Oral Mucous Membrane
Mucous membrane can be defined as a thin moist sheet of tissue that covers or lines body cavities or canals that communicate with the exterior, such as the linings of the oral cavity, digestive tube, respiratory passages, genitourinary tract, etc.
Table of Contents
Read And Learn More: Oral Histology Notes
It consists of a surface layer of epithelial tissue covering a deeper layer of connective tissue and functions to protect the underlying structures, lubricates the surface, absorbs water, salts and other solutes.
Mucous membrane lining the oral cavity is called oral mucous membrane or oral mucosa.
Functions Of The Oral Mucosa
Protection:
- Oral cavity comes under a variety of stimuli during function and rest. The oral mucous membrane shows morphological and histological adaptations to withstand these insults.
- Multilayered, stratified squamous type of epithelium of the oral mucosa is specialized to act as an effective barrier against frictional, microbial, thermal and chemical stresses.
- The presence of keratinized surface in areas which come under masticatory load affords further protection to underlying structures from mechanical forces.
Mastication:
- Mastication is chiefly performed by teeth but few other parts of the oral cavity like the hard palate, gingival and dorsal surface of tongue also play a role in this process.
- Oral mucosa in these locations shows morphological and histological
adaptations (such as hard keratinized surface, firm attachment to underlying tissues) which help in crushing and grinding of food.
Absorption:
- Oral mucous membrane is selectively permeable and can absorb small molecular weight molecules.
- The subepithelial connective tissue of the oral mucosa is richly supplied by a network of capillaries which further help in absorption.
Clinical Consideration
– This absorptive function of oral mucosa is utilized for the
administration of certain drugs directly through the oral mucous membrane into the bloodstream.
Secretion and lubrication:
- Oral mucosa contains numerous salivary glands distributed within the subepithelial connective tissue (the minor salivary glands) which secrete theirproducts through small individual ducts opening on the surface of mucosa. The secretions of these glands are usually rich in mucous and help keep the surface of the oral cavity lubricated and moist.
- The posterior part of the anterior two-third of the dorsal surface of the tongue contains numerous serous salivary acini that secrete thin watery saliva which helps in diffusion of food particles into the taste buds for stimulating gustatory sensation.
Sensory:
- Oral mucosa can perceive a number of sensory stimuli. The connective tissue of the oral mucosa contains receptors for pain, touch, pressure and temperature which help to prevent injury to tissues due to any noxious stimulus.
- The epithelium of the oral mucosa contains certain sensory cells (Merkel cells) which provide sensory capabilities to the oral epithelium. Receptors for gustatory sensation (taste buds) are unique to the oral cavity.
Clinical considerations:
– Thermal receptors allow us to assess the temperature of food and drinks preventing extremely hot or cold substances from reaching and injuring tissues of the elementary tract.
– Touch, pressure and pain receptors can perceive sharp objects which if ingested can possibly damage tissues of the gastrointestinal tract.
– Sensory receptors in the oral mucosa are responsible for various oral reflexes such as swallowing (deglutition), gag reflex, retching and salivation.
Classification Of Oral Mucosa
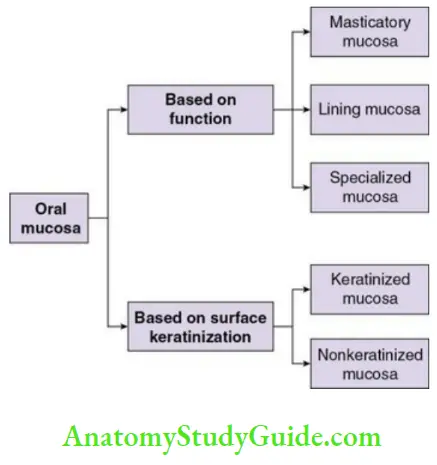
Based on Function
1. Masticatory Mucosa:
- Masticatory mucosa is located in those areas of the oral cavity where the oral mucosa plays some role in mastication.
– Hard palate
– Gingiva
– Dorsal surface of tongue - The mucosa covering these areas tends to be tightly bound to the underlying structures like bone or muscle and tend to demonstrate a hard surface covered by dense keratin protein.
2. Lining (reflecting) Mucosa:
- Most other parts of the oral mucosa not involved with mastication act as a lining tissue and hence called lining mucosa. These areas include
– Inner surfaces of the cheek (buccal mucosa), and the lip (labial mucosa)
– Floor of mouth
– Ventral and lateral surfaces of tongue
– Vestibular fornix
– Soft palate
– Lining over jaw bone (alveolar mucosa), etc. - The mucosa covering these regions tends to be distensible and adapts
itself to the movements of various structures of the oral cavity.
3. Specialized Mucosa:
- The oral mucosa is unique as compared to the mucosa covering any
other part of the body due to its special ability to perform the function of taste sensation (gustation). - Specialized sensory structures (taste buds) are found in certain specific locations of oral cavity within the mucosa and provide the facility of taste sensation. Majority of taste buds are concentrated on the dorsum of the tongue with few distributed along the lateral border of the tongue, soft palate, upper oesophagus, cheek, and epiglottis.
Based on surface keratinization
1. Keratinized Mucosa:
Keratinized mucosa are the areas of the oral mucosa where the surface of the epithelium exhibits a layer of cornified cells (keratin). Such type of mucosa is found in the
– Hard palate
– Attached gingiva
– Filiform and circumvallate papillae present on the dorsal surface of the tongue
2. Nonkeratinized Mucosa:
These are the areas of oral mucosa where the surface the epithelium does not demonstrate the presence of keratin. Such type of mucosa is found in the
– Buccal mucosa
– Labial mucosa
– Floor of mouth
– Ventral and lateral surfaces of tongue, fungiform papillae on dorsal surface of tongue
– Vestibular fornix
– Soft palate
– Alveolar mucosa
Organization Of Oral Mucosa
The organization of oral mucosa is similar to that of the skin. The oral mucosa basically consists of two components.
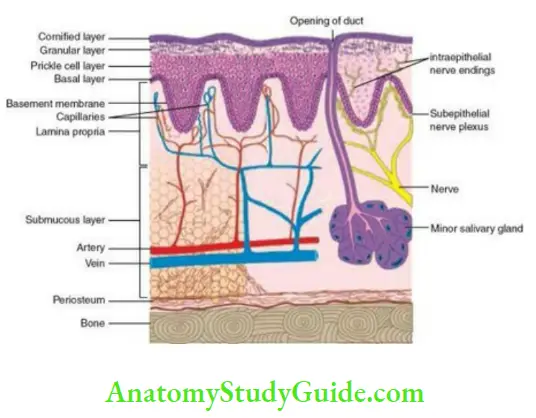
- An outer covering of oral epithelium which is avascular, aneural. It insulates the underlying tissues.
- The oral epithelium is supported by the connective tissue, called lamina propria, which contains the vascular and neural supply.
- Beneath the oral mucosa is a layer of loose connective tissue known as submucosa that supports the mucosa. The submucosa of the oral cavity blends indistinguishably with the overlying lamina propria and it is difficult to clearly identify the boundaries between the two (unlike in the gastrointestinal tract, where the submucosa is distinctly demarcated from the overlying mucosa by a layer of elastic fibres and smooth muscles).
The submucosa consists of
– Loose fatty connective tissue
– Minor salivary glands
– Nerves
– Blood vessels - In some parts of the oral cavity, the mucosa is directly attached to the periosteum of underlying jaw bone without intervening submucosa. This arrangement is called mucoperiosteum. This is found in sites where oral mucosa performs a masticatory function which requires the mucosal tissue to be tightly adherent to the bone with minimal mobility of the tissues.
The locations of mucoperiosteum include
– Medial zone of the hard palate
– Attached gingiva
Oral Epithelium
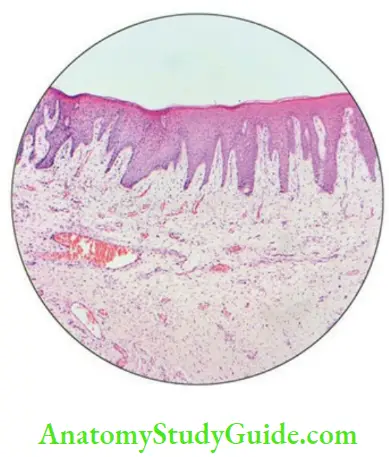
Epithelium lining the oral cavity forms the primary barrier between the oral environment and deeper tissues. To effectively perform its function as a barrier against mechanical, chemical, thermal, and microbial insults, the epithelium of the oral mucosa is a multilayered epithelium arranged in a number of distinct layers or strata known as stratified squamous type of epithelium.
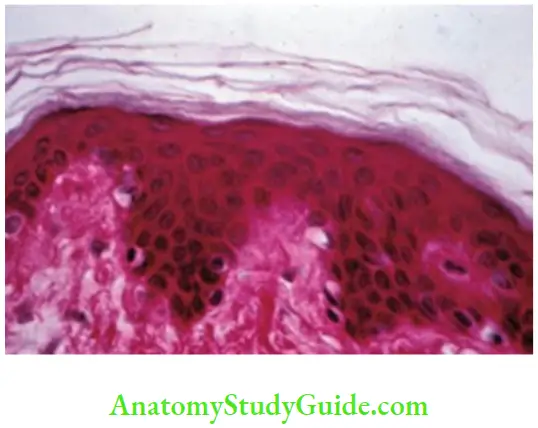
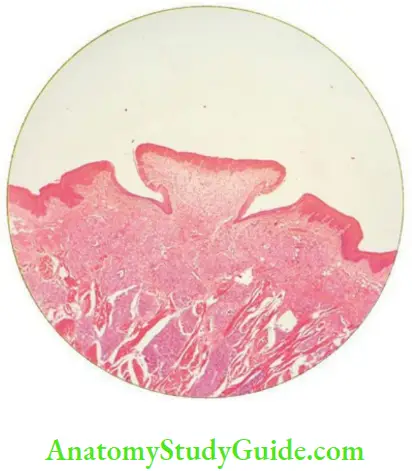
- Surface of the epithelium may be keratinized (Fig. 8.2) or nonkeratinized.
- Keratinization itself may be of two types
- Orthokeratinization: Superficial cornified cells are devoid of nuclei.
- Parakeratinization: Superficial keratinized cells have pyknotic
(degenerated) nuclei.
The interface between the epithelium and underlying lamina propria is not smooth but undulating in nature and thrown into a series of peg-like projections called rete pegs or rete ridges which interdigitate with finger-like protuberances called the papillae in the superficial portion of the connective tissue.
Clinical significance: This arrangement helps to form a strong mechanical interlocking between the epithelium and lamina propria, and prevents stripping off of the epithelial tissue under shearing or abrasive stresses.
The epithelium is separated from the connective tissue by an acellular structure, the basement membrane.
Epithelial Proliferation And Turnover
- The stratified squamous epithelium of the oral cavity is characterized by continuous process of renewal and maturation. The thickness of the epithelium and the number of layers for any site at any given time is constant. This balance is maintained by continuous shedding off of older cells and replacement by new cells.
- New cells are formed by cell division of existing cells in the deepest layer of the epithelium (proliferation) and senescent cells are shed off from the surface at various sites layer (exfoliation).
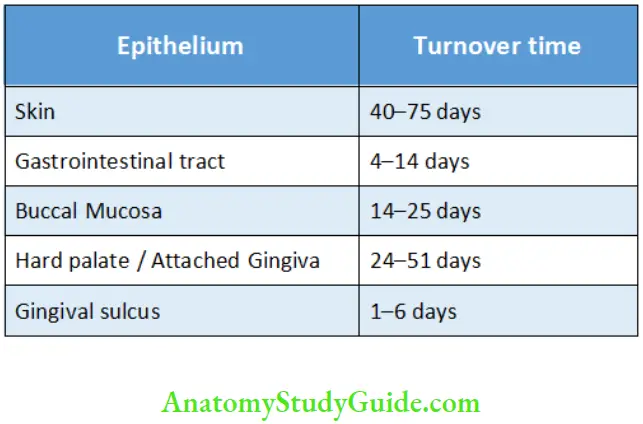
- Each newly formed epithelial cell goes through a process of maturation in which it passes through all the layers of the epithelium, from innermost to outermost, and is finally exfoliated from the surface. The time taken for an epithelial cell from its formation till it is exfoliated is called the turnover time. Turnover time
varies for different tissues and locations in the body (Table 8.1). - In general, nonkeratinized epithelium turns over faster than the keratinized epithelium.
Turnover Rate of Epithelium at Various Sites
The oral epithelium consists of two populations of cells
- The progenitor population: It is composed of stem cells and amplifying cells, which continually divide to provide new cells required for the replacement of exfoliated cells. This population of cells is restricted to the deepest layer of the epithelium.
- The stem cell is characterized by capability of infinite cycles of cell division. Each stem cell divides to produce two daughter cells:
- One remains as the stem cell.
- The other becomes an amplifying cell.
- The amplifying cell undergoes a few finite cycles of cell division leading to increase in number of cells (hence the name ‘amplifying’) after which these cells lose their capability to undergo further division and enter the maturation phase.
- The maturing population: These are cells which leave the cell cycle to undergo a process of differentiation by acquiring special characteristics of a stratified squamous epithelial cell and progress through different layers of the epithelium till finally exfoliated. Each cell in the maturing population goes through a series of morphological and structural changes continually acquiring specialized characteristics. Maturing cells are pushed outwards as newer cells are formed in the deeper layer. These cells move to higher layers until they reach the superficialmost layer from where they are shed or exfoliated.
Epithelial Maturation
Maturation of the oral epithelium is characterized by progressive changes in the morphology and structure of epithelial cells as they pass through various layers of the stratified epithelium.
- The maturation pattern is quite similar for the keratinized and nonkeratinized epithelium, but there are slight differences, which ultimately are related to the specific function of the epithelium.
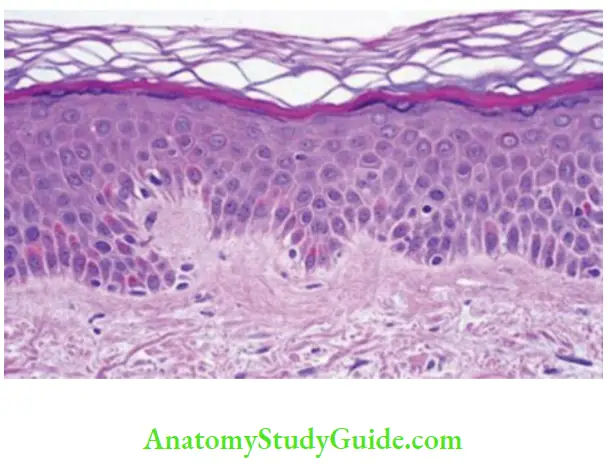
Structure And Maturation Of Keratinized Oral Epithelium
In locations of the masticatory mucosa, i.e. hard palate and attached gingiva, the epithelial surface is tough, inflexible and tightly bound to the lamina propria in order to resist abrasive forces. This toughness and inflexibility is provided by the formation of alayer of keratin on the surface of the epithelium and the process known as keratinization. When observed in routine microscopic sections, the cells of the keratinized epithelium can be divided into following four distinct layers of variable thickness (Box 8.1) having characteristic morphological appearances
- Stratum basale
- Stratum spinosum
- Stratum granulosum
- Stratum corneum
Layers Of Keratinized Epithelium
Stratum basale
Stratum spinosum
Stratum granulosum
Stratum corneum
Each individual epithelial cell starts from stratum basale and passes through spinosum, granulosum and corneum as it matures before being finally exfoliated. As the cell passes through these layers, there are changes in its morphological and structural characteristics, which constitute the maturation process in these cells.
Stratum basale:
Also known as the basal layer or sometimes as stratum germinativum.
It is the layer which contains the stem cells and amplifying cells that provide new cells for the epithelium. This layer constitutes one or rarely two innermost layers of the epithelium. The cells of the innermost layer rest on the basement membrane separating the epithelium from the connective tissue.
- Under light microscope, the cells of this layer are usually cuboidal to sometimes short columnar in shape and have moderately abundant eosinophilic cytoplasm with ovoid nucleus.
Ultrastructurally these cells show all the usual cytoplasmic organelles like mitochondria, ribosomes, endoplasmic reticulum and Golgi apparatus. - The basal cells have two populations of cells:
- Serrated which contain tonofilaments
- Nonserrated made up of slowly dividing stem cells
- The cytoplasm shows certain characteristic structures, known as tonofilaments, which are found only in epithelial cells and can be used to differentiate epithelial cells from all other cells of
- the body.
- Tonofilaments are filamentous intracellular proteins which are
classified under intermediate filaments. They make up the
cytoskeleton of epithelial cells and form components of intercellular bridges between epithelial cells. Chemically, they are made up of a family of proteins called cytokeratins. - A characteristic of epithelial cells, also seen in basal cells, is the presence of intercellular bridges known as desmosomes. Each cell is attached to its neighbouring cell by means of these desmosomes.
- Basal epithelial cells are attached to the basement membrane by means of hemidesmosomes which help to firmly bind the epithelial cells to the underlying tissues. They have a structure which is half of a desmosome hence they are called so. They are found only in the basal cells of the epithelium.
Stratum spinosum:
Also known as the spinous layer or prickle cell layer. It is called the prickle cell layer due to the presence of characteristic spiny thorn-like projections on the surface of the cells
formed by intercellular bridges or desmosomes connecting neighbouring cells. The layer appears spiny due to the shrinking of cells during tissue preparation leading to separation at points where the desmosomes do not anchor them together.
- This layer is most active in synthesis of proteins. It is the most prominent layer of the oral epithelium and constitutes the bulk of its thickness.
- When observed under light microscope, the cells of this layer are
- Larger in size as compared to cells in the basal layer.
- Polyhedral in shape with abundant eosinophilic cytoplasm.
- Possess round to ovoid nucleus.
- The cells of the spinous layer resemble a cocklebur or a sticker with each spine ending at a desmosome.
- Under the electron microscope
- They show all regular cellular organelles which were seen in basal cells.
- The tonofilaments, which were present as thin separate filamentous structures in the basal cells, start aggregating into small bundles known as tonofibrils.
- In the upper zones of the stratum spinosum, lamellate granular structures are seen which are known as lamellar bodies or Odland bodies or membrane-coating granules or keratinosomes.
- These are ovoid in shape, 200–300 nm in size and are secretory organelles, which produce a lipid-rich substance which coat the outer surface of the cell membrane and function as permeability barrier.
- The number of Odland bodies increases as the cells reach higher layers of the epithelium
- They are also found in the next layer, i.e. stratum granulosum.
Stratum Granulosum
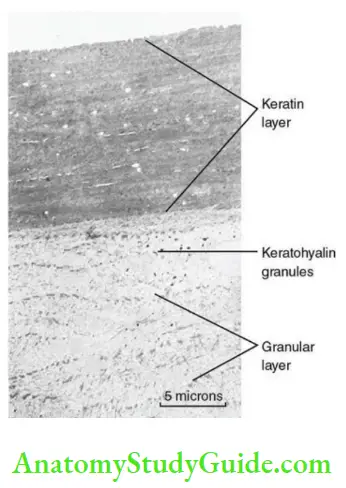
- The cells change in shape as they reach higher up in the epithelium. The epithelial cells now become progressively broader and start assuming the characteristic flattened appearance (From squamous → flattened).
- There is appearance of unique structures within the cytoplasm, which appear as dark basophilic granules when viewed under the light microscope. These are known as keratohyalin granules (hence the name stratum granulosum) and are characteristic of keratinized stratified squamous epithelium. Ultrastructurally, these are irregular-shaped electron dense structures, about 100–300 nm in size and are closely associated with tonofibrils.
- Keratohyalin granules are rich in two proteins; filaggrin and loricrin. Filaggrin (Filament aggregating protein) helps in aggregation of tonofilaments and formation of cross links between cytokeratin filaments. In the presence of this protein, tonofibrils begin to aggregate into thicker bundles and start accumulating within the cytoplasm.
- As the keratin protein starts accumulating within the cytoplasm, the other organelles start decreasing in numbers except for Odland bodies which become more abundant. The nucleus also starts showing signs of degeneration with every advancing layer.
Stratum corneum:
Stratum corneum is also called the cornified layer and is the outermost layer of the keratinized stratified squamous epithelium.
Marked morphological and structural changes take place in the epithelial cells once they reach this level.
- Cells become nonvital, dehydrated and completely filled with keratin protein.
- Light microscopically
- The cells appear markedly flattened disk like in shape (known as squames) with intensely eosinophilic cytoplasm. The nucleus may be degenerated and appear as a condensed, dark basophilic structure known as the pyknotic nucleus (parakeratinization) or may sometimes be completely lost (orthokeratinization).
- Ultrastructurally:
- The cells lose all their cellular organelles, become dehydrated and get completely filled with tightly packed tonofibrils now called keratin. Keratin is a highly eosinophilic protein, and hence, this layer appears brightly eosinophilic under the light microscope.
The tightly packed keratin and a tough insoluble cell envelop makes this layer highly resistant to chemical and mechanical stresses.
- As the cells reach the outermost layer, they are shed off by a process known as desquamation or exfoliation. This process is mediated by proteolytic enzymes secreted by the epithelial cells that gradually breakdown desmosomal proteins thus weakening the intercellular cohesion until it decreases to a critical level when the cell gets completely detached from its surrounding cells and is thus shed off.
The process of desquamation is extremely important to
- Maintain the homeostasis and balance of cell population in the oral epithelium.
- Prevent prolonged colonization of microbes on the surface of the epithelium.
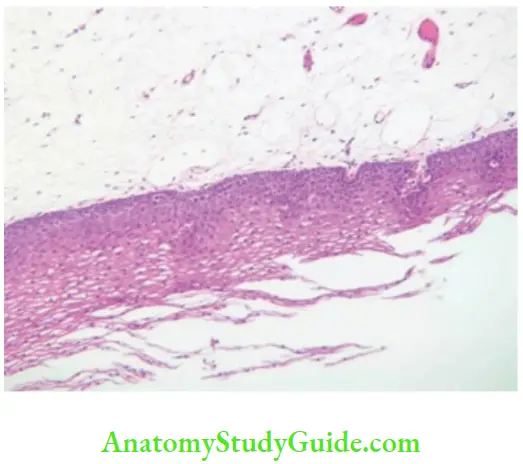
Structure And Maturation Of Nonkeratinized Oral Epithelium
The epithelium of the lining mucosa needs to be flexible to accommodate the mobility of these structures, and hence, there is no need for a tough keratinized surface. Accordingly, these areas are lined by nonkeratinized stratified squamous epithelium. The basic structure and arrangement of nonkeratinized epithelium is similar to that of the keratinized epithelium with few differences:
- The epithelium in nonkeratinized areas is usually thicker.
- Rete ridges are usually broader and shorter.
- Changes in size and shape of the cells in different layers are less dramatic.
- The cells in all layers of the nonkeratinized epithelium are slightly larger.
- The intercellular bridges are not as conspicuous, and thus, the term stratum spinosum is generally not used for describing the comparative layers in the nonkeratinized mucosa.
- Nonkeratinized epithelium is characterized by the absence of keratohyalin granules and consequently stratum granulosum and stratum corneum. Rarely few keratohyalin granules may be seen, but these do not contain filaggrin and loricrin and are not associated with tonofilaments.
- The cells present at the surface layer of the nonkeratinized epithelium are viable cells with functional cellular organelles.
The nonkeratinized epithelium is broadly divided into three layers based on their location
- Stratum basale
- Stratum intermedium
- Stratum superficiale
Laters Of Nonkeratinized Epithelium
- Stratum basale
- Stratum intermedium
- Stratum superficiale
The cells of the nonkeratinized epithelium also pass through all the layers before being exfoliated.
- Unlike the keratinized epithelium the cells constituting the supra basal layers do not show marked and sudden change in morphology or structure to be clearly demarcated into distinct layers.
- The changes in size and shape of the cells are gradual and not striking. Cells change from cuboidal to polyhedral to flattened shape, but the transition is gradual with no distinct demarcating events.
Stratum basale:
- The basal layer in the nonkeratinized epithelium functions to provide new cells.
- The cells are
- Cuboidal with moderately abundant eosinophilic cytoplasm
- Ovoid nucleus
- Show all routine organelles such as mitochondria, ribosomes, endoplasmic reticulum and Golgi apparatus
- These cells contain tonofilaments and show the presence of desmosomes and hemidesmosomes as in the keratinized epithelium.
Stratum intermedium:
- This constitutes the layers above the basal cells and makes the bulk of epithelial thickness.
- Cells of this layer are
- Polyhedral in shape with abundant eosinophilic cytoplasm
- Round to ovoid nucleus
- Slightly larger than cells at similar location in the keratinized epithelium
- The cells are attached to each other by desmosomes, but these are not seen as prominently as in the keratinized epithelium.
- Under the electron microscope, they show all regular cellular organelles as well as tonofilaments. These filaments are not aggregated to form tonofibrils but are dispersed throughout the cytoplasm forming the cytoskeleton.
- Odland bodies are less in number and produce a coating material, which is not as impermeable as that produced by the keratinized epithelium. Their structure is also slightly different with granules here that appear circular in shape with amorphous core as opposed to lamellar arrangement seen in keratinized epithelium.
- Cells of the upper intermediate layer show deposition of glycogen within the cytoplasm. This glycogen could possibly be related to the presence and maintenance of living viable cells till the superficial layers of the nonkeratinized epithelium. The surface of nonkeratinized epithelium consists of metabolically viable cells which will require energy. Due to the thickness of the epithelium these cells tend to be distant from the nourishment provided by the vascularity which is present within the lamina propria. The glycogen deposits present in the upper portions of the epithelium may be utilized for this purpose.
Stratum superficiale:
- The few superficialmost layers of nonkeratinized epithelium are made up of flattened cells and is known as stratum superficiale or stratum distendum (due to ability of these cells to exhibit some amount of stretching and flexibility as compared to the rigid, inflexible cells of stratum corneum of the keratinized epithelium).
- The superficial cells of the nonkeratinized epithelium are flattened disk like in shape and are called squames, but the amount of flattening is markedly lesser than that seen in cells of the keratinized epithelium.
- As the cells move higher in this layer, the number of cytoplasmic organelles the but the cells remain viable till the uppermost layer.
- Tonofilaments are present dispersed throughout the cytoplasm without aggregating into bundles. Because of lack of keratin formation, the cells of this layer do not take an intensely eosinophilic staining as compared to stratum corneum of keratinized mucosa.
- The superficial cells also show glycogen deposits, but these decrease as the cells move to higher layers.
- The cells finally degenerate, possibly because of depleted nutritional stores, and are subsequently exfoliated.
Keratin
- Keratins are intermediate filaments of a family of fibrous structural proteins which form the cytoskeleton of epithelial cells and are characteristic feature of these cells.
- These are present as filamentous strands called tonofilaments and also form integral components of desmosomes and hemidesmosomes.
- In the keratinized stratified squamous epithelium, under the influence of aggregating proteins such as filaggrin, tonofilaments tend to aggregate together into progressively thicker bundles which precipitate within the cytoplasm. As more and more bundles of tonofilaments accumulate within the cytoplasm, the cellular organelles degenerate and the cell becomes dehydrated and loses its viability. These protein packed cellular shells are now known as extracellular keratin or simply keratin.
- Keratin is extremely an insoluble and tough protein, widely distributed in the animal kingdom and makes up a variety of structures such as
- Hair, horns, nails, claws and hooves of mammals
- Nails, scales and claws of reptiles
- Shells of tortoise, turtle, etc.
- Feathers, beaks and claws of birds
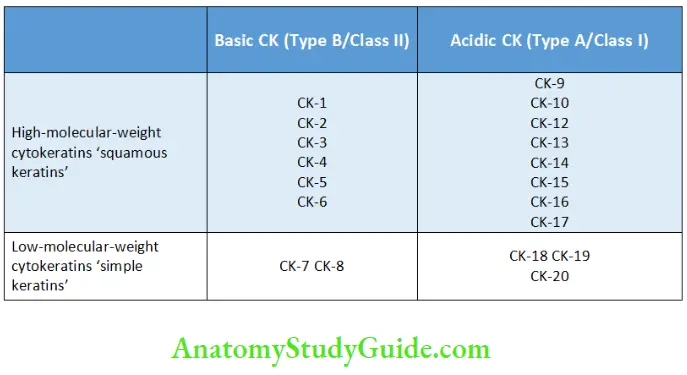
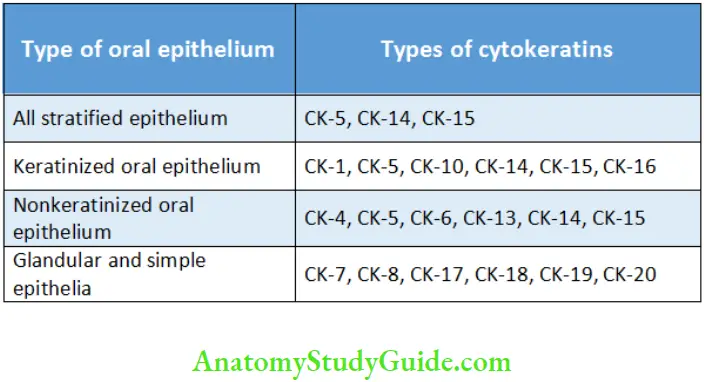
- Chemically keratin is made up of intracellular proteins called cytokeratins. These are a family of proteins numbered from 1 to 20 . Usually, cytokeratins are present in pairs and different keratin combinations are found in different epithelial tissues.
- Under normal physiological conditions, specific keratin combinations are found in specific tissues, but there may a change in keratin expression patterns. For example, under certain pathological processes, cytokeratins found in keratinized epithelium may appear in areas where normally epithelium is nonkeratinized leading to appearance of keratinization in these sites.
Classification of Cytokeratins
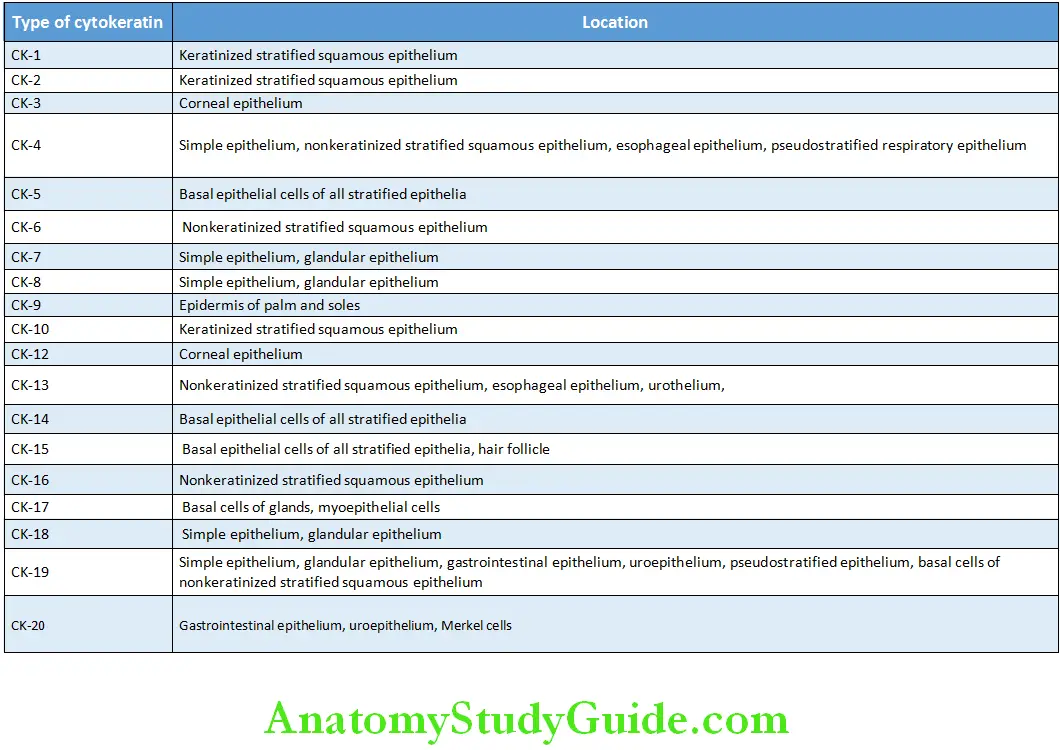
Distribution of Cytokeratins in Various Epithelial Tissues
Distribution of Cytokeratins in Various Locations of Oral Epithelium
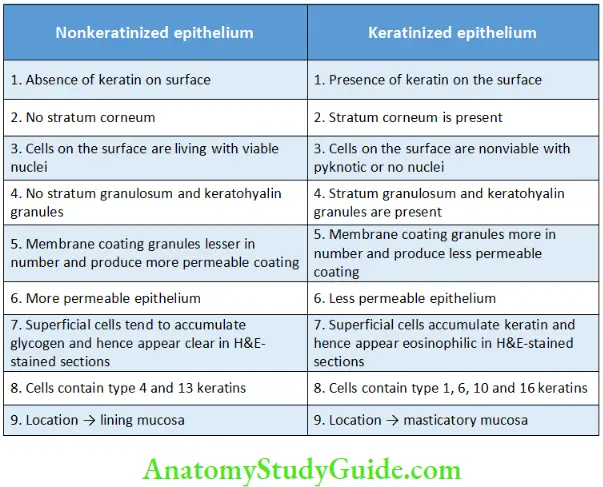
Cytokeratin is present in cells of all types of stratified squamous epithelium, whether keratinized or nonkeratinized, these cells are capable of producing surface keratin and are also known as keratinocytes. The difference between the presence of keratinization and nonkeratinization lies in ability of the epithelium to aggregate these cytokeratin filaments into thicker aggregates. The differences between keratinized and nonkeratinized epithelium have been summarized in Table.
Summarizing Difference between Keratinization and Nonkeratinization
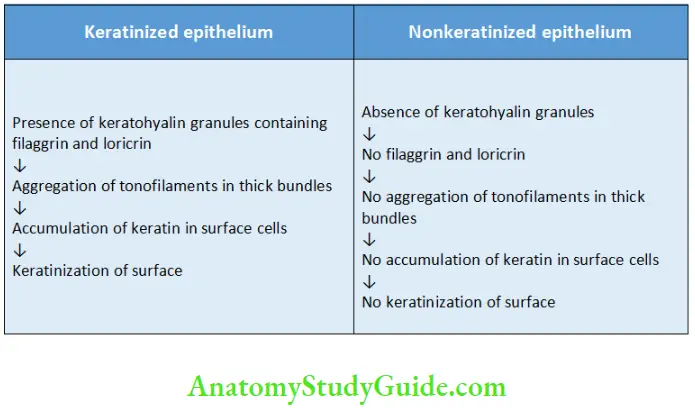
Differences between Keratinized and Nonkeratinized Epithelium
Nonkeratinocytes in the oral epithelium
Majority of the population of cells of the stratified squamous epithelium (90%) is constituted by keratinocytes, but the epithelium also contains a small portion (about 10%) of cells which do not produce keratin and are known as nonkeratinocytes.
- Heterogeneous group of cells in the oral epithelium which lack tonofilaments and hence the ability to synthesize keratin.
- These cells can be differentiated from keratinocytes in normal histologic sections by the fact that the cytoplasm of these cells does not take up eosin stain and hence appears as a clear halo around the nucleus as opposed to brightly eosinophilic cytoplasm of keratinocytes. Hence sometimes these cells are also called clear cells.
- They constitute about 10% of the total cell population of oral epithelial cells and consist of four different types of cells
- Melanocytes
- Merkel cells
- Langerhans cells
- Inflammatory cells
1. Melanocytes
Melanocytes are specialized cells which synthesize the pigment called melanin which is one of the number of factors responsible for a particular colour of oral tissues.
- Origin:
– Embryonically these are derived from the neural crest cells which migrate to the oral epithelium at about 11 weeks of gestation. - Location:
– These cells are located in the stratum basale in both keratinized as well as nonkeratinized epithelium sporadically interspersed between the basal keratinocytes.
– Also called low-level clear cells - Morphology:
– Under the light microscope and haematoxylin and eosin staining, the cytoplasm of melanocyte appears as a clear halo containing groups of dark brown granules known as melanosomes or melanin granules.
– Ultrastructurally, these cells lack desmosomes and tonofilaments and have dendritic processes that extend between the keratinocytes. - Function:
– The ratio of melanocytes to keratinocytes ranges from 1:10 to 1:15. Melanocytes and keratinocytes form epidermal melanin units; each unit consists of one melanocyte and a group of about 30–40 neighbouring keratinocytes.
– Melanin is synthetized within the melanocytes in small structures called melanosomes. These melanosomes are then injected into the keratinocytes of the unit by dendritic processes of the melanocyte.
– The number and density of melanocytes remains constant irrespective of skin colour of individuals or lightly or heavily pigmented areas. The difference in tissue shade is due to difference in activity of melanocytes.
– In heavily pigmented individuals or areas, the melanin may extrude from the epithelial cell to get deposited in subepithelial connective tissue. This the is known as melanin incontinence and the deposited melanin is usually taken up by macrophages which are called melanophages. - Staining:
– DOPA reaction – Cells containing tyrosinase appear dark and melanin-producing cells that contain tyrosinase are demonstrated.
– Masson Fontana stain (Silver stain)
– They appear spider like.
2. Merkel Cell
First identified by German anatomist Friedrich Sigmund Merkel in 1875.
- Origin:
Two hypotheses exist concerning the developmental origin of Merkel cells:
– The neural crest origin hypothesis
– The epidermal origin hypothesis
– currently accepted hypothesis for origin of mammalian Merkel cells - Location:
– Localized in the basal layer of the epidermis and found in close contact with enlarged terminal branches of myelinated afferent nerve fibres.
– Vary from 0.5% to 5% of all cells in the epidermis but can vary in different areas of the body. The palmar aspect of hands, the feet and plantar aspects of the toes, has a far higher density than any other part of the body. They are more numerous in the sun-exposed skin than in covered skin.
– In the oral cavity, they are found in high numbers in the lip, anterior hard palate and gingiva. - Function:
– The regions richer in Merkel cells are involved in tactile perception, suggesting that these cells are associated with sensory function. - Morphology:
– Using routine light microscopy of haematoxylin and eosin–stained human skin the Merkel cells can be hardly identified.
-Ultrastructurally, these cells are different from melanocytes by lack of dendritic processes and presence of some tonofilaments, desmosomes and hemidesmosomes.
– Some of the Merkel cells make contact with nerve terminals to form Merkel cell–neurite complexes.
– Characteristics of Merkel cells are secretory granules that are accumulated near the nerve fibre junction. These granules liberate transmitter substance across synapse-like junction between Merkel cells and nerve ending to transmit impulses. - Staining:
– PAS stain
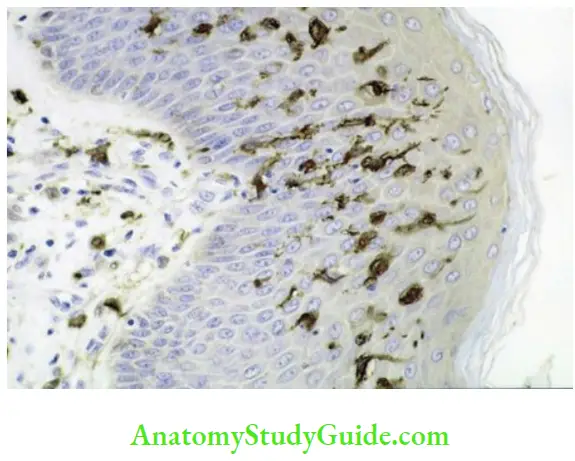
3. Langerhans Cell
First described by Paul Langerhans in 1868.
- Origin:
– Originate in the bone marrow from the precursors of the monocyte lineage and then migrate into the epithelium. - Location:
– These cells are seen in histological sections stained with
haematoxylin and eosin as ‘clear cells’ in suprabasal layers of mucous membranes.
– Also called high-level clear cells.
– These are dendritic cells with their cell bodies present usually in stratum spinosum and processes extending up to stratum corneum. - Morphology:
– Ultrastructurally, these cells lack tonofilaments and are characterized by the presence of small, rod-shaped or flaskshaped granules – Birbeck granules.
– These cells have the ability to move in and out of the epithelium and hence act as antigen-presenting cells which recognize and processes any antigenic material entering the epithelium and present it to T lymphocytes for mounting immune response. Thus, they help in immune surveillance. - Staining:
– Gold chloride
– ATPase
– Immunofluorescent markers
4. Inflammatory Cells
These are immune cells which are transiently present in the oral epithelium and keep moving in and out of the epithelium.
- These cells include
- Lymphocytes (most numerous)
- Polymorphonuclear leukocytes
- Mast cells
- These cells also function in immune surveillance
Nonkeratinocytes:
- Melanocytes
- Merkel cells
- Langerhans cells
- Inflammatory cells
Lamina Propria
Beneath the oral epithelium is a fibrovascular connective tissue which supports and nourishes the epithelial cells. The connective tissue of the oral mucosa is named as lamina propria and is equivalent to the dermis on the skin.
The lamina propria can be divided into two zones:
- Papillary lamina propria
- Reticular lamina propria
Papillary lamina propria:
- Superficial zone of lamina propria
- Named so as in this portion, the connective tissue extends in the form of fingerlike projections between the epithelial rete ridges
- Collagen fibres are delicate and loosely arranged and mostly run perpendicular to the epithelial surface
- Numerous delicate capillary loops and nerve endings are present in this zone
Reticular lamina propria:
- Deeper zone of lamina propria
- Named so because of the particular arrangement of collagen fibres which are arranged in an interlacing net-like like fashion (reticular = net-like).
- Collagen fibres in this zone are present as thicker bundles as compared to the papillary zone and run roughly parallel to the epithelial surface.
- This zone contains larger vessels and thicker nerve bundles
Lamina propria is made up of cells and extracellular components (chiefly fibres) all of which are embedded and dispersed in an amorphous gel-like matrix called the ground substance.
Components of Lamina Propria:
Cells
Fibroblasts:
Fibroblasts are principal cells of the lamina propria.
- Responsible for formation and maintenance of both the fibrillar components as well as the ground substance.
Morphology:
- Fusiform or stellate-shaped cells with indistinct cytoplasm and ovoid nucleus
- Possess long processes that tend to lie parallel to bundles of collagen fibres
- Nuclei contain one or more prominent nucleoli
Ultrastructure:
- They show characteristics of an actively synthetic cell.
- Rich in rough endoplasmic reticulum, Golgi complex, mitochondria and secretory granules.
- Cells may develop intracellular actin filaments and become contractile → mainly during wound healing.
After a certain period of active synthesis, the fibroblasts become latent and undergo certain morphological changes and are now known as fibrocytes.
- These cells lose their proliferative ability and active synthetic function.
- Under light microscope, they appear as thin spindle-shaped cells.
- Ultrastructurally the cellular organelles are markedly reduced in numbers.
Macrophages:
Macrophages are cells of haemopoetic origin and part of the immune system which also function as scavenger cells and remove cellular and extracellular debris.
- They are large phagocytic cells (macro = large, phagein = to eat) which are amoeba like in appearance and engulf extracellular material in a similar manner.
Origin:
- Circulating monocytes are precursor of these cells and once they come out of circulation they convert to macrophages.
Location:
- Macrophages have the ability to move around within the connective tissue (wandering macrophage) or they can become fixed at a particular site (fixed macrophage or histiocyte).
Morphology:
- Under light microscope, they appear as fusiform or stellate-shaped cells and are difficult to distinguish from fibroblasts.
Ultrastructure:
- Smaller and denser nuclei than fibroblasts
- Less number of rough endoplasmic reticulum
- Large number of lysosomes
Function:
- Phagocytosis → Ingestion of damaged tissue or foreign material
- Antigen processing and presentation
- Stimulation of fibroblast proliferation by the secretion of growth factors
- Ingestion of melanin which has extruded from the epithelium into connective tissue → melanophages
- Ingestion of hemosiderin which is formed due to the degradation of
extravasated RBCs → siderophages
Mast cells:
- Mast cells are also haemopoetic in origin and are also known as mastocyte or labrocyte.
Morphology:
- They appear as large spherical or elliptical cells with a small dense nucleus.
- The cytoplasm is eosinophilic and often difficult to appreciate in the background of eosinophilic collagen fibres. Metachromatic stains like toluidine blue can be used to demonstrate these cells in histological sections.
- Cytoplasm possesses numerous granules containing histamine and heparin.
Location:
- In lamina propria, these cells are usually found in close association with small blood vessels
Functions:
- Releasing histamines
- Maintenance of vascular homeostasis
- Angiogenesis
- Immune tolerance
- Defence against pathogens
Inflammatory cells:
- Although inflammatory cells are found in significant numbers in the oral mucosa only during response to injury or during wound healing, few scattered inflammatory cells are consistently present in the lamina propria under normal circumstances.
- Usually lymphocytes and plasma cells.
- These cells function in immune surveillance.
Fibres
Collagen:
- Collagen is the most abundant type of fibre found in the lamina propria and forms the bulk of this tissue.
- Mainly, Type I and Type III collagen fibres are found in lamina
propria. - Type IV and VII collagen are found in the basement membrane.
- Mainly, Type I and Type III collagen fibres are found in lamina
- Collagen fibres are present in the form of bundles which are arranged either loosely or densely depending on the location within the oral cavity
- In general
- In the papillary layer → Collagen is in thin and loosely arranged
- In reticular layer → thick bundles that lie parallel to the surface plane
Light microscope:
Collagen fibres are eosinophilic in appearance and are arranged in parallel bundles which give the lamina propria a characteristic bright eosinophilic hue in histological sections.
Elastic fibres:
- These fibres are principally made up of elastin protein and can stretch up to 1.5 times their length and snap back to their original length when relaxed.
- Found in small number in all locations of the oral mucosa but are more abundantly seen in areas lined by flexible lining mucosa.
- Not easy to appreciate in routine H&E-stained histological sections but demonstrated by using special stains like Weigert’s elastic stain.
Ground Substance
- Amorphous gel-like material, synthesized by fibroblasts, in which all tissue components are suspended.
- Primarily composed of water and heterogeneous carbohydrate complexes which are chemically divided into two groups
- Proteoglycans
- Glycoproteins
Proteoglycans are basically protein cores made up of polypeptide chains to which carbohydrate (glycosaminoglycan) side chains are attached. Chief proteoglycans found in the oral mucosa include
- Hyaluronan
- Chondroitin sulphate
- Dermatan sulphate
- Heparan sulphate
- Versican
- Decorin
- Biglycan
- Syndican
Functions:
- Provides support to the cells and extracellular components of the
connective tissue - Storage of water and nutrients
- Intercellular exchange between the cells of connective tissue
Epithelial Connective Tissue Interface The Basement Membrane
The interface between the oral epithelium and lamina propria is not a smooth regular interface.
- The under surface of the epithelium shows undulations with numerous peg-like extensions embedded into the connective tissue, known as rete pegs or rete ridges.
- Finger-like papillary extensions of the connective tissue project between the rete pegs thus forming an interdigitating arrangement.
The advantage of this type of arrangement is as follows:
- Increased surface area of contact between the epithelium and connective tissue leading to better attachment of epithelium to the connective tissue.
- More effective dispersal of mechanical forces to a larger surface.
- More effective exchange of nutrients and metabolic products between epithelial cells and connective tissue.
This arrangement is even more pronounced in areas of masticatory mucosa with more numerous and deeper rete pegs as these areas are exposed to much heavier load as compared to lining mucosa.
Cells of the deepest layer of the epithelium (stratum basale) are separated from the connective tissue by an acellular delineating membrane called the basement membrane, sometimes also referred to as basal lamina. Although just about 100 nm in thickness, the basal lamina has a complex structure.
Light microscope:
- Under H&E staining it appears as a structureless eosinophilic band on which the basal keratinocytes rest.
- When stained by periodic acid–Schiff (PAS) stain, the basal lamina appears as bright PAS-positive band running parallel to the basal cell membrane of basal keratinocytes.
Ultrastructure:
The basal lamina shows a complex structure with three distinct layers
- Lamina lucida
- Lamina densa
- Lamina fibroreticularis
Because of this structural complexity, the current concept considers this structure as basement membrane zone rather than a simple lamina.
Lamina lucida:
- The lamina lucida is named so because this layer appears electron lucent or clear under the electron microscope.
- It lies between the basal cell membrane of the epithelial cell and the lamina densa and is about 40 nm in thickness.
- It consists of attachment proteins which form the part of hemidesmosome that attaches the epithelial cells to the basement membrane. These include
- Bullous pemphigoid antigen (BPAg)
- Integrins
- Laminin
- Some studies suggest that this layer does not actually exist but is an artefact arising during tissue processing.
Lamina densa:
- The lamina densa is named so because this layer appears as electron dense under the electron microscope.
- This layer lies between the lamina densa and the lamina fibroreticularis and is 30–70 nm in thickness.
- Components of lamina densa are as follows:
- Type IV collagen which is arranged in a chicken wire-like configuration and forms the main framework of this layer
- Laminins
- Heparan sulphate which surrounds Type IV collagen network
Lamina fibroreticularis
- The lamina fibroreticularis is named so because this layer is made up of network of fibres (reticular = net-like).
- This layer is made up of Type VII collagen, known as anchoring fibrils, which is arranged as loops with their ends embedded in lamina densa.
- Fibrils of Type I and Type III collagen of reticular lamina propria pass through the loops of anchoring fibrils to form a flexible attachment between the basal lamina and subepithelial connective tissue.
Keratinized Areas Of the Oral Cavity
Masticatory mucosa
- Hard palate
- Gingiva
Specialized mucosa
- Tongue (dorsum)
Vermilion border/zone of the lip
Hard Palate
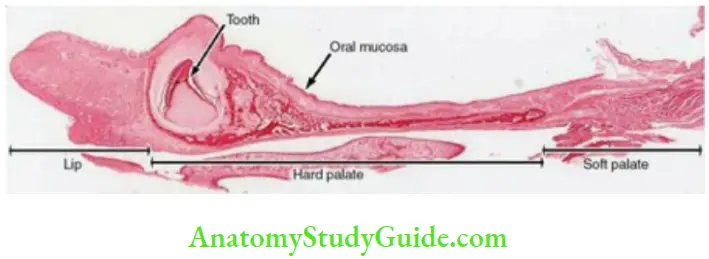
Mucous membrane:
- The mucous membrane of the hard palate is tightly attached to the underlying periosteum of the bone and thus immobile.
Colour:
- Pink
Epithelium:
- Keratinized stratified squamous epithelium.
- The cells of the stratum corneum are stacked upon each other.
- The adaptive changes to resist the masticatory forces are
- Desmosomes increase in number and length
- Density of tonofilaments increases
- Irregular epithelium connective tissue interface
Lamina propria:
- The connective tissue is dense.
- It is thicker in the anterior regions than in the posterior region.
- Numerous long connective tissue papillae are present.
Zones of the palate:
Four zones are observed in the palate due to variation in the submucosa.
Zones of the Palate:
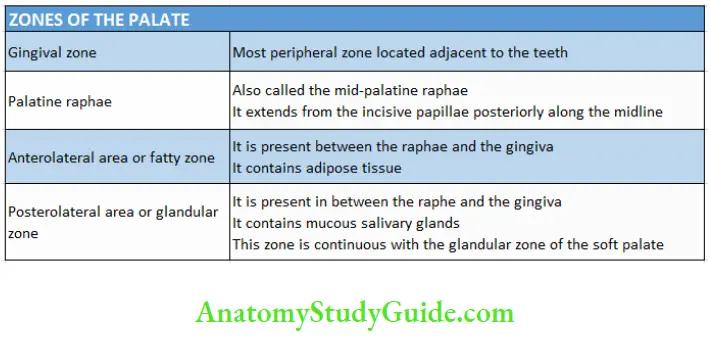
Submucosa:
- It varies in different parts of the palate.
- It is absent in the periphery in the zone adjacent to the gingiva and along the midline of the palate also called the mid-palatine raphae.
- The submucosa is present between the palatine gingiva and the mid-palatine raphae. The mucous membrane is firmly attached to the periosteum of the maxilla by dense vertical bands and fibrous connective tissue trabeculae.
- Loose connective surrounds the area at the junction of the alveolar process and the horizontal plate of the hard palate. This area is wedge shaped and contains anterior palatine vessels and nerves. This area is larger in the posterior than the anterior part of the palate.
Incisive papilla:
- Made up of dense connective tissue.
- The incisive papilla contains the oral parts of the vestigial nasopalatine ducts which are blind and lined by simple or pseudostratified columnar epithelium.
- Opening of mucous glands are seen in the lumen of the ducts.
- Cysts might arise from these ducts.
Palatine rugae:
- Palatine rugae are ridges of the mucosa which extend laterally from the incisive papilla to the anterior part of the mid-palatine raphae.
- The ridges are irregular and asymmetrical.
- The core of the rugae contains dense connective tissue with interwoven fibres.
Epithelial pearls:
- Remnants of the epithelium found in the lamina propria seen along the line of fusion between the two palatine processes.
Gingiva
The part of the oral mucosa that surrounds the neck of the tooth and covers the alveolar process is called the gingiva.
Colour:
- It is normally pink.
- The colour of the gingiva depends on the surface, thickness and the degree of pigmentation. The pink colour is due to the underlying blood vessels in the tissues and the circulating blood.
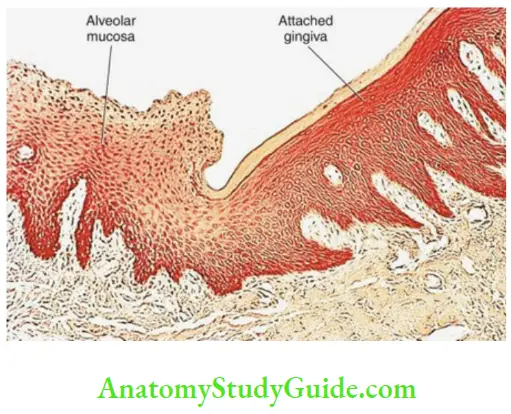
Extent:
- Dentogingival junction to the alveolar mucosa.
- The mucogingival junction separates the pale pink gingiva from the bright pink alveolar mucosa.
- A line of demarcation is present between the gingiva and the mucosa of the floor of the mouth.
- There is no sharp distinction between the gingiva and the palatal mucosa.
Parts :
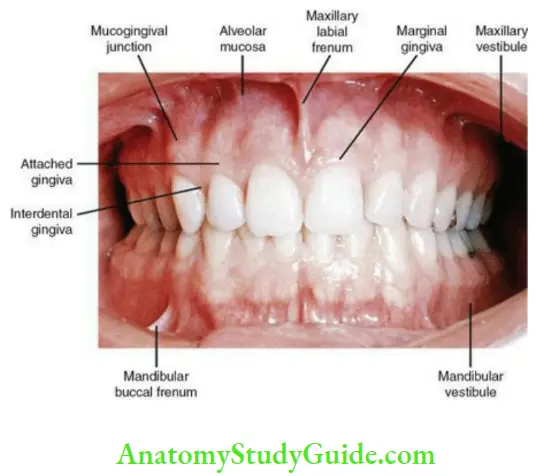
Parts of the Gingiva:
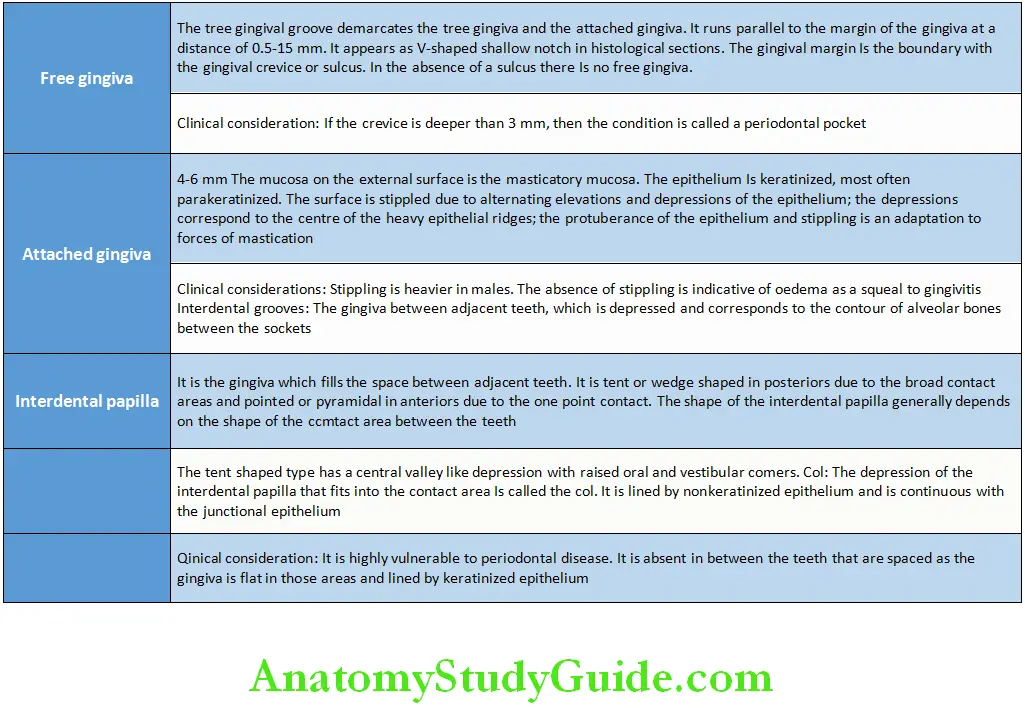
There are three parts:
- Free/marginal gingiva
- Attached gingiva
- Interdental papilla
Epithelium:
- In the general population, it is stratified squamous epithelium which is:
- Parakeratinized – 75%
- Keratinized – 15%
- Nonkeratinized – 10%
- The tissue appears whiter when keratinized.
- Stratified squamous epithelium which is either keratinized/non keratinized but mostly parakeratinized
Lamina propria
- Dense connective tissue.
- Connective tissue papillae are numerous, long and slender which is a distinguishing feature for the gingival mucosa.
- Few elastic fibres are present in the walls of the blood vessels.
- Majority of collagen fibres are Type I collagen. The turnover of collagen is faster in the gingiva than in other areas of the oral cavity.
- Collagen fibres are arranged in groups and are called the gingival ligament. The gingival ligament.
- Provides support to the free gingiva
- Binds the attached gingiva to the bone and the tooth
- Helps in linking one tooth to the other
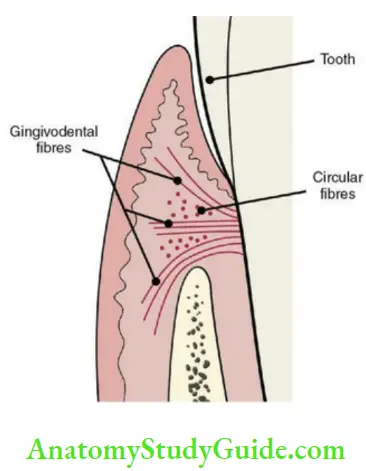
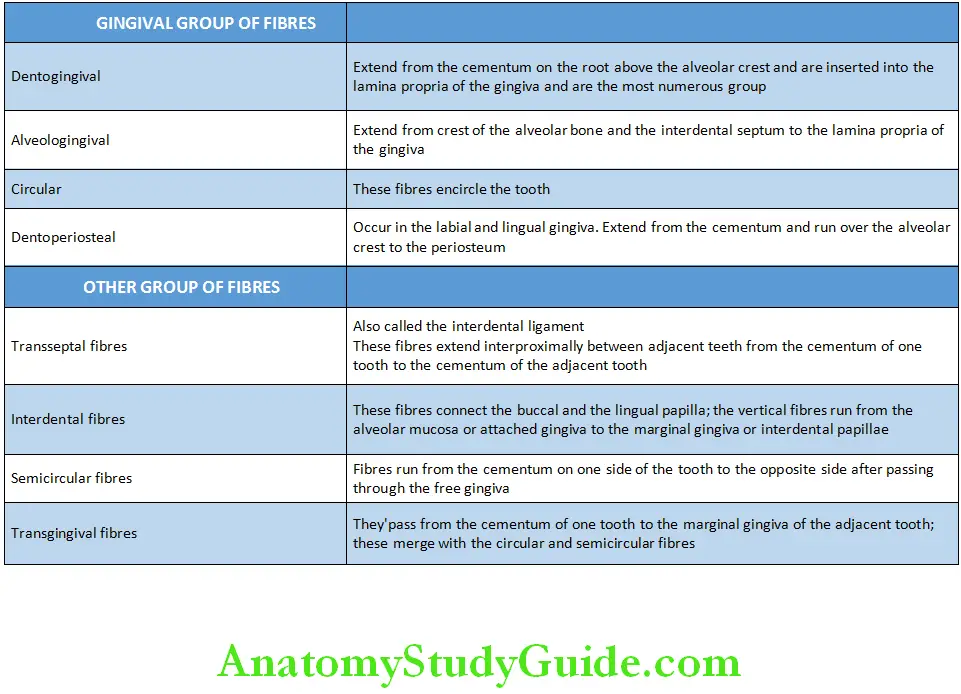
Fibres of the Gingiva
- The gingiva is firmly attached to the periosteum of the alveolar bone and is thus immovable. This type of arrangement is called the mucoperiosteum.
- The extracellular matrix has little ground substance and less Type III collagen. It is rich in hyaluronan.
- Submucosa is absent in the gingiva.
Vascular and nerve supply
Vascular supply:
- Interdental alveolar arteries that end in the interdental papilla supply it and the labial and lingual gingiva.
- Lymph vessels of the gingiva drain into the submental and submandibular nodes.
Nerve supply:
- Meissner/Krause corpuscles
- End bulbs
- Loops
- Fine nerve fibres that enter the epithelium as ultraterminal fibres
Vermilion Zone Of Lip And The Mucocutaneous Junction
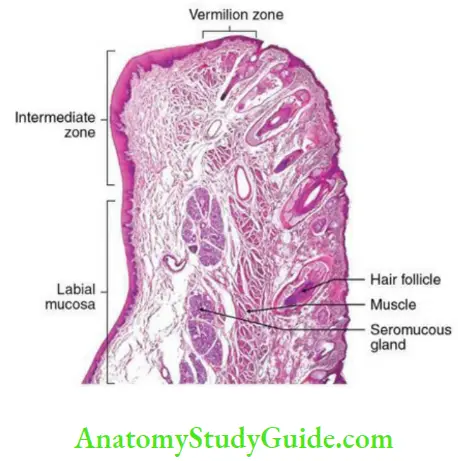
The upper and lower lips form the external boundary of the oral cavity and are the areas where the oral mucosa meets the skin of the face, the mucocutaneous junction. Each lip constitutes of
- An inner surface lined by nonkeratinized oral mucosa (labial mucosa)
- An outer surface lined by keratinized epithelium of the skin (epidermis) which are continuous with each other.
The transition from labial mucosa to epidermis is not abrupt but shows a zone of transition which is known as the vermilion zone of lip. The line that separates this zone from epidermis is known as the vermilion border. Each of the three regions of the lip is distinct clinically and histologically.
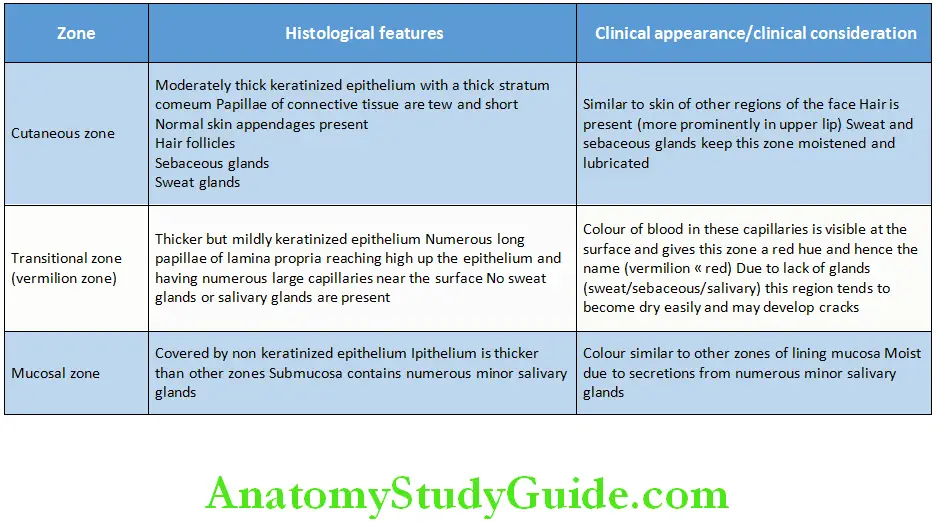
Histological and Clinical Characteristics of Various Zones of the Lip
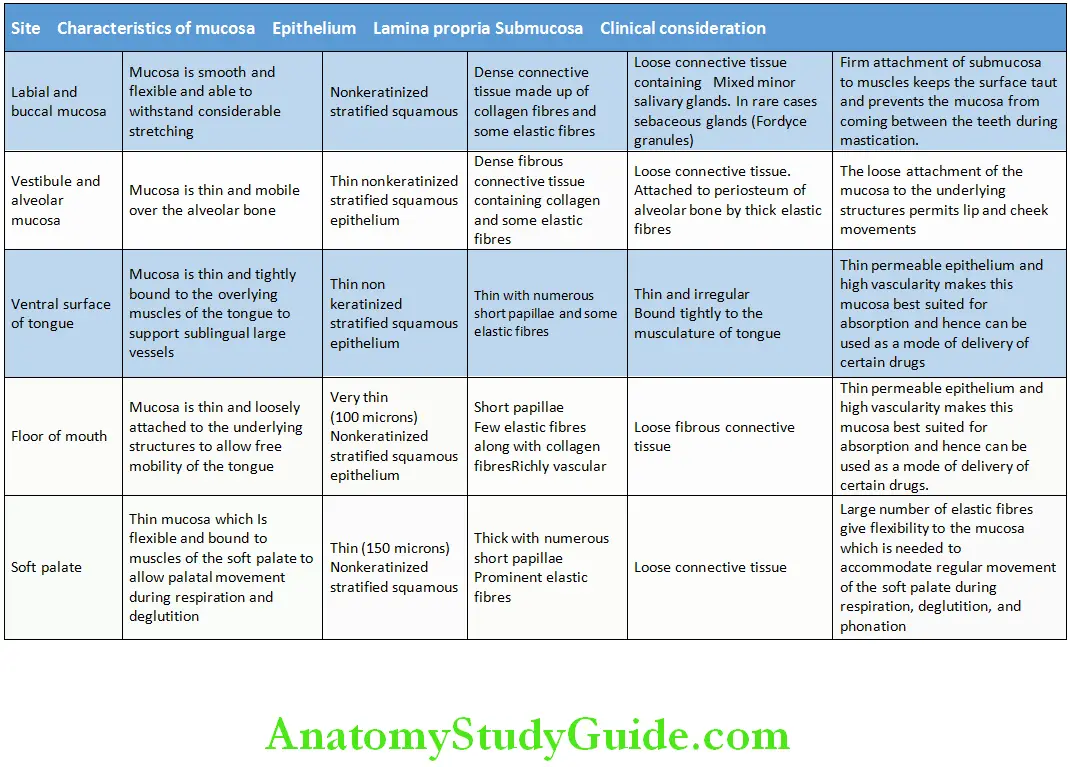
Lining Mucosa:
The lining mucosa is elastic and covers the musculature and is fixed to the fascia. This allows the mucosa to maintain a smooth surface during movement of the muscles.
Area:
- Lip
- Cheek
- Vestibular fornix
- Alveolar mucosa
Epithelium:
- Thick nonkeratinized epithelium
Connective tissue:
- Thin lamina propria
Submucosa:
- Loosely textured in the lips, cheeks and tongue to the alveolar bone
- Loose and of considerable volume in the reflectory mucosa in the
vestibular fornix and sublingual sulcus - The loose attachment of the mucosa to the underlying structures
permits movements of the lip and cheeks
Rest of the nonkeratinized areas are:
- Labial and buccal mucosa
- Vestibule and alveolar mucosa
- Ventral surface of tongue
- Floor of mouth
- Soft palate
The features are mentioned in Table.
Nonkeratinized Areas of the Oral Cavity:
Dorsal Surface Of Tongue (Specialized Mucosa)
The superior surface of the tongue is irregular and rough.
- The anterior part of the tongue is called the papillary and the posterior part is called the lymphatic part of the dorsolingual mucosa. The anterior and the posterior parts are separated by a V-shaped line.
- The mucosa covering anterior two-thirds of the dorsal surface of the tongue is unique and markedly different from anywhere else in the body and performs a specialized function of taste sensation and hence called the specialized mucosa.
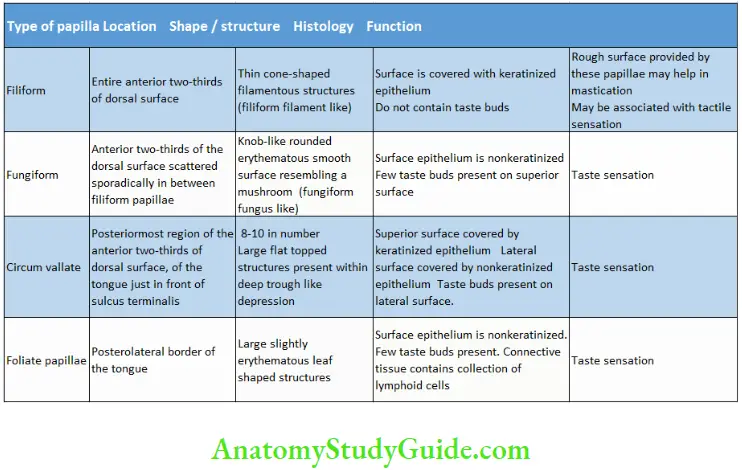
The dorsum of the tongue shows rough surface with numerous thin projections called the lingual papillae which are of four types.
- Filiform
- Fungiform
- Circumvallate
- Foliate
Papilla of the Tongue


Taste Buds
They are specialized to perceive the sensation of taste
Location:
- Papillae of the tongue
- Also seen in the posterior portion of the palate, uvula, epiglottis
Microscopic features:
- These are oval- or barrel-shaped intraepithelial organs that extend from the basal lamina to the epithelial surface containing 30–50 modified epithelial cells.
- About 40 microns in diameter and 80 microns height.
The outer surface is covered by few flat epithelial cells except a small opening called the taste pore. (More than one taste pore may be present in one taste bud). - Four types of cells are seen in the taste buds (Table 8.14).
Cells of the Taste Buds:
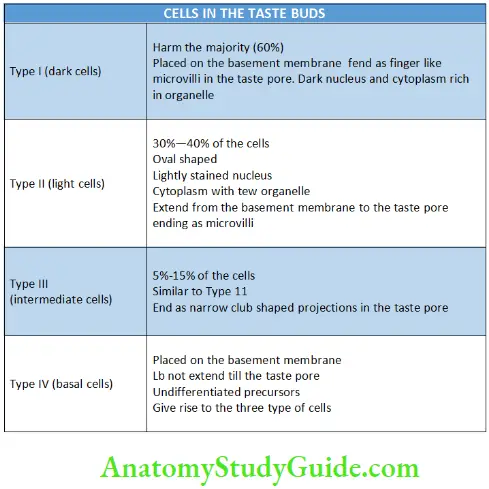
A rich neural plexus is found below the taste buds that penetrate the basal lamina and enter the taste buds.
Classic view of perception of taste:
- Sweet – tip of the tongue – fungiform papilla
- Salty – lateral border of the tongue – fungiform papilla
- Bitter and sour – palate and posterior part of the tongue – vallate and foliate
- Bitter in the middle and sour in the lateral part of the tongue
Bitter and sour – glossopharyngeal nerve
Sweet and salty – chorda tympani
Lingual tonsils:
The collection of lymphoid follicles in the posterior one-third of the tongue is called the lingual tonsils. The follicles are deep crypts which are lined by stratified squamous epithelium and contain lymphoid material. The follicles open onto the superior surface of the tongue. Ducts of mucous glands open into the crypts.
Gingival Sulcus
This is also called gingival crevice.
It is the invagination made by the gingiva as it joins with the tooth surface.
- If seen in longitudinal section it is a ‘V’-shaped space with one arm of the V made by gingival soft tissue and other arm by tooth (usually enamel). At the base of the sulcus, the gingiva meets the tooth and this area is called the dentogingival junction.
Extent:
- Free gingival margin to the dentogingival junction
Depth:
- It is considered absent in healthy, plaque-free gingiva in germ-free animals.
- In a healthy state, the depth corresponds to the level of the free gingival groove on the outer surface of the gingiva.
Clinical Consideration:
- If the depth exceeds 3 mm when clinically measured, then it is considered a periodontal pocket
Epithelium
- The sulcular epithelium is nonkeratinized and thinner than the gingiva.
- It lacks epithelial ridges and thus has a smooth interface with the lamina propria.
- It is continuous with the gingival epithelium and the attachment epithelium.
Dentogingival Junction
- The junction between the tooth and the gingiva is called the dentogingival junction.
- The epithelium of the gingiva attached to the tooth is called the junctional or attachment epithelium.
- The mode of attachment between the epithelium and the tooth is called the epithelial attachment.
Junctional epithelium:
- Junctional epithelium is a collar of epithelial cells surrounding the tooth and extending from the region of the CEJ to the bottom of the gingival sulcus. It may extend for about 2 mm.
- It is derived from the reduced enamel epithelium.
- It is 15–30 cell thick coronally and 1–3 cell thick apically.
- It has a layer of cuboidal cells overlying multiple layers of flat cells.
- It has high turnover rate of about 5–6 days and also high permeability.
- Lymphocyte and plasma cells in the connective tissue at the bottom of the gingival crevice and junctional epithelium help in defence.
Epithelial attachment:
- The cells of the junctional epithelium are attached to the tooth by means of hemidesmosomes and a basal lamina called the attachment apparatus or the epithelial attachment.
- The basal lamina towards the tooth surface is called the internal basal lamina.
- The basal lamina between the junctional epithelium and the lamina propria is called the external basal lamina.
- The internal basal lamina lacks
- Laminin
- Type IV collagen
- Anchoring fibrils
Development of the dentogingival junction:
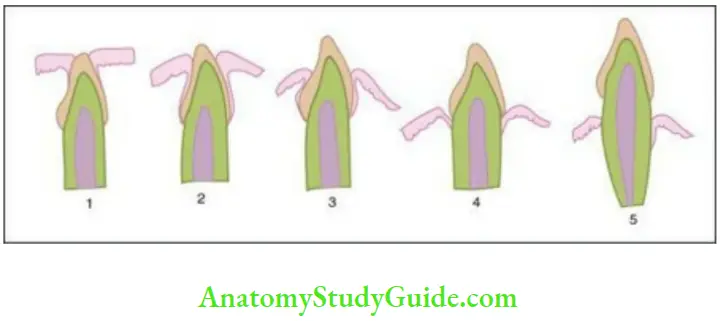
- After the formation of the enamel, the reduced enamel epithelium(REE) covers the enamel surface and is attached to the primary enamel cuticle and extends till the CEJ.
- The tooth approaches the oral epithelium as it erupts. The oral epithelium fuses with the REE. Degeneration of the epithelium covering the tip of the tooth occurs and the crown erupts through this perforation.
- The REE remains attached to the portion of the enamel that is yet to erupt. The REE is now called the primary attachment epithelium.
- The attachment epithelium is continuous with the oral epithelium at the margin of the gingiva. The REE grows shorter with eruption of the tooth and is replaced by the oral epithelium.
- A groove begins to develop between the gingiva and the tooth surface all around the tooth called the gingival sulcus. This is bounded at the base by the attachment epithelium and laterally by the gingival margin.
- As the REE separates from the tooth, the groove deepens and the gingiva surrounding the sulcus becomes the free or marginal gingiva.
Shift of the dentogingival junction:
- The entire enamel is covered by epithelium when the tip of the enamel emerges into the oral cavity.
- The attachment epithelium gradually separates from the enamel surface as the crown erupts into the oral cavity.
- The epithelium separates rapidly from the tooth surface after the tip of the crown appears into the oral cavity. The separation slows down as the tooth occludes with the opposing tooth.
- One third to one-fourth of the enamel is still covered by gingiva as the tooth first reaches occlusion. The exposure of rest of the crown follows gradually.
- The separation of the primary attachment epithelium from the enamel surface is called passive eruption. Further recession to expose the cementum occurs. The REE is gradually lost and replaced by the cells of the oral epithelium. This primary attachment epithelium is now replaced by the gingival epithelium and is called the secondary attachment epithelium.
Shift of the Dentogingival Junction:
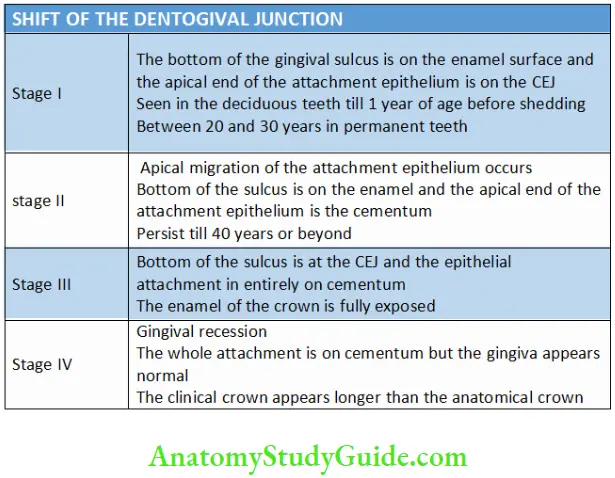
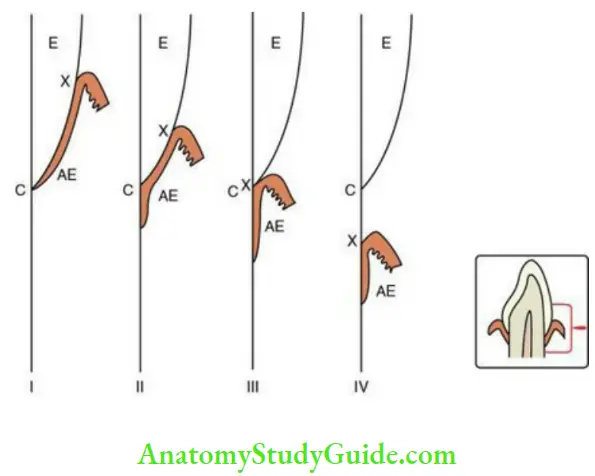
- The migration of the attachment epithelium in an apical direction occurs in four stages:
- The first two stages are considered normal but the last two stages may be considered pathological.
- In stage I and II, the clinical crown is shorter than the anatomical and vice versa in stage IV.
- The anatomical crown is equal to the clinical crown in stage III.
Dental cuticle:
The oral epithelium replaces the ameloblasts to form the secondary cuticle. The proliferation of the epithelium beyond the CEJ extends the cuticle along the cementum. The secondary cuticle and the cemental cuticle are called the dental cuticle.
Development Of The Oral Mucosa
- It is derived from the ectoderm and the endoderm.
- The epithelium lining the anterior part of the oral cavity is from the ectoderm.
- The structures derived from the pharyngeal arches derive their epithelium from the endoderm. These include tongue, epiglottis and pharynx.
- Sixth week: Separation of the vestibular lamina from the primary epithelial band. Cells in the central part of this process degenerate and form the labial and buccal sulcus.
- Seventh week: Lingual papilla appears.
- 10–12 weeks: Vallate, foliate and filiform papilla in order of appearance.
- 13–20 weeks – Keratinized and nonkeratinized mucosa can be distinguished.
- Lamina propria
- 6–8 weeks: Reticular fibres
- 8–12 weeks: Collagen fibres
- 17–20 weeks: Elastic fibres
Age Changes In Oral Mucosa
- Decrease in thickness of the oral epithelium with decrease in prominence of rete ridges.
- Decrease in number of filiform papillae on the tongue.
- Decrease in the number of Langerhans cell in the oral epithelium which leads to decreased immune response.
- Decrease in activity of salivary glands leading to dryness of the mouth.
- Some individuals complain of decreased taste sensation in old age possibly due to decreased functioning of taste receptors.
- Fordyce’s granules:
- Although sebaceous glands are not normally found in the oral mucosa sometimes ectopic collection of sebaceous glands are found in buccal or labial mucosa of some individuals. These clinically appear as small creamish yellow papules on the mucosa and are known as Fordyce’s granules. These are not seen in childhood and start appearing only after puberty as development of sebaceous glands is accelerated during that period.
- Lingual varicosities:
- Prominent tortuous veins commonly seen on the ventral surface of the tongue of older adults possibly age-related decrease in tone and elasticity of perivascular connective tissue.
Clinical Considerations
Periodontal pocket:
- Deepening of the gingival sulcus
- Injury to the junctional epithelium due to inflammation, trauma, flossing and other causes can lead to the junctional epithelium being converted to pocket epithelium. This leads to periodontitis.
- Treatment should be aimed at decreasing the pocket depth
Gingival attachment in restorations:
- In young individuals, the clinical crown is smaller than anatomical crown. It is tough to prepare such a tooth for a crown.
- The crown might have to be replaced later on
Root exposure due to recession:
- Preparation should not extend till the gingiva when recession has occurred and the roots are exposed.
- The gingival margins should be at the sulcus when the gingiva is on the enamel with an intact interdental papilla.
- In case of recession, the restoration is done after the periodontal treatment. The margins of the cavity need be carried to the gingiva.
- Gingival recession can lead to cemental exposure and cemental caries or abrasion. Further loss of cementum can expose the dentin and cause dentin sensitivity.
Variation in the submucosa:
- If the submucosa is made up of loose connective tissue, then haemorrhage and oedema may cause swelling and spread widely.
- Incision in the lining mucosa gapes as it is attached to the muscle and thus suturing is mandatory. Injections are not painful into the lining mucosa as it is easy to infiltrate.
- Incision in the masticatory mucosa do not gape due to its firm attachment to the underlying bone; but injections are painful as infiltration is tough.
Permeability of the oral mucosa:
- It varies with areas in the oral cavity.
- Rapid absorption is seen in the floor of the mouth and thus is a route for drug administration.
Healing of the oral mucosa:
- It heals faster than skin due to high vascularity and turnover rate of the epithelium.
Systemic diseases:
- Changes are seen in the oral mucosa due to certain systemic diseases.
- Koplik’s spots: Small red spots with bluish white central portion on the buccal mucosa are seen in Measles. These appear before the skin manifestations.
- Atrophy of the lingual mucosa leading to strawberry tongue: Scarlet fever
- Pernicious anaemia: Magenta tongue
- Vitamin B deficiency
Oral Mucous Membrane Synopsis
Mucous membrane can be defined as a thin moist sheet of tissue that covers or lines body cavities or canals that communicate with the exterior, such as the linings of the oral cavity, the digestive tube, the respiratory passages and the genitourinary tract.
It consists of a surface layer of epithelial tissue covering a deeper layer of connective tissue and functions to protect the underlying structure, lubricates the surface, absorbs water, salts and other solutes. Mucous membrane lining the oral cavity is called oral mucous membrane or oral mucosa.
Functions of the oral mucosa include protection, mastication, absorption, secretion and lubrication, sensory:
Based on function, it can be classified as masticatory mucosa, lining (reflecting) mucosa, specialized mucosa Based on surface keratinization, it can be classified as keratinized mucosa and nonkeratinized mucosa
Organization of oral mucosa:
The oral mucosa basically consists of two components:
- An outer covering of oral epithelium which is avascular, aneural. It insulates the underlying tissues.
- The oral epithelium is supported by connective tissue, called lamina propria, which contains the vascular and neural supply.
- Beneath the oral mucosa is a layer of loose connective tissue known as submucosa that supports the mucosa.
- In some parts of the oral cavity, the mucosa is directly attached to the periosteum of underlying jaw bone without intervening submucosa. This arrangement is called mucoperiosteum.
Oral epithelium is a multilayered epithelium arranged in a number of distinct layers or strata known as stratified squamous type of epithelium.
Surface of the epithelium may be keratinized or nonkeratinized. Keratinization itself may be of two types
- Orthokeratinization → superficial cornified cells devoid of nuclei
- Parakeratinization → superficial keratinized cells having pyknotic (degenerated) nuclei
The interface between the epithelium and underlying lamina propria. The epithelium is separated from the connective tissue by an acellular structure, the basement membrane.
Epithelial proliferation and turnover: The time taken for an epithelial cell from its formation till it is exfoliated is called the turnover time. Turnover time varies for different tissues and locations in the body.
Epithelial maturation: Maturation of the oral epithelium is characterized by progressive changes in the morphology and structure of epithelial cells as they pass through various layers of the stratified epithelium.
Keratinized epithelium: It can be divided into the following four distinct layers of variable thickness having characteristic morphological appearances – stratum basale, stratum spinosum, stratum granulosum, stratum corneum.
Nonkeratinized oral epithelium: The nonkeratinized epithelium is broadly divided into three layers based on their location – stratum basale, stratum intermedium and stratum superficiale.
Keratin: Keratins are intermediate filaments of a family of fibrous structural proteins which form the cytoskeleton of epithelial cells and are characteristic feature of these cells. These are present as filamentous strands called tonofilaments and also form integral components of desmosomes and hemidesmosomes.
Nonkeratinocytes in oral epithelium: Majority of the population of cells of stratified squamous epithelium (90%) is constituted by keratinocytes, but the epithelium also contains a small portion (about 10%) of cells which do not produce keratin and are known as nonkeratinocytes. They constitute about 10% of the total cell population of oral epithelial cells and consist of four different types of cells – melanocytes, Merkel cells, Langerhans cells and inflammatory cells
Keratinized areas of the oral cavity
Masticatory mucosa
- Hard palate
- Gingiva
Specialized mucosa
- Tongue (dorsum)
Vermilion border/zone of the lip
Hard palate: Four zones are observed in the palate due to variation in the submucosa, i.e. gingival zone, palatine raphae, anterolateral area or fatty zone, posterolateral area or glandular zone
Gingiva: The part of the oral mucosa that surrounds the neck of the tooth and covers the alveolar process is called the gingiva. The three parts are free/marginal gingiva, attached gingiva and interdental papilla. Gingival group of fibres include dentogingival, alveologingival, circular, dentoperiosteal.
Vermilion zone of lip and the mucocutaneous junction: The upper and lower lips form the external boundary of oral cavity and are the areas where the oral mucosa meets the skin of the face, the mucocutaneous junction. The transition from labial mucosa to epidermis is not abrupt but shows a zone of transition which is known as the vermilion zone of lip. The line that separates this zone from epidermis is known as the vermilion border.
Lining mucosa: The lining mucosa is elastic and covers the musculature and is fixed to the fascia. This allows the mucosa to maintain a smooth surface during movement of the muscles.
Dorsal surface of tongue (specialized mucosa): The dorsum of the tongue shows rough surface with numerous thin projections called the lingual papillae which are of four types – filiform, fungiform, circumvallate and foliate.
Taste buds: They are specialized to perceive the sensation of taste and located on the papillae of the tongue and also in the posterior portion of the palate, uvula, epiglottis. A rich neural plexus is found below the taste buds that penetrate the basal lamina and enter the taste buds. Gingival sulcus also called gingival crevice is the invagination made by the gingiva as it joins with the tooth surface.
Dentogingival junction: The junction between the tooth and the gingiva is called the dentogingival junction. The epithelium of the gingiva attached to the tooth is called the junctional or attachment epithelium. The mode of attachment between the epithelium and the tooth is called the epithelial attachment.
Junctional epithelium: It is a collar of epithelial cells surrounding the tooth and extending from the region of the CEJ to the bottom of the gingival sulcus. It may extend for about 2 mm. It is derived from the reduced enamel epithelium.
Epithelial attachment: The cells of the junctional epithelium are attached to the tooth by means of hemidesmosomes and a basal lamina called the attachment apparatus or the epithelial attachment.
Leave a Reply