).
- Action: It constricts lower part of pharynx.
2. Cricopharyngeus: It is rounded and thicker than the flat sheets of other constrictors. It extends from one side of cricoid arch to other side of cricoid arch.
- Proximal attachment: It arises from the side of the arch of the cricoid cartilage.
- Distal attachment: It blends with circular oesophageal fibres around the narrowest part of pharynx.
Nerve supply
Action: It acts as a sphincter at the junction of the laryngopharynx and the oesophagus.
2. Applied anatomy
- On the posterior surface of pharynx, there is a gap between two components of inferior constrictor, called “pharyngeal dimple” or “Killian’s dehiscence”.
The mucosa and submucosa of pharynx may bulge through the weak area to form the pharyngeal diverticulum. - In spasm of cricopharyngeus, there is failure of the relaxation of cricopharyngeus.
The bolus of food fails to move downward. Hence, it is pushed in the region of Killian’s dehiscence producing a pharyngeal diverticulum.
It is also called pharyngeal pouch. - Patient presents dysphagia (difficulty in swallowing) if pharyngeal pouch is filled with food.
- Third stage of swallowing is brought by inferior constrictor of pharynx.
In this stage, the food passes from lower part of the pharynx to the oesophagus.
Pharyngobasilar fascia (pharyngeal aponeurosis)
Introduction: Between the base of skull and upper border of superior constrictor, there is a gap called “sinus of Morgagni”.
It is closed internally by a rigid membrane called pharyngobasilar fascia.
1. Extent: It extends from the upper border of superior constrictor muscle of pharynx to the base of the skull.
2. Attachments
1. Above
- Basilar part of occipital bone.
- Petrous part of temporal bone.
- Posterior border of medial pterygoid plate.
- Pterygomandibular raphe.
2. Below: It gradually becomes areolar and merges in pharyngeal muscles and never extends below superior constrictor muscle.
3. Features
- It is non-expansible sheet of fascia.
- It is strengthened by pharyngeal ligament, a midline thickening.
4. Structures piercing: Auditory tube.
5. Function: It keeps the wall of nasopharynx permanently open for breathing.
Pferygomandibular raphe
Introduction: It is a thin band of tendinous fibres between buccinator anteriorly and superior constrictor posteriorly.
1. Extent: It extends
- From hamulus of medial pterygoid plate
- To the posterior end of mylohyoid line of the mandible.
2. Relations
- Medially: Mucous membrane of the mouth.
- Laterally: Adipose tissue and ramus of mandible.
3. Attachments
- Anteriorly to the central part of buccinator, and
- Posteriorly to the superior constrictor of pharynx.
4. Surface anatomy: In wide opened mouth, the raphe raises a fold of mucosa that marks internally the posterior boundary of cheek.
It is important landmark for the inferior alveolar nerve block.
5. Applied anatomy: The pterygomandibular space lies lateral to the pterygomandibular raphe.
It contains lingual and inferior alveolar nerves.
This is the site for the injection for inferior alveolar nerve block.
Auditory tube
Introduction: It is a funnel y shaped tube which connects middle ear cavity to nasopharynx.
1. Gross
- Length: 36 mm.
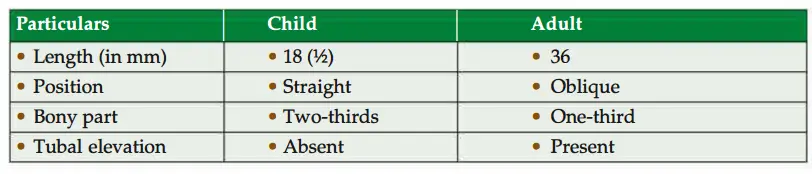
2. Parts: Two parts.
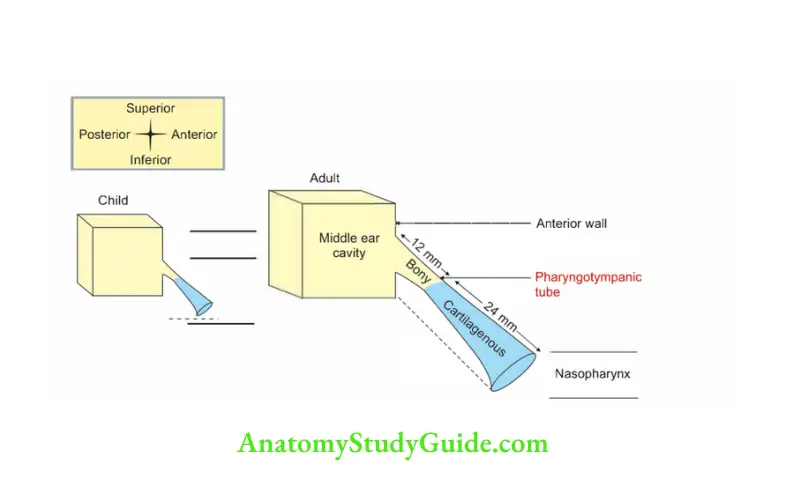
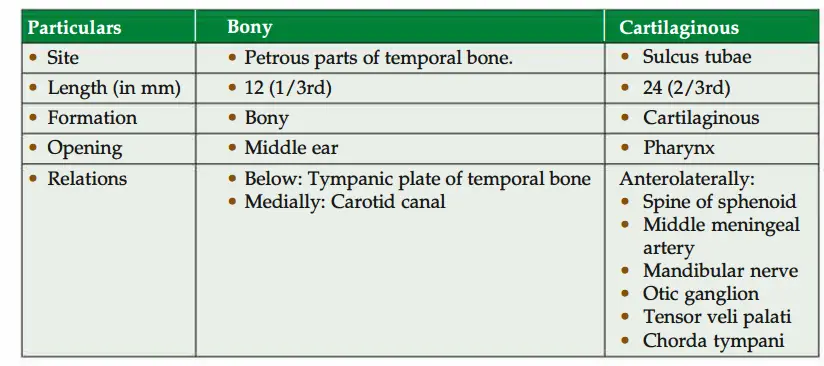
3. Age difference
4. Blood supply:
- Middle meningeal artery (maxillary artery).
- Ascending pharyngeal artery (external carotid artery).
5. Venous drainage: Pterygoid venous plexus.
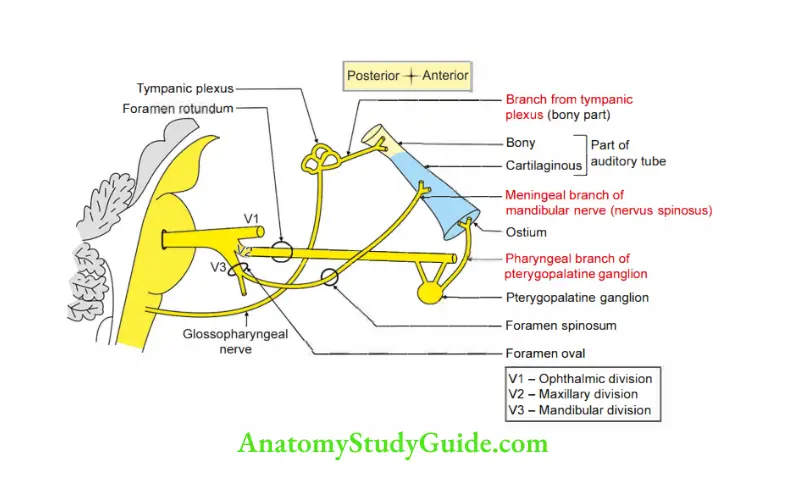
6. Nerve supply: There are three nerves supplying various parts of auditory tube.
- Bony part of auditory tube is supplied by a branch from tympanic plexus.
- Cartilaginous part is supplied by meningeal branch of mandibular nerve.
- Ostium of the auditory tube is supplied by pharyngeal branch of pterygopalatine ganglion.
7. Functions
- Maintains equilibrium of air pressure on either side of tympanic membrane.
- Increased pressure in middle ear forces the auditory tube to open with a click.
8. Applied anatomy
1. In children, infection of oral cavity, nasal cavity or pharynx usually spreads to the middle ear because auditory tube is short in length and horizontal in position.
2. Sometimes tube is blocked due to inflammation of tubal tonsil.
3. The tube can dysfunction due to
- Blockage of tube due to cold,
- Congestion of nasal mucosa or tube
- Pressure variation
4. Glue ear (otitis media with effusion): Absorption of air in the middle ear.
Air is replaced by fluid.
It leads to conductive deafnss and sometimes pain in air.
In children, it leads to learning disability.
5. Barotrauma: Due to significant difference of pressure on both sides of tympanic membrane, there can be damage to middle ear. This situation occurs in
- Rapid ascent as in mountaineering
- Scuba (Self-contained underwater breathing apparatus) diving
- Pilots who travel the air craft without using air pressure cabin.
- In landing or taking off
- From hill you are rapidly coming down
6. The tympanic membrane may pull inward or outward depending upon pressure ingredients.
This separates tympanic membrane and develops severe pain in the ear.
7. Conductive deafnss is defined as a type of deafnss which is due to impaired function of those components of ear which are involved in the conduction of sound energy.
8. Following are the causes for conductive deafnss
- Causes in external auditory meatus
- Large wax in the external ear
- Foreign body in external ear
- Infection in external ear
- Tympanic membrane is dysfunctional or perforated or because of barotauma
- Problems in the middle ear
- Problems in ossicles
- Air is replaced by fluid
- Cholestatoma in the middle ear
Tensor palatini (dilator tubae)
1. Proximal attachments: It arises from
- Lateral side of cartilaginous part of auditory tube. It is outside pharynx.
- Sulcus tubae,
- Spine of the sphenoid bone, and
- Scaphoid fossa of medial pterygoid plate of sphenoid bone.
2. Distal attachments: It is inserted in the form of aponeurosis which is attached to
- Posterior border of hard palate.
- Inferior surface of hard palate behind palatine crest.
3. Peculiarities
- It is more active in blowing and less active in sleeping.
- Its tendon hooks round the pterygoid hamulus and passes medially to expand to form the palatine aponeurosis of its lower half.
4. Relations
1. It lies anterior to levator palatini muscle.
2. Laterally, it is related to
- Mandibular nerve
- Auriculotemporal nerve
- Chorda tympani nerve
- Otic ganglion, and
- Middle meningeal artery.
5. Blood supply
- Ascending palatine branch of facial artery.
- Greater palatine branch of maxillary artery.
6. Actions
- Its primary role is to open the pharyngotympanic tube, e.g. during deglutition and yawning.
Thus, it equalizes the pressure between the middle ear and nasopharynx, and - Tightens the soft palate, chiefly the anterior part.
- It dilates the auditory tube; hence, it is known as dilator tubae.
7. Development: It develops from mesoderm of 1st pharyngeal arch.
8. Nerve supply: It is supplied by the mandibular nerve, nerve of 1st pharyngeal arch.
Development of palate
1. Chronological age:
- Eighth week of intrauterine life.
- Palatogenesis begins at the end of 5th week. However, it is not completed until 12th week.
- Critical period of development: End of 6th week to the beginning of 9th week
2. Germ layer: Mesoderm of pharyngeal arches.
3. Site: At the primitive oral cavity.
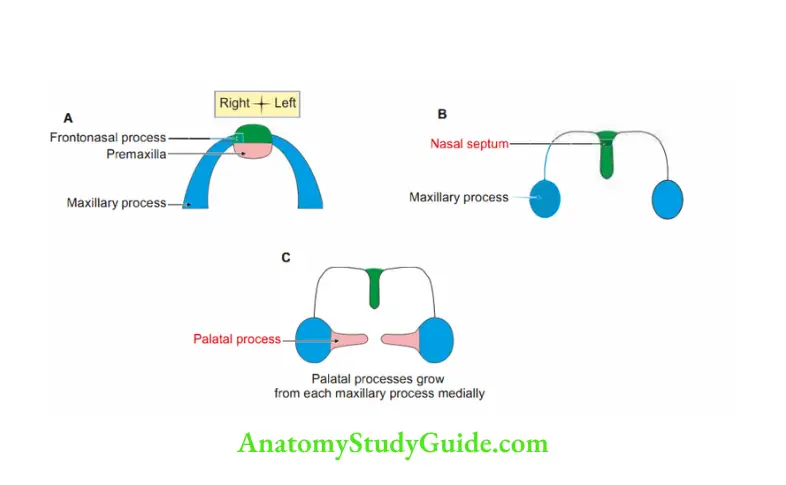
4. Sources: It consists of two parts
1. Primary palate: It is an area in front of incisive fossa. It is developed by fusion of
- Medial nasal process, and
- Maxillary process.
2. Secondary palate: Permanent palate lies behind primitive palate. It is developed from fusion of
- Left and right palatine process of both maxillae in midline.
- The fusion between the primitive and permanent palates takes place in a ‘Y’ shaped manner.
The fusion extends from before backwards.
3. Anterior 314th of permanent palate: Ossifies and fuses with nasal septum.
- Posterior 1 /4thof the permanent palate does not fuse with lower edge of nasal septum and hangs as soft palate.
5. Anomalies
- Cleft palate
- Cleft lip
Cleft palate
Introduction: It is failure of fusion of primitive and permanent palates. It varies in
degree of severity.
1. 1st degree: Bifid uvula.
2. 2nd degree: Ununited palatal process.
3. 3rd degree: Ununited palatal process and a cleft of one side of premaxilla.
4. 4th degree: It is rare. Ununited palatal process and cleft on both sides of premaxilla.
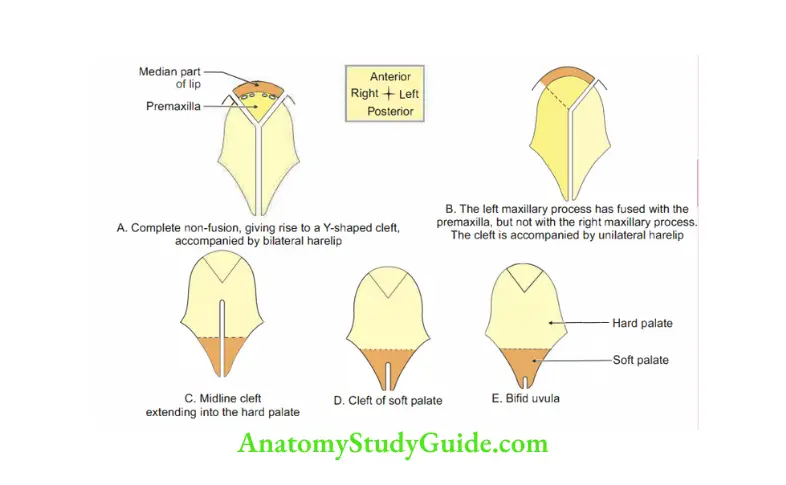
Cleft lip
1. Incidence: It is most common abnormality. The incidence is 1:750 births.
2. Cleft lip: Due to failure or union of the
- Medial nasal process with the
- Maxillary process of the mandibular arch.
3. Situation: It may be unilateral or bilateral. It is more frequently unilateral. It runs down from the nostril.
Development of oral mucosa
1. Parts: The mouth cavity consists of two parts
- The primitive mouth is derived from ectodermal stomodeum.
- The definitive mouth is developed from endoderm of the cephalic part of foregut.
2. Division of stomodeum: The stomodeum is divided by the development of the primitive and permanent palate into
1. Nasal: The nasal component of the stomodeum forms the
- Mucous membrane of the nasal cavity,
- Nasal septum, and
- Palate.
2. Oral cavities: The oral component of the stomodeum forms the
- Mucous linings of the cheek (vestibule of the mouth),
- Lips,
- Gums, and
- Enamel of the teeth.
3. Germ layers: The floor of the definitive mouth is developed from the foregut because the mucous lining of the tongue is entirely derived from the endodermal elements of the branchial arches.
4. Process of development: The epithelial cells lining the margins of the primitive oral fissure proliferate outward into the surrounding mesenchyme.
Eventually the epithelial cells breakdown, and the endodermal alveolus-labial sulcus thus formed separates the lips and the cheek from the gums and teeth of the jaw.
Leave a Reply