Surgical Endodontics Introduction
Root canal treatment has more than 95% of success rate but it fails if the infection remains within the root canal. To treat endodontic failure, one should attempt nonsurgical endodontic retreatment but if it is not possible, then endodontic surgery is performed to save the tooth.
Table of Contents
After case evaluation, surgical success mainly depends on careful management of hard and soft tissues, complete removal of pathognomic tissues, and final sealing of the root canal.
To check the success of the surgical procedure, a radiograph should be exposed following treatment for comparison with future radiographs to assess healing.
Read And Learn More: Endodontics Notes
Surgical Endodontics Definition
Endodontic surgery is defined as the “removal of tissues other than the contents of the root canal to retain a tooth with pulpal or periapical involvement.” Surgical intervention is required for cases where retreatment has failed or is not an option and the tooth is to be retained rather than extracted.
The first case of endodontic surgery was performed by Abulcasis in the 11th century. A root-end resection procedure to manage a tooth with a necrotic pulp and an alveolar abscess was documented in 1871 and root-end resection with retrograde cavity preparation and filing with amalgam in the 1890s.
Endodontic surgery was often considered as an alternative to root canal treatment and indications for surgery were proposed first in the 1930s. Over the past decade, periradicular surgery has continued to evolve into a precise, biologically based adjunct to nonsurgical root canal therapy.
Surgical Endodontics Rationale
The rationale of surgical endodontics is to remove the diseased tissue present in the canal and around the apex and retrofit the root canal space with biologically inert material so as to achieve a flid tight seal.
Surgical Endodontics Objectives
- Removal of diseased periapical tissue like granuloma, cyst, overfilled material, etc.
- Root inspection for knowing the etiology of endodontic failure, fracture, accessory canals, etc.
- To provide fluid tight seal at the apical end by retrograde preparation and obturation
- To eliminate apical ramifications by root resections so as to completely remove the cause of failure for endodontic treatment.
Surgical Endodontics Indications
- Need for surgical drainage
- Failed nonsurgical treatment:
- Irretrievable root canal filling material
- Irretrievable intraarticular post
- Continuous postoperative discomfort
- Recurring exacerbations of nonsurgical endodontic treatment
- Calcific metamorphosis of the pulp space
- Horizontal fracture at the root tip with associated periapical disease
- Procedural errors:
- Instrument separation
- Non-negotiable lodging
- Root perforation
- Severe apical transportations
- Symptomatic over filing
- Anatomic variations
- Root dilacerations
- Apical root fenestrations
- Non-negotiable root curvatures
- Biopsy
- Corrective surgery
- Root resorptive defects
- Root caries
- Root resection
- Hemisection
- Bicuspidization
- Replacement surgery
- Intentional replantation
- Post-traumatic replantation
- Implant surgery
- Endodontic implants
- Osseointegrated implants.
- Exploratory surgery.
Surgical Endodontics Contraindications
- Periodontal health of the tooth: Tooth mobility and periodontal pockets are two main factors affecting the treatment plan
- Patients health considerations:
- Leukemia or neutropenia in an active state leads to more chances of infection after surgery and impaired healing
- Uncontrolled diabetes mellitus: Defective leukocyte function, and defective wound healing commonly occurs in severe diabetic patients
- Recent serious cardiac or cancer surgery
- Very old patients: Old age is usually associated with complications like cardiovascular or pulmonary disorders, decreased kidney functions, and liver functions
- Uncontrolled hypertension
- Uncontrolled bleeding disorders
- Immunocompromised patients
- Recent myocardial infarction or patient taking anticoagulants
- Patients who have undergone radiation treatment of the face because in such cases incidence of osteoradionecrosis and impaired healing is high
- Patient in first trimester of pregnancy: It is during this period, the fetus is susceptible to insult, injury, and environmental influences that may result in postpartum disorders
- Patient’s mental or psychological status:
- The patient does not desire surgery
- Very apprehensive patient
- Patients unable to handle stress for long complicated procedures
- Surgeon’s skill and ability: Clinicians must be completely honest about their surgical skills and knowledge. Beyond their abilities, the case must be referred to an endodontist or oral surgeon
- Anatomic considerations such as in mandibular second molar area:
- Roots are inclined lingually
- Root apices are much closer to the mandibular canal
- Presence of too-thick buccal plate
- Restricted access to the root tip
- Short root length in which removal of root apex further compromises the prognosis
- Proximity to nasal floor and maxillary sinus: A careful surgical procedure is required to avoid surgical perforation of the sinus
- Miscellaneous
- Nonrestorable teeth
- Poor periodontal prognosis
- Vertically fractured teeth
- Nonstrategic teeth.
Surgical Endodontics Classifiation
1. Surgical drainage
- Incision and drainage (I and D)
- Cortical trephination (fistula surgery
2. Periradicular surgery
- Curettage
- Biopsy
- Root-end resection
- Root-end preparation filing
- Corrective surgery
- Perforation repair
- Mechanical (iatrogenic)
- Resorptive (internal and external)
- Root resection
- Hemisection
- Perforation repair
3. Replacement surgery
4. Implant surgery
- Endodontic implants
- Root-form osseointegrated implants.
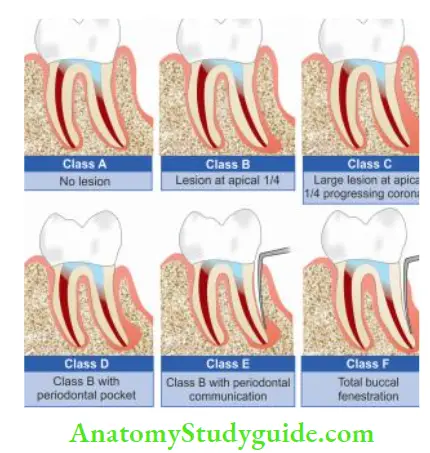
Classifiation of Endodontic Microsurgical Cases
Given by Richard Rubenstein and Kim according to the assessment of root form osseous integrated implant treatment outcome.
- Class A: Absence of periradicular lesion but persistent symptoms after nonsurgical treatments.
- Class B: Presence of small periapical lesion and no periodontal pockets.
- Class C: Presence of large periapical lesion progressing coronally but no periodontal pockets.
- Class D: Any of Class B or C lesion with a periodontal pocket.
- Class E: Periapical lesion with endodontic and periodontal communication but no root fracture.
- Class F: Tooth with periapical lesion and complete denudation of buccal plate.
Leave a Reply