Pharmacology In Endodontics Notes
Pain and periapical infections are the most common problems seen in patients with endodontic problems. Consequently, pain control and infection management are the foremost aims while performing endodontic therapy.
Table of Contents
Therefore, the use of analgesics and antibiotics has become an essential part of dental procedures for treating infections and providing pain-free procedures.
Pain Control in Endodontics
Though pain control in endodontics is not very difficult, sometimes it becomes almost impossible to control pain. Clinicians must be able to diagnose the source of pain and have strategies for its management. The “3-D” principle—diagnosis, dental treatment, and drugs—should be applied to manage pain.
Correct diagnosis of the etiological factors of pain and proper treatment of the problem relieves pain in many cases. Drugs should only be used as an adjunct to dental treatment. While performing a dental procedure, it is necessary to maintain profound anesthesia that can be achieved using local anesthetics.
Pain-management drugs include nonopioids [i.e., non-steroidal anti-inflammatory drugs (NSAIDs) and paracetamol] or opioids (i.e., narcotics). NSAIDs provide excellent pain relief due to their anti-inflmmatory and analgesic action.
Opioids are strong analgesics but have significant side effects, and therefore they should be reserved for severe pain only.
Read And Learn More: Endodontics Notes
Pain control can be achieved through:
- Local anesthesia
- Nonopioid drugs
- Opioid drugs.
Local Anesthesia Definition
It is defined as a loss of sensation in a circumscribed area of the body caused by depression of excitation in nerve endings or inhibition of the conduction process in peripheral nerves.
Purpose of Local Anesthetic:
- To stop the generation and conduction of nerve impulses
- To abort impulses from stimuli-like extraction or endodontic treatment.
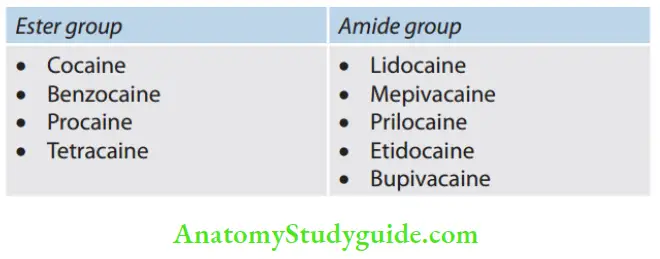
Classification of Local Anesthetic Agents
1. Based on chemical structure
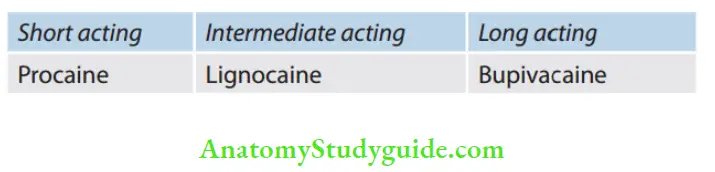
2. Based on the duration of action
Local Anesthetic Mechanism of Action:
The primary action of the local anesthetics agent is to decrease the nerve permeability to sodium (Na+) ions, thus preventing the influx of Na+ ions into the nerve. This interferes with sodium conductance and inhibits the propagation of impulse along the nerve fiers.
In tissues with lower pH, local anesthetics show a slower onset of anesthesia than in tissues with higher pH because, at alkaline pH, local anesthetic is present in an undissociated base form that penetrates the axon.
Composition of a local anesthetic agent:
- Local anesthetic—a salt form of lidocaine hydrochloride
- Vasoconstrictor—epinephrine
- Preservative for vasoconstrictor—sodium bisulfite
- Isotonic solution—sodium chloride
- Preservative—methylparaben
- Sterile water to make the rest of the volume
Intrapulpal Injection
Adequate pulpal anesthesia is required for the treatment of pulpally involved teeth. Mandibular teeth usually offer some problems in obtaining profound anesthesia. This injection controls pain, by both applying pressure and utilizing the pharmacologic action of local anesthetic agents.
Intrapulpal Injection Indications:
Lack of obtaining profound anesthesia in pulpily involved teeth by other techniques.
Intrapulpal Injection Nerves anesthetized:
Terminal nerve endings at the site of injection.
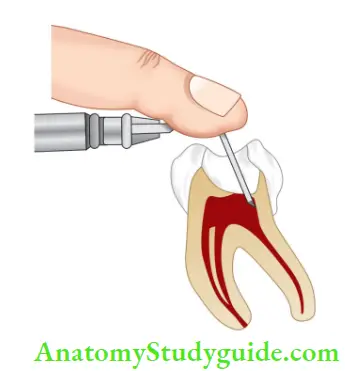
Intrapulpal Injection Technique
- Insert 25 or 27-gauge needle firmly into the pulp chamber
- Before inserting the needle, the patient must be informed that he/she may experience a brief period of sensitivity (mild to very painful) after giving the injection
- Always deposit local anesthetic solution under pressure as back pressure is shown to be the major factor in producing anesthesia
- For creating back pressure, block the access with stoppers (cotton pellet). To prevent backflow, other stoppers that can be used are gutta-percha, waxes or pieces of rubber
- Deposit a very small amount of solution (0.2–0.3 mL) under pressure (5–10 s)
- Sometimes, the bending of needle is done for gaining access to the canal.
Intrapulpal Injection Mechanism of Action:
The success of intrapulpal injection depends on the fact that it has to be administrated under pressure. Monheim suggested that prolonged pressure may lead to degeneration of nerve fiers in many instances leading to profound anesthesia for endodontic procedures.
Intrapulpal Injection Mechanism of Action Advantages
- Requires less volume
- Early onset
- Easy to learn.
Intrapulpal Injection Mechanism of Action Disadvantages
- Results are not predictable as it may vary (it should always be given under pressure).
- Taste of local anesthetic drug is not accepted by patients as it may spill during administration of intrapulpal injection.
- Brief pain during or after insertion of solution (not tolerated by some patients).
Analgesics
The main purpose of using analgesics is to eliminate the source of pain. But, at first, one must consider adjusting regimens according to the patient’s needs and response. Analgesics can be opioids or nonopioids.
Nonsteroidal Anti-inflammatory Drugs:
These are weaker analgesics but good anti-inflammatory drugs. These act primarily on peripheral pain mechanisms and also in the central nervous system (CNS) to increase the pain threshold.
Analgesics Classification
- Nonselective COX (cyclooxygenase) inhibitors
- Salicylates: Aspirin
- Propionic acid derivatives: Ibuprofen, naproxen
- Pyrrolo-pyrrole derivative: Ketorolac
- Indole derivatives: Indomethacin
- Anthranilic acid derivatives: Mefenamic acid
- Oxicam derivatives: Piroxicam, meloxicam
- Preferential COX-2 inhibitors: Diclofenac, aceclofenac, nimesulide, meloxicam
- Highly selective COX-2 inhibitors: Etoricoxib, parecoxib
- Analgesics and antipyretics with poor anti-inflammatory effect: Paracetamol (Acetaminophen).
Aspirin:
-
- Rapidly converted in the body to salicylic acid that is responsible for most of the actions
- Aspirin inhibits COX (Cyclooxygenase) irreversibly. The return of COX activity depends on the synthesis of fresh enzymes
- Analgesic action is mainly due to obtunding of peripheral pain receptors and prevention of prostaglandin mediated sensitization of nerve endings
- Absorbed from the stomach and small intestines
- Analgesic dose and antipyretic effect: 600 mg three times a day
- Anti-inflammatory dose: 3–6 g/day or 100 mg/kg/day
- Side effects:
- Gastric upset
- Irreversibly inhibits TXA2 synthesis by platelets; thus, it
interferes with platelet aggregation and prolongs bleeding time - Hypersensitivity.
- Contraindications:
- Peptic ulcer
- Bleeding disorders
- Chronic liver disease
- Pregnancy.
- Ibuprofen:
- Better tolerated alternative to aspirin
- Side effects are milder than aspirin
- Gastric discomfort, nausea, and vomiting are less than aspirin
- Dose: 400–600 mg three times a day.
Diclofenac Sodium:
- Most extensively used
- Epigastric pain, nausea, headache, dizziness, and rashes are side effects
- Gastric ulceration and bleeding are less common
- Dose: 50 mg three times a day or 100 mg sustained release once a day.
Paracetamol:
- Potent antipyretic and analgesic effects with poor anti-inflammatory activity
- Poor ability to inhibit COX in the presence of peroxides that are generated at the site of inflammation
- Well absorbed orally
- Plasma t1 2s 2 to 3 h
- Should be used cautiously in patients with liver disease or chronic alcoholics
- Preferred analgesic and antipyretic in patients having peptic ulcer and bronchial asthma
- Dose: 0.5 to 1 g three times a day.
Choice of NSAIDs in Dentistry
- Mild-to-moderate pain with a little inflmmation: paracetamol or low-dose ibuprofen
- Patients with a history of asthma: Paracetamol or Nimesulide
- Postextraction or similar acute but short-lasting pain: Ketorolac, ibuprofen, diclofenac
- Gastric intolerance to conventional NSAIDs: Etoricoxib or paracetamol
- Pregnancy: paracetamol
- Hypertensive, diabetic, ischaemic heart disease, epileptic, and other patients receiving long-term regular medication: consult a physician and consider the interaction of drugs with NSAIDs.
Opioid Analgesic Drugs:
Opioid analgesics are used to relieve acute, moderate to-severe pain. The opioid receptors are located at several important sites in the brain, and their activation inhibits the transmission of nociceptive signals from trigeminal nucleus to higher brain regions. Opioids also activate peripheral opioid receptors.
Classification
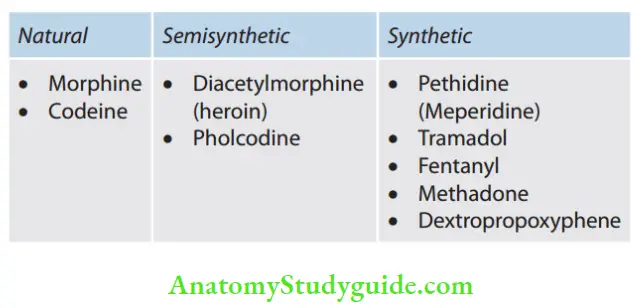
Codeine
- It is a methylmorphine.
- Occurs naturally in opium, partly converted into morphine in the body
- It is less potent than morphine. Codeine is 1/6–1/10 as analgesic to morphine.
- When compared to aspirin, it is more potent 60 mg codeine–600 mg aspirin.
Morphine
- It has site-specific depressant and stimulant actions in CNS.
- The degree of analgesia increases with the dose
- Depresses respiratory center, death in morphine poisoning is due to respiratory failure
- Oral bioavailability averages one-fourth of parenterally administered drug
- About 30% bound to plasma protein and high first pass metabolism
- Plasma t1 2 2 to 3 h
- Morphine is noncumulative
- Doses: 10–15 mg intramuscular or subcutaneous (SC).
Side effects:
Sedation, constipation, respiratory depression, nausea and vomiting
Antidote:
Naloxone 0.4 to 0.8 mg IV repeated every 2 to 3 min till respiration picks up; used in acute morphine poisoning.
Dextropropoxyphene:
- Half as potent as codeine
- Plasma t1 2s 4–12 h
- Doses: 60–120 mg three times a day.
Tramadol:
- Centrally acting analgesic; relieves pain by opioid as well as an additional mechanism
- Injected IV 100 mg tramadol is equianalgesic to 10 mg morphine
- Plasma t1 2s 3–5 h, effects last 4–6 h
- Indicated for mild to medium intensity pain due to dental or surgical procedures.
Side effects: Dizziness, nausea, sleepiness, dry mouth, sweating.
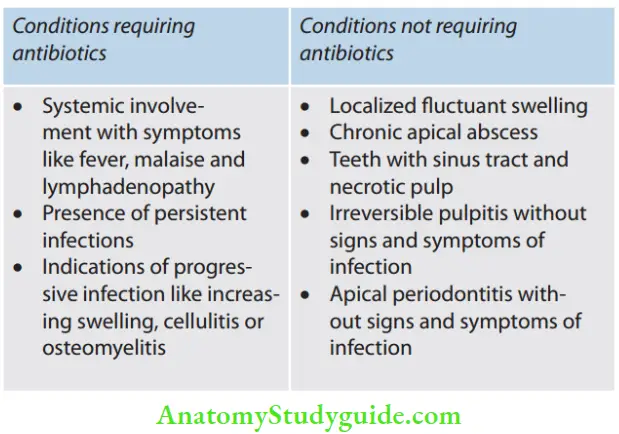
Infection Control
In general, the pulpal invasion begins with the mixed infection of aerobes and anaerobes. As the infection increases, flra changes to obligate anaerobes and facultative organisms because of oxygen depletion. One of the primary goals of endodontic therapy is to eliminate a habitat of microorganisms in canal space.
Thus, thorough sterilization is needed starting from the pulpal debridement up to the step of obturation. When drainage from the root-canal system becomes difficult to obtain or when host resistance is low or when the virulence of the attacker is high, antibiotics are needed.
Antibiotics are substances that are produced by microorganisms, which suppress or kill other microorganisms at very low concentrations. Nowadays, oral and systemic antibiotics are most frequently used; hence, a thorough understanding about their pharmacologic profie is necessary. In this topic, we will discuss the indications, uses, and side effects of the most commonly used antibiotics.
What are the principles of prescribing antibiotics?
- Use only when there is an indication.
- Choose the narrowest spectrum drug that will be effctive.
- Consider the risk/benefit equation.
- Prescribe an adequate dose with the required duration.
Reasons for failure of endodontic therapy:
- Improper drug or dose
- Bacterial resistance
- Compromised host defense
- Poor compliance.
Classification of Antimicrobial drugs
1. Based on the spectrum of activity
1. Narrow spectrum 2. Broad spectrum
- Penicillin G 1. Tetracyclines
- Streptomycin 2. Chloramphenicol
- Erythromycin
2. Types of action
- Bactericidal
- Penicillin and cephalosporins
- Metronidazole
- Fluoroquinolone
- Ciprofloxacin
- Ofloxacin
- Aminoglycosides
- Streptomycin
- Amikacin
2. Bacteriostatic
- Sulfonamides
- Tetracycline
- Clindamycin
- Erythromycin.
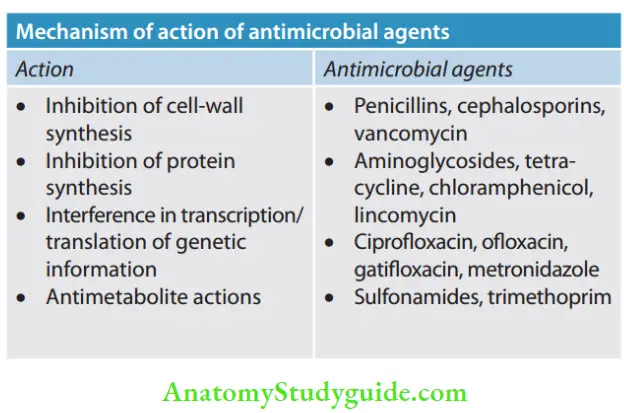
Penicillins:
- It was the first antibiotic developed and used clinically in 1941.
- Aminopencillins i.e. Ampicillin and Amoxicillin are broad-spectrum drugs effctive against Gram-positive and Gram-negative bacteria.
- Amoxicillin is one of the most frequently used antibioticsfor treatment of dental infections
- Dose of Amoxicillin – 250–500 mg t.i.d
- Amoxicillin is one of the most frequently used antibiotics for the treatment of dental infections
- Dose of Amoxicillin – 250–500 mg t.i.d
Clindamycin:
- An alternative for penicillin-allergic or penicillinresistant patients
- Active against Gram-positive and Gram-negative anaerobes and facultative/aerobic bacteria
- The dose is 150–300 mg 6 hourly.
Tetracyclines:
- This group includes tetracycline, doxycycline and minocycline which are broad-spectrum bacteriostatic antibiotics. These drugs inhibit bacterial protein synthesis
- These are useful in the treatment of periodontal disease.
Macrolides:
- This group includes erythromycin, clarithromycin, and azithromycin.
- Erythromycin was the former drug of choice for penicillin-allergic/penicillin-resistant patients, but it showed gastrointestinal adverse effects.
- It is active against Gram-positive aerobic/facultative Staphylococci, Streptococci, and Gram-negative anaerobes.
Metronidazole:
- It is highly effctive in most anaerobic infections.
- Patient should avoid alcohol during treatment with metronidazole.
- The dose is 200 to 400 mg thrice a day for or dental infections.
Antibiotic Prophylaxis Guidelines:
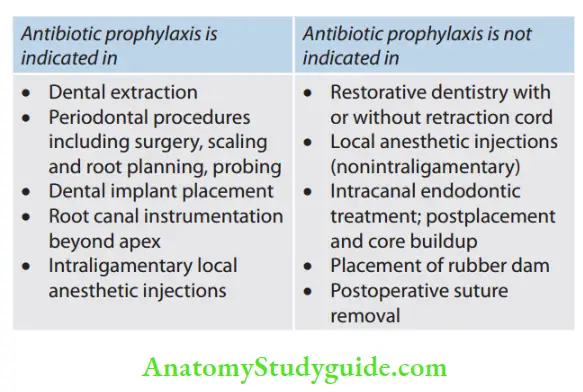
Standard antibiotic prophylaxis regimen
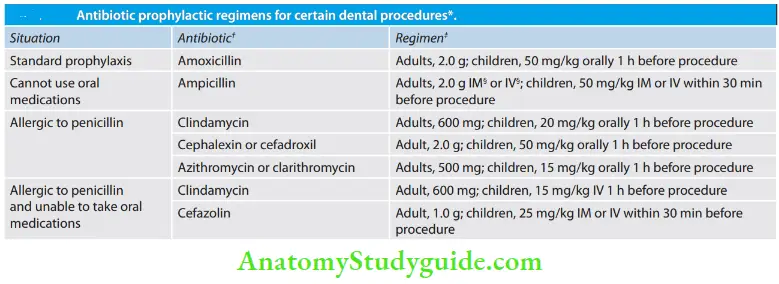
Reprinted with permission of the Journal of the American Medical Association from Dajani et al. Cephalosporins should not be used in patients with immediate-type hypersensitivity reactions (urticaria, angioedema or anaphylaxis) to penicillins. The total children’s dose should not exceed the adult dose. IM: intramuscular; IV: intravenous.
Leave a Reply